
Abstract
Background:
Hazelnut represents one of the most important food allergens. Yet, sensitization to hazelnut is often randomly detected during routine diagnostic workup without a clear-cut history of allergy. The aim of this study was to assess the diagnostic usefulness of recombinant hazelnut components and whole hazelnut extract for the prediction of clinical reactivity in sensitized children.
Methods:
Fifty-three consecutive children were investigated who underwent oral food challenge (OFC) due to positive in vitro test results and/or cutaneous reactions after hazelnut ingestion. Determination of specific immunoglobulin E (sIgE) against allergen extracts and recombinant hazelnut components had been performed in all patients prior to OFC.
Results:
OFC revealed hazelnut allergy in 19 children (36%). At a mean total IgE of 518 kU/L, sIgE to hazelnut extract was significantly higher in allergic than in tolerant children (38 vs. 13 kU/L). In contrast, no significant difference in sIgE levels against allergen components was detected. A ratio of rCor a 1 to hazelnut extract sIgE levels >1 predicted hazelnut tolerance with a sensitivity and a negative predictive value of 100%. The corresponding specificity (47%) and positive predictive value (51%) were low.
Conclusions:
In the present study, a ratio of rCor a 1 to hazelnut extract sIgE >1 predicted hazelnut tolerance during OFC in children with suspected hazelnut allergy. However, further investigations in larger populations are warranted to investigate the transferability of these results to other patient populations. Until then, OFC remain the diagnostic gold standard for the definitive diagnostic workup of suspected food allergy.
Introduction
H
In these clinical situations, only controlled oral food challenges (OFCs) can clarify the actual relevance of previously positive in vivo and/or in vitro test results. However, OFCs are time-consuming, costly, and not without a certain risk of severe reactions, even if performed in experienced centers. 2 As a consequence, several clinical research groups have utilized the in vitro approach of component-resolved diagnostics (CRD) with the aim of identifying those patients at increased risk of systemic reactions upon allergen exposure. In brief, CRD comprises the additional laboratory determination of specific immunoglobulin E (sIgE) antibodies against single allergenic molecules rather than to whole allergen extracts alone. Once the patient's IgE recognition pattern against these food allergen components has been established, the association of the obtained individual sensitization profile with clinical parameters, especially symptoms and clinical severity of challenge reactions, can be evaluated. 3
In this context, most data exist for patients with peanut allergy. In particular, Ara h 2 is a peanut seed-storage protein with a high stability to degradation from heat and digestion. It has been shown that the detection of sIgE to recombinant (r) Ara h 2 is associated with a reasonably high probability of clinical reactions during peanut OFC.2,4–7
Intriguingly, the sIgE recognition pattern to single allergen components in hazelnut-sensitized patients seems to be more complex. Accordingly, sIgE against the recombinant hazelnut proteins rCor a 9, rCor a 14, and rCor a 8 is potentially associated with severe anaphylactic reactions in hazelnut-allergic individuals.8–15 Sensitization to rCor a 9 and rCor a 14 has been shown to predict allergy to hazelnut in adults and older children to some extent. 15 Nevertheless, many tolerant individuals are clearly sensitized to Cor a 9 and Cor a 14.13,15 Besides these allergenic proteins, various other allergen components have been described as possible biomarkers of an elevated risk for severe allergic reactions. 13 Yet, this allergen panel also renders prediction of probable reaction types rather difficult, because many serum parameters would have to be measured simultaneously to obtain the complete sIgE profile. Thus, the present study aimed to investigate the clinical usefulness of a single, commercially available hazelnut component (rCor a 1) and whole hazelnut extract for the in vitro prediction of clinical reactivity in hazelnut-sensitized children in Germany.
Materials and Methods
Patient selection
All children who underwent an OFC with hazelnut in our hospital between May 2009 and August 2012 were included in this investigation. A thorough medical history of each patient was taken by a pediatric allergologist using a standardized questionnaire. Only children with an IgE-mediated sensitization to hazelnut were included and allocated to either group A (no known previous ingestion of hazelnut) or group B (history of mild, cutaneous reactions after hazelnut ingestion within the last 2 years). Patients with a history of full-blown hazelnut anaphylaxis with additional extracutaneous symptoms did not undergo OFC and were excluded from further analysis.
