
Abstract
Background:
Adipokines have been claimed for the link between obesity and asthma. The aim of the present study was to evaluate the roles of leptin and adiponectin in children with asthma and/or obesity and their effect on pulmonary functions.
Methods:
Obese (n=71) and lean asthmatics (n=72), obese non-asthmatics (n=46), and lean healthy children (n=49) were included in the study. Serum leptin and adiponectin levels were compared according to groups and sex.
Results:
Mean leptin levels of obese asthmatics were higher than those of lean asthmatics (13.1±9.1 vs. 3.7±4.4; p<0.001). Serum adiponectin levels of lean asthmatics (16±7.1) were significantly higher than those of obese asthmatics (12.1±6.9; p<0.001) and of their lean healthy (13.2±5.9; p<0.05) counterparts. In obese asthmatics, adiponectin levels were positively correlated with the forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) ratio, and serum leptin levels were inversely correlated with forced expiratory flow (FEF25–75). Leptin/adiponectin ratio was inversely correlated with FEV1/FVC ratio in lean and obese asthmatic patients.
Conclusions:
The present findings suggest that adiponectin may have protective disease modifying effect(s) in asthmatic children. Anti-inflammatory mechanisms regarding adiponectin may work better in girls than in boys.
Introduction
I
Leptin plays a key role in the regulation of body weight, appetite, and energy balance of the body.10,11 It typically stimulates Th1 cytokine response that leads to the production of additional pro-inflammatory cytokines. Leptin and its receptors are also expressed in human airway cells, suggesting relationship between obesity and asthma. Adiponectin, which is the most abundant protein specific to adipose tissue, might play a role as an anti-inflammatory hormone. 7 Adiponectin receptors are also expressed on lung cells. However, unlike leptin, adiponectin is inversely related to obesity. 12
In the light of this information, the aim of this study was to evaluate the roles of leptin and adiponectin in children with asthma and/or obesity and their effects on the parameters of pulmonary functions.
Methods and Materials
Two hundred and thirty-eight children, who were admitted to Baskent University Hospital, Departments of Pediatric Allergy, Pediatric Endocrinology, and General Pediatrics between September 2009 and July 2010, were included in the study. All the patients with asthma were physician diagnosed. Patients were investigated in four groups: group 1, obese children with asthma; group 2, lean children with asthma; group 3, obese non-asthmatic children; group 4, lean healthy children (control group).
The study was approved by Baskent University Institutional Review Board and Ethics Committee (Project No: KA09/189) and supported by Baskent University Research Fund. Written informed consent was obtained from each subject and his/her parents.
All the children included in the study were 6–16 years of age and were assessed through physical examination. Each subject's height was measured with a standard wall-mounted stadiometer, and their weight was measured with calibrated electronic scales. Body mass index (BMI) was calculated using the weight divided by height in meters squared (kg/m2) formula. Children with a BMI >95th percentile according to age and sex were defined as obese according to the National Center for Health Statistics (www.cdc.gov). 13 Lean subjects with no history of bronchial asthma, allergic rhinitis, or other respiratory symptoms and no personal or familial history of allergic disease were selected as controls. They were otherwise healthy children, and were not using any medication.
Pulmonary function tests were performed in all asthmatics and obese children by using Flow handy ZAN 100 USB (Nspire health, GmbH, Oberthulba, Germany). Forced expiratory volume in one second (FEV1), forced vital capacity (FVC), FEV1/FVC, and the forced expiratory flow (FEF25–75) were measured. While performing spirometry, a minimum of three flow-volume loop results within 10% of each other were recorded, and the flow-volume loop with the highest FEV1 was analyzed. All results were revised based on the temperature, pressure, and saturation conditions. All asthmatic children were mild or moderate persistent asthmatics who had been using inhaled corticosteroids (either 200 μg fluticasone propionate or 400 μg budesonide). The asthmatic patients had been previously diagnosed according to the Global Strategy for Asthma Management and Prevention Classification based on a history of intermittent wheezing and demonstration of reversible airway obstruction as defined by at least a 12% improvement in FEV1 following bronchodilator administration. 14 Since the intention was to eliminate the strong anti-inflammatory effect of systemic corticosteroids, those children with a history of systemic (intravenous, intramuscular, or oral) corticosteroids within the last 6 months were excluded from the study.