This study was approved by the local ethics committee, and parents gave their informed consent for participation.
OFCs
In both groups, OFCs followed standardized protocols and were performed in either a double-blind, placebo-controlled or an open manner. The choice of challenge mode depended on the pretest probability of subjective symptoms as estimated by the investigator team after obtaining a thorough medical history.
OFCs were carried out on an inpatient basis with children receiving paste made from hazelnuts that had been dried at 100°C according to the manufacturer's information. The OFC dosing steps were 5 mg, 10 mg, 50 mg, 100 mg, 500 mg, 1,000 mg, and 5,000 mg, resulting in a cumulative dose of 6.65 g per hazelnut challenge. Incremental doses were administered at 30 min intervals if no subjective or objective symptoms occurred. After development of objective symptoms, the challenge was immediately stopped. Likewise, the challenge was also rated positive if repetitive or severe subjective symptoms occurred such as abdominal cramps, nausea, marked irritability, a sudden feeling of pending doom, or severe oral allergy syndrome with throat tightness.
Allergen-specific IgE detection
Prior to OFC, IgE serum levels were measured using a commercially available fluorescence enzyme immunoassay (ImmunoCAP; Phadia/Thermofisher, Freiburg, Germany) with a lower detection limit of 0.1 kU/L and an upper detection limit of 100 kU/L. Besides total serum IgE (tIgE), sIgE against hazelnut and birch extract as well as against rCor a 1 was determined. A ratio of sIgE was calculated, dividing sIgE to rCor a 1 by hazelnut extract.
Statistics
Descriptive statistics were used to analyze demographic data and reaction patterns, whereas Mann–Whitney rank sum tests were used for group comparisons. All statistical analyses and graph plots were performed with SigmaPlot for Windows v11.0 (Systat Software GmbH, Erkrath, Germany) and Medcalc v12.4.0 (Medcalc Software bvba, Ostend, Belgium).
Results
Patients
A total of 53 patients (38% female) entered the current study, corresponding to the entire population of children with suspected hazelnut allergy who had been referred to our clinic for oral provocation testing from May 2009 to August 2012 (Table 1). Thirty-three of the included children (62%) underwent OFC because of hazelnut-specific sensitization without any known prior hazelnut ingestion (group A). In contrast, 20 individuals (38%) had previously developed mild to moderate symptoms (pruritus, urticaria, angioedema) after hazelnut consumption (group B).
Percentage in population of OFC-positive patients.
Ratio of rCor a 1- and hazelnut-specific sIgE serum levels.
SD, standard deviation; OFC, oral food challenge; sIgE, specific immunoglobulin E.
At a mean age of 64±40 months (range 14–171 months), a clear majority of children (74%) presented with current or previous episodes of AD diagnosed in accordance with Hanifin and Rajka's criteria. Thirty-five children (66%) suffered from challenge-proven allergy against at least one of the following food allergens: peanut (n=15), egg (n=11), walnut (n=4), and cow's milk (n=2), as well as soy, fish, lentil, celery, sesame, kiwi, sunflower seed, and poppy seed (n=1, respectively). Additionally, 16 patients (47%) were affected by physician-diagnosed allergic rhinoconjunctivitis and extrinsic asthma, whereas isolated allergic rhinoconjunctivitis or extrinsic asthma occurred in 9 (17%) and 8 (15%) individuals, respectively. These 33 children with inhalant allergy revealed sensitizations against one or more of the following indoor and outdoor allergens: birch (n=25) and grass (n=18) pollen, house dust mite (n=13), animal epithelia (n=7), molds (n=6), and mugwort pollen (n=4).
Challenge outcomes
OFC confirmed hazelnut allergy in 5 girls and 14 boys (i.e., 36% of the study population), undergoing provocation tests at a mean age of 64 months (range 14–168 months). With regard to the clinical status of these 19 OFC-positive children, atopic comorbidities consisted of AD, allergic rhinitis, and asthma in 15 (79%), 11 (58%), and 7 (37%) individuals, respectively. Fourteen patients (74%) had previously revealed allergies against at least one food allergen other than hazelnut, mostly peanut (n=7) and hen's egg (n=6).