Skin prick tests and total immunoglobulin E (IgE) were obtained from medical records. Total eosiniophil counts and eosinophil percentiles were obtained at the same time with serum leptin and adiponectin samples.
A serum sample was immediately frozen from each case in a −80°C freezer until enzyme-linked immunosorbent assay (ELISA) measurement. All samples were thawed at once before ELISA testing and leptin and adiponectin levels were measured according to the manufacturer's protocol. Serum leptin concentrations were measured by immunoenzymometric assay (DIA Source Immuno Assays S.A., Nivelles, Belgium). Serum adiponectin concentrations were measured by immunoenzymometric assay manufactured by BioVendor—Laboratorni Medicina a.s. (Brno, Czech Republic).
Statistical analysis
Shapiro–Wilk's test was used to assess the normality of distributions of the variables, and Levene's test was used to assess the homogeneity of variances among groups. Comparisons of group means were performed with factorial analysis of variance and Tukey HSD multiple comparison tests. In order to eliminate age effect for some variables, covariance analysis was used. Parametric test assumptions were not available for some variables. Data transformation methods were applied to these variables, and then the analysis was performed. Assumptions are still not available for some variables despite the data transformation. Therefore, comparison of the group medians for these variables was performed by Kruskal–Wallis test and Dunn multiple comparison test. Correlations between variables were evaluated by Spearman's rho correlation coefficient.
Data analyses were performed using the SPSS Statistics for Windows v17.0 (SPSS, Inc., Chicago, IL). A p-value of<0.05 was considered statistically significant. The results of the statistical analysis indicated a number of observations (n), mean±standard deviation (M±SD), median, and minimum–maximum values (min–max).
Results
A total of 238 children (120 male) were investigated in four groups: 71 obese asthmatics, 72 lean asthmatics, 46 obese non-asthmatics, and 49 lean healthy children. The clinical characteristics of participants in the study are summarized in Table 1. The comparison between obese children (117 children) and lean subjects (121 children) indicated that eosinophil percentages were significantly higher in obese asthmatics (4.2±3.7) than they were in lean asthmatics (3.2±2.4; p<0.05). The same figure was present in the comparison of obese non-asthmatics (2.8±1.7) with lean controls (1.5±1.3; p<0.05; Table 1).
p<0.001; b,fp<0.01; c,ep<0.05.
BMI, body mass index; FVC, forced vital capacity; FEV1, forced expiratory volume in one second; FEF, forced expiratory flow.
The highest leptin levels were observed in obese non-asthmatic children (17.2±1.5 ng/mL). Mean leptin levels of obese asthmatic children were significantly higher (13.1±9.1) than those in lean asthmatics (3.7±4.4; p<0.001; Fig. 1). However, there was no difference concerning the levels of leptin between lean asthmatics (3.7±4.4) and lean healthy children (3.9±4.6; Table 1). Adiponectin levels were highest in lean asthmatics (16±7.1), whereas the lowest results were observed in obese non-asthmatic children (8.2±4.4). Serum adiponectin levels of lean asthmatics (16±7.1) were significantly higher compared to both obese asthmatics (12.1±6.9) and lean healthy children (13.2±5.9; p<0.001 and p<0.05, respectively; Fig. 1).
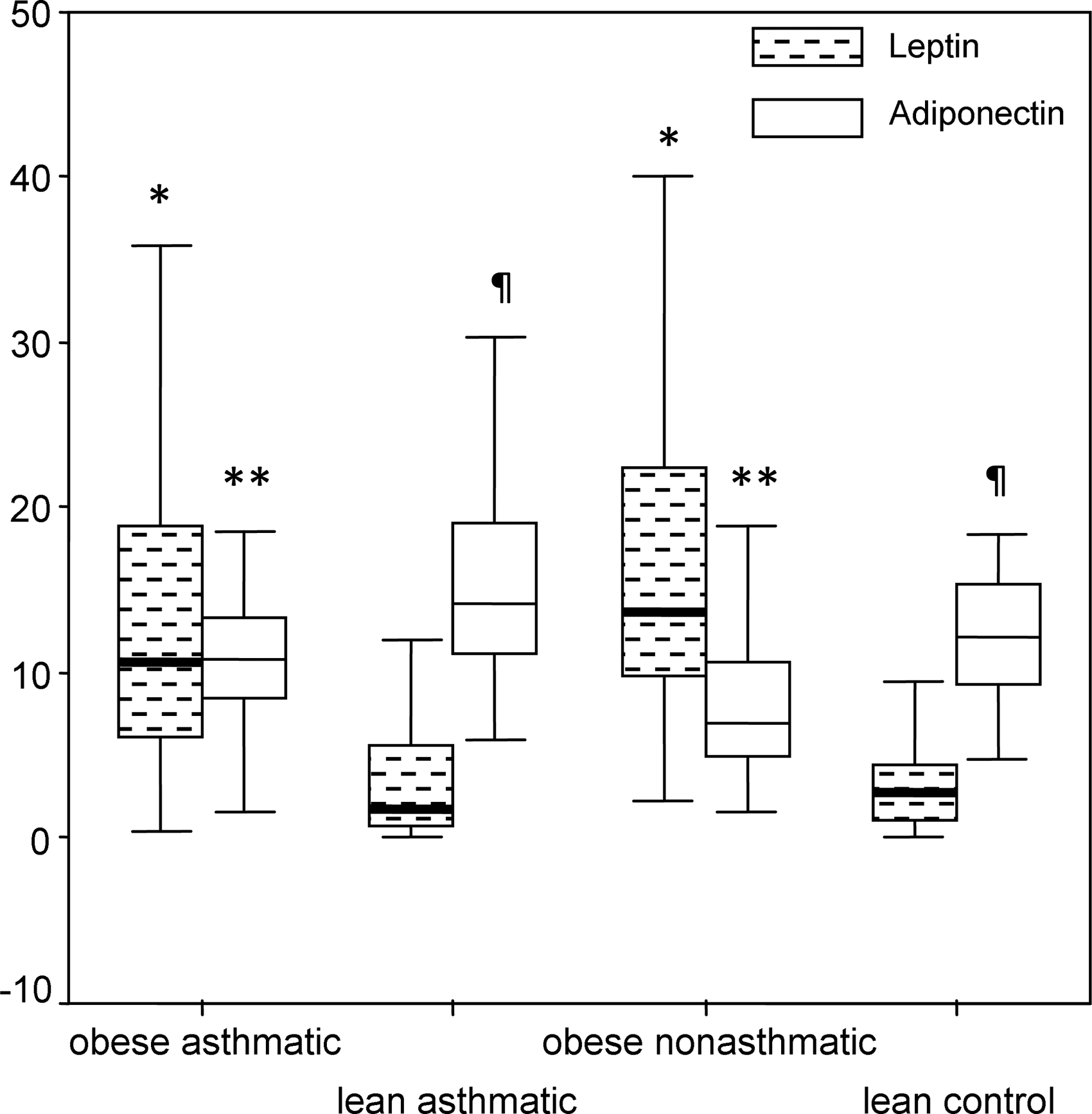
Comparison of serum leptin and adiponectin levels according to groups.
When asthmatic patients were classified according to the presence of atopy, no difference in terms of leptin and adiponectin levels was observed. With increasing age, leptin levels increased not only in obese and lean asthmatic children (p<0.01, Spearman's ρ=0.495; p<0.01, Spearman's ρ=0.484, respectively) but also in healthy controls (p<0.05, Spearman's ρ=0.323). Serum leptin levels showed a positive correlation with BMI in lean asthmatics (p<0.01, Spearman's ρ=0.671), lean healthy children (p<0.01, Spearman's ρ=0.633), and obese asthmatics (p<0.01, Spearman's ρ=0.616), whereas adiponectin levels displayed negative correlation with BMI (p<0.01, Spearman's ρ=−0.349).
Serum leptin levels of girls were higher when compared to those in boys in all groups (Table 2). Adiponectin levels of lean asthmatic girls (16.5±7.4) were significantly higher than in lean healthy girls (12.6±5.8; p<0.05; Fig. 2). When obese asthmatic and obese non-asthmatic children were compared, adiponectin levels of obese asthmatic girls (11.5±7.5) were found to be higher than in obese non-asthmatic girls (7.9±4.7; p<0.05), and adiponectin levels of obese asthmatic boys (12.5±6.4) were higher than for obese non-asthmatic boys (8.5±4; p<0.01; Table 2). The leptin/adiponectin ratio was higher in obese non-asthmatic children (2.9±3.3) compared to obese asthmatic children (1.45±1.4; p<0.01; Table 1), and this ratio was significantly higher in girls compared to boys in all groups (p<0.01; Table 2).

Comparison of serum leptin and adiponectin levels of girls according to study groups.
Comparison of groups 1 and 3: *p<0.05; **p<0.01.
Comparison of groups 2 and 4: ***p<0.05.
Significantly significant values are shown in bold.
FEV1 and FEF25–75 values in obese and lean asthmatic subjects were statistically lower than those in obese non-asthmatic subjects (Table 1). A negative correlation was demonstrated concerning FEV1/FVC and BMI in both obese (p<0.01, Spearman's ρ=–0.347) and lean asthmatic children (p<0.01, Spearman's ρ=−0.380). The FEV1/FVC ratio was positively correlated (p<0.01, Spearman's ρ=0.322) with adiponectin levels (Fig. 3), and FEF25–75 levels were inversely correlated with serum leptin levels in obese asthmatics (p<0.05, Spearman's ρ=−0.234; Figure 4). The FEV1/FVC ratio was negatively correlated with th eleptin/adiponectin ratio in lean and obese asthmatic patients (p<0.01, Spearman's ρ=−0.328; p<0.05, Spearman's ρ=−0.294, respectively).
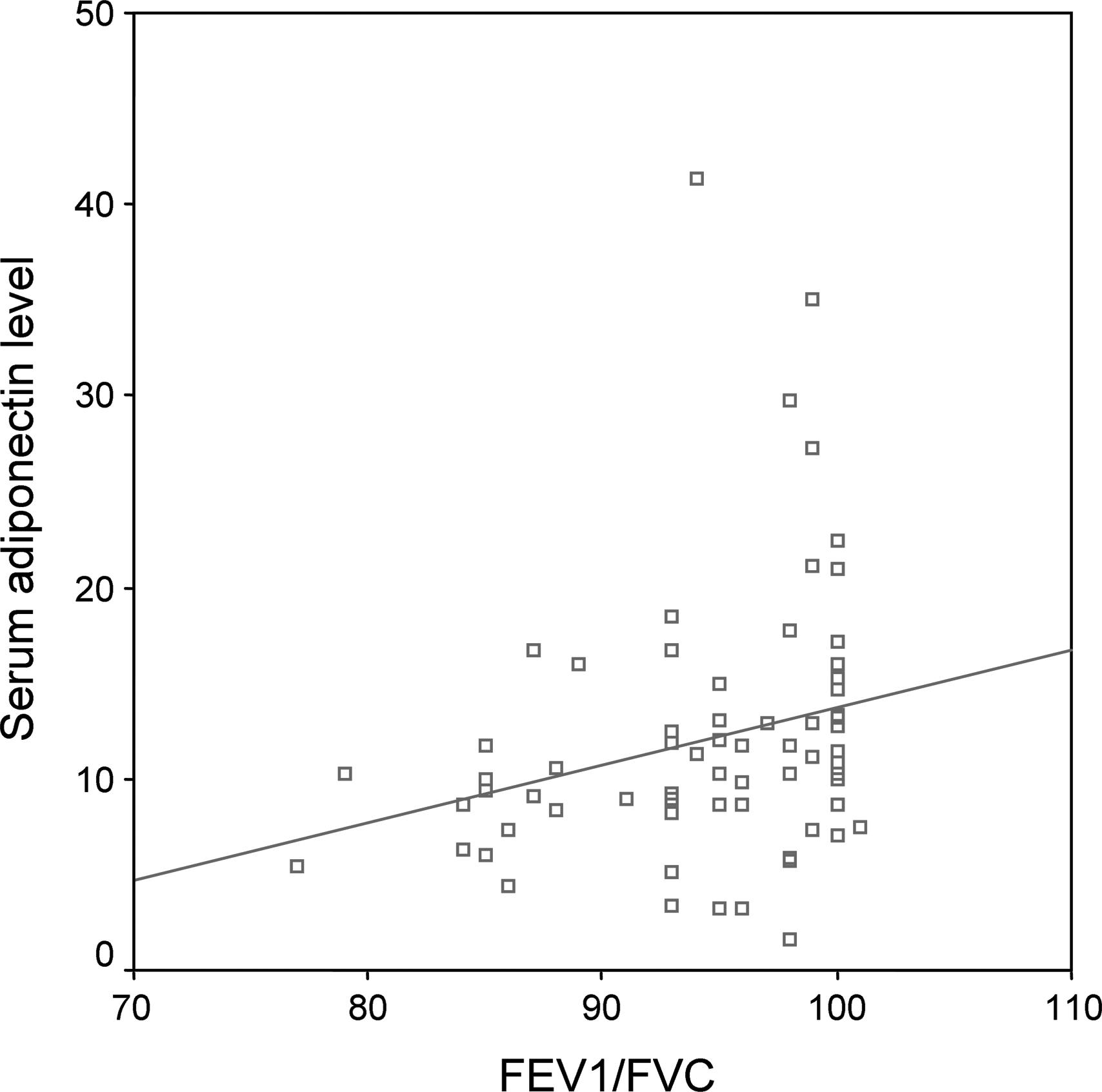
Relationship between serum adiponectin level and the forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) ratio in obese asthmatics.
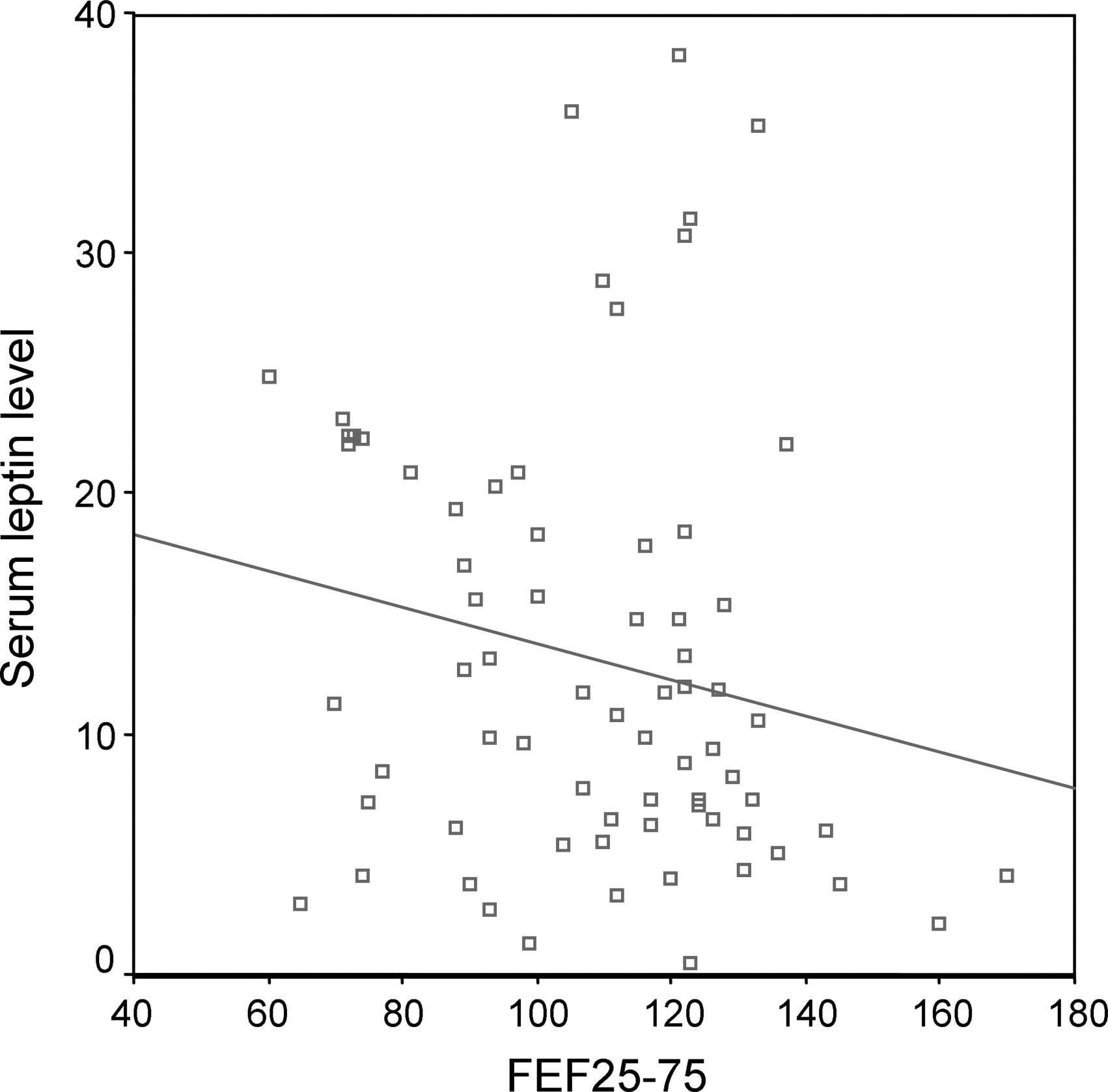
Relationship between serum leptin level and forced expiratory flow (FEF25–75) in obese asthmatics.
Discussion
In recent studies, the relationship between asthma and obesity has been demonstrated.3,4 Furthermore, obesity has been identified as a risk factor for asthma. Nevertheless, the underlying mechanisms have not yet been completely established, and data concerning the role of adipokines in asthmatic children are inconsistent.6,15
In the present study, serum adiponectin levels of lean asthmatic children were found to be higher than in the other groups, including the control group, with similar BMI percentiles. Meanwhile, obese asthmatics had higher adiponectin levels compared to those in non-asthmatic obese children. These findings are consistent with some studies published recently.16,17 However, conflicting results, indicating decreased18–21 or normal22–25 levels of adiponectin in asthmatics, have also been reported. Exogenous administration of adiponectin resulted in suppression of allergen-induced airway hyperreactivity and airway inflammation. 26 In the present study, it was found that lean as well as obese asthmatics had higher adiponectin levels compared to those in non-asthmatic peers. This finding suggests that adiponectin is part of the mechanism to counteract inflammation in airways and has a protective role in asthmatic children. A sex difference was prominent for adipokine levels only in lean children. Serum adiponectin levels of lean asthmatic girls were higher than in lean healthy girls, despite there being no difference among boys. This suggests that anti-inflammatory mechanisms regarding adiponectin work better in girls compared to boys. This can be explained by differences in the hormonal status of pre/peripubertal periods in boys and girls, and may also illuminate why childhood asthma is more prevalent in boys. 14 Recent studies have concluded that obese asthmatics had lower adiponectin levels compared to those in lean controls.17,27 However, in the present study, despite a prominent difference in BMI and leptin levels, no difference concerning serum adiponectin levels was determined between obese asthmatics and lean healthy subjects. This finding may indicate that having asthma in obese subjects might cause waxing in the anti-inflammatory protein levels, which supports the idea that increased adiponectin has a role in anti-inflammatory mechanisms in asthmatics.
Leptin is a pro-inflammatory protein that increases when fat tissue increases. This increase in fat tissue may contribute to the chronic inflammation in asthmatic airways. Similar to other studies, in the present study, serum leptin levels of obese subjects were higher than in lean counterparts. As expected, BMI showed a positive correlation with leptin levels due to the contribution of increased fat tissue.16,17,28,29 Although BMI is a determining factor for leptin, some studies have found that leptin levels were not elevated in obese asthmatics compared to lean asthmatics or controls.27,30 Indeed, the literature revealed different results for leptin levels in asthmatics, as for adiponectin levels, showing normal22,23,30–32 or increased levels.17,25,28,33–37 Although some studies suggest that leptin may play a role in asthma independent of obesity, leptin levels of lean asthmatics were not higher than healthy controls in the present study.27,33–35 The findings of this study suggest that having asthma has no effect on leptin levels in normal-weight children. On the other hand, since all patients were undergoing steroid treatment, it should be pointed out that inhaled steroid treatment may cause this protective effect. Supporting this conclusion, Gurkan et al. 35 found that leptin levels decreased after using inhaled corticosteroid treatment in asthmatic children. Decreased leptin levels may also have occurred due to successful asthma management.
The relationship between asthma and leptin is inconsistent when regarding sex. Recent studies have suggested that the influence of leptin on increasing risk of asthma varied by sex.33,35,38,39 In the present study, it was found that independent of having asthma, leptin levels of girls were higher than in boys in all groups except obese asthmatics. However, a similar sex difference concerning adiponectin levels was not evident. This finding suggests that increased leptin levels in girls are related to sex, regardless of asthma. Some other studies have also revealed that higher serum leptin levels are strongly associated with female sex in asthmatic children17,30,38,39 and adults. 36 In contrast, another study found higher serum leptin levels in asthmatic prepubertal boys, particularly in atopics. 33 This variety may have occurred due to differences in patient selection regarding age, sex, severity of asthma, hormonal status, percentages of body fat, and being in different life stages.
Attention should be drawn to why no sex and leptin level difference existed in obese asthmatics in the present study. First, in obese asthmatic girls, inhaled steroids might help to reduce inflammation or have more impact on inflammation and leptin levels. Second, asthmatic boys might have higher leptin levels so that no difference would be evident. Another finding is that with increasing age, serum leptin levels increase, and serum adiponectin levels decrease significantly in only obese asthmatics. Therefore, it is suggested that the effect of leptin on asthma may increase, whereas the effect of adiponectin may decrease with age, finally contributing to increased risk of asthma by age. Since leptin has pro-inflammatory and adiponectin has anti-inflammatory roles, leptin/adiponectin imbalance seems to be important, and the leptin/adiponectin ratio should be evaluated in future studies. Supporting this opinion, a recent study found a relationship between the leptin/adiponectin ratio and asthma at ages 24–39. 22 In the present study, the leptin/adiponectin ratio was higher in females regardless of having asthma or obesity probably due to having higher amounts of body fat percentages compared to boys with similar BMI. Nevertheless, it is suggested that larger and multicentric studies with homogenous patient groups can further elucidate relevance of leptin