In group A, 9 of 33 children (27%) reacted during hazelnut challenge. Six of these individuals revealed cutaneous symptoms, whereas additional pulmonary (dyspnea) and gastrointestinal symptoms (abdominal cramps, nausea, vomiting) were noted in four patients. In group B, 10 of 20 children (50%) showed similar positive reactions, consisting of cutaneous as well as additional respiratory and gastrointestinal complaints in two and three patients, respectively. As a cardiocirculatory symptom, a moderate drop in blood pressure was recorded in one patient in group B.
In line with these mostly mild to moderate OFC reactions, seven patients fully and rapidly recovered without any specific treatment. The other 12 children received systemic antiallergic treatment consisting of an intravenous H1-antihistamine (dimetindene maleate). Seven of these patients received additional systemic glucocorticosteroid therapy (prednisolone), which was combined with salbutamol inhalations in three children due to additional cough and/or mild dyspnea. One single patient received epinephrine inhalations because of inspiratory stridor, while no child had to be treated with intramuscular or intravenous epinephrine.
Serologic parameters
At a mean total serum IgE of 518±737 kU/L, tIgE levels of the entire study population revealed marked interindividual variability ranging from 15 kU/L to 2,768 kU/L. Analyzed separately, tIgE levels in groups A and B (508±727 kU/L vs. 525±758 kU/L) did not differ significantly (p=0.7). Likewise, there was no significant difference between both groups with regard to sIgE serum levels against whole hazelnut extract (p=0.8), birch extract (p=0.6), and rCor a 1 (p=0.5).
Stratifying sIgE levels according to OFC outcome, hazelnut extract-specific IgE levels were significantly higher (p=0.004) in patients with challenge-proven allergy (38±35 kU/L; range 0.9–100 kU/L) as compared to tolerant children (13±9 kU/L; range 0–94 kU/L). In contrast, neither tIgE levels nor birch extract or rCor a 1 sIgE levels differed significantly between both groups (p>0.5; Fig. 1).
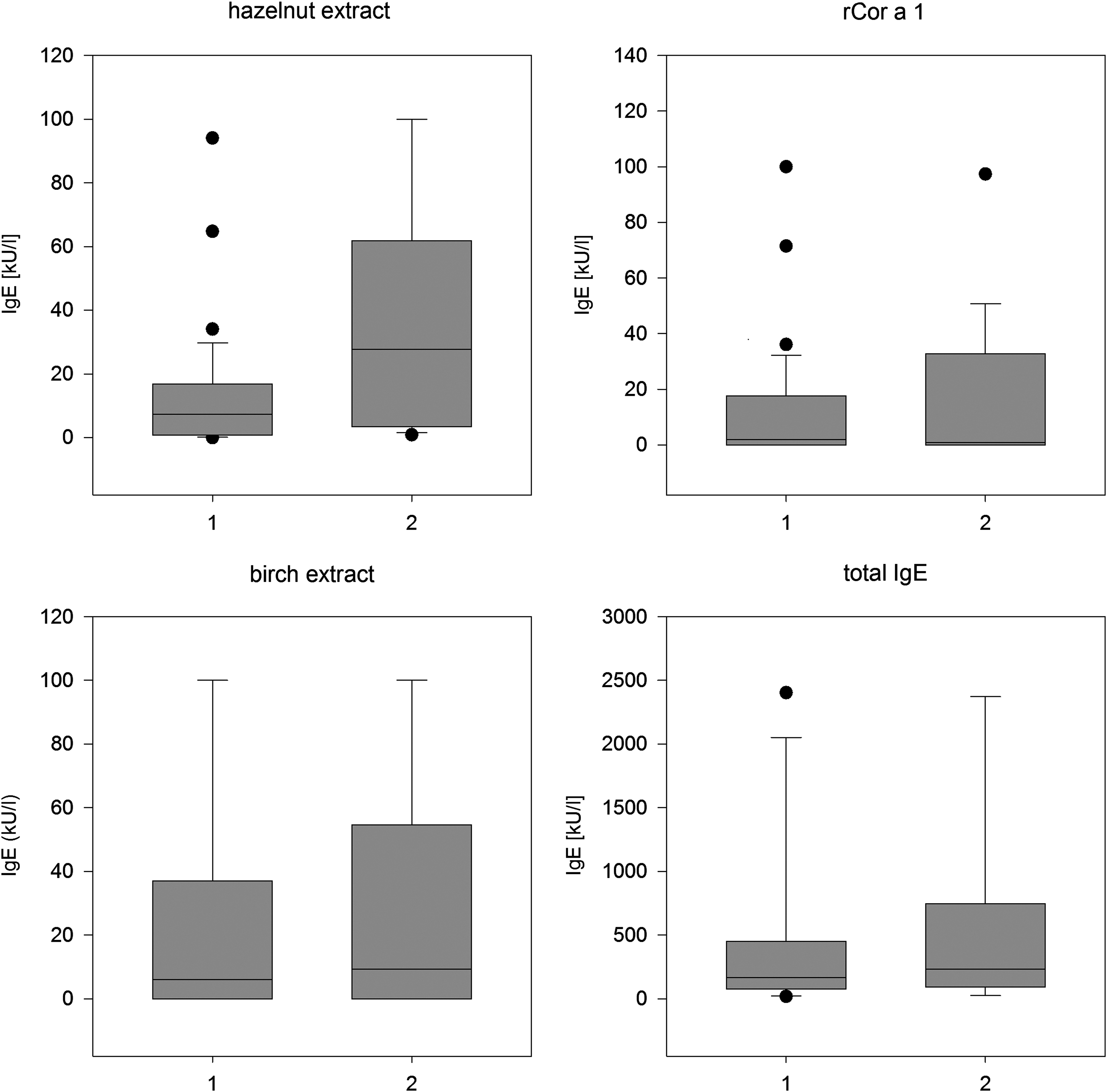
Box-and-whisker plots of total and allergen-specific serum immunoglobulin E levels in oral food challenge (OFC)-negative (1) and OFC-positive (2) children. The length of each box corresponds to the respective interquartile range (25th to 75th percentile); horizontal lines represent the median. Vertical lines (whiskers) extend from the 10th to the 90th percentile; black dots depict outliers.
Additional calculation of the ratio of rCor a 1- and hazelnut-specific sIgE levels disclosed distinct patterns in OFC-positive and OFC-negative patients. Whereas 16 OFC-negative children revealed a ratio >1, all OFC-positive patients showed ratio levels <1 (Table 2). The corresponding diagnostic test evaluation yielded a very high sensitivity (100%, confidence interval [CI] 82.2–100%) and negative predictive value (100%, CI 79.2–100%) of a component- to extract-sIgE ratio >1. In contrast, both specificity (47%, CI 29.8–64.9%) and positive predictive value (51.4%, CI 34.4–68.1%) of this threshold were low.
Discussion
Establishing a definite diagnosis of hazelnut allergy remains an important clinical challenge, especially in pediatric patients without a clear-cut history of severe anaphylaxis. Moreover, it has recently been shown that medical history alone is not sufficient to predict reaction patterns upon re-exposure to hazelnut. For example, Masthof et al. 14 demonstrated that reported allergic reactions after accidental hazelnut ingestion had a positive predictive value of only 59%, which corresponds very closely to the 50% of children with a positive history but negative OFC included in the present study. This further corroborates that in order to avoid unnecessary elimination diets, a thorough diagnostic workup including OFC should be undertaken in all children with suspected food allergy. On the other hand, the rate of positive OFC in recruited children with a sensitization to hazelnut, but without any known previous hazelnut ingestion, was as high as 27% in the present study. As a consequence, it is strongly recommended that the first exposure of sensitized patients to potential food allergens should take place in an adequate medical setting allowing for immediate emergency management.
In this context, CRD aims to help the clinician in the assessment of sensitized patients, mainly with regard to their risk of clinical reactivity and their potential for cross-reactions. Providing sIgE recognition patterns to single molecules, CRD has the potential to disclose serologic predictors of allergic reactions. This has been particularly pointed out for young children with peanut allergy in whom rAra h 2 seems to be a useful biomarker, at least if present at values >1.2 kU/L. 2 In hazelnut-sensitized patients, the pollen-independent seed-storage proteins rCor a 9 and rCor a 14 have been used to predict clinical allergy. 15 Yet, in the pediatric age group, a significant number of patients has been described who were tolerant to hazelnut despite sensitization to rCor a 9 and/or rCor a 14. 15 This makes merely serological predictions of the individual patient's tolerance unreliable and further stresses the significance of OFC in daily clinical practice. As neither rCor a 9 nor rCor a 14 proteins were commercially available at the time of the current investigation, this important aspect could not be investigated any further.
In accordance with the results of a study by Masthoff et al., sIgE to hazelnut major allergen rCor a 1 alone did not sufficiently predict the clinical relevance of hazelnut sensitization in the present study. Likewise, the statistically significant difference between sIgE levels against whole hazelnut extract in OFC-positive and OFC-negative patients was of little clinical use in the current patient population because some tolerant individuals revealed very high sIgE levels, whereas some allergic children were not sensitized to hazelnut extract at all. As a consequence, serological diagnosis based on rCor a 1- or hazelnut extract-specific IgE cannot be considered an adequate alternative to OFC.
These limitations led us the investigation of whether it was possible to predict a negative outcome of hazelnut OFC in sensitized patients by calculating the ratio of sIgE against commercially available rCor a 1 and whole hazelnut extract. Intriguingly, it was found that all patients with an rCor a 1/hazelnut-ratio >1 proved to be tolerant during the standardized OFC.
Bearing in mind the high rate of positive sIgE responses to birch extract in patients in the current study, it can be speculated that the sensitization to hazelnut was predominantly based on cross-sensitization to rBet v1, the birch pollen homologue of rCor a 1. In contrast, sensitization to other highly allergenic hazelnut components such as pollen-independent seed-storage proteins would have led to ratios <1. This is in agreement with a recent publication by Asarnoj et al., who demonstrated that exclusive sensitization to rAra h 8, the rBet v 1 homologue of peanut, was associated with clinical tolerance, whereas symptom severity increased with greater diversity of sIgE responses to a broad spectrum of peanut components including seed-storage proteins.16,17 However, as already pointed out, the analysis of more comprehensive, hazelnut-specific sensitization patterns was not possible in the present study due to a lack of freely available hazelnut components suitable for in vitro allergy testing.
Furthermore, Skamstrup Hansen et al. investigated the pattern of sensitization to hazelnut components in a large group of adolescent and adult patients living in three different regions of Europe. 13 They found a huge variety of sensitizations to different epitopes in hazelnut-allergic patients. Moreover, hazelnut-tolerant but pollen-allergic patients showed no difference compared to truly hazelnut-allergic patients with regard to the frequency of sensitizations to seed-storage proteins such as rCor a 9. This emphasizes that the positive prediction of a clinical reaction in hazelnut-sensitized patients might remain difficult, even after the evaluation of sensitization to hazelnut seed-storage proteins has become commercially available.
In sum, a ratio of rCor a 1- and hazelnut-specific IgE >1 safely predicted hazelnut tolerance during OFC in pediatric patients with suspected hazelnut allergy. However, although the included children with a positive medical history of hazelnut allergy only had mild cutaneous reactions, these were presumably systemic and could have been a precursor to a more serious systemic reaction after future ingestion. In addition, the clear majority of the patient population was made up of atopic children with a high rate of concurrent sensitizations to inhalant and food allergens as well as frequent atopic comorbidities. Hence, although these findings strongly suggest that determining the rCor a1/hazelnut extract ratios may decrease the need for challenge testing, further studies performed with a broader panel of hazelnut allergen components in larger, well-defined populations are surely warranted. In particular, future investigations are needed to clarify the transferability of these results to distinct patient populations such as children with a higher anamnestic risk of anaphylaxis or children less frequently affected by IgE-mediated polysensitization and atopic comorbidities. Consequently, controlled OFCs with the culprit food allergen are still indispensable for the definite diagnosis or exclusion of hazelnut allergy.
Footnotes
Author Disclosure Statement
L. Lange and H. Ott have received speakers' fees from Phadia/Thermofisher. H. Ott has previously received an unrestricted scientific grant from Phadia/Thermofisher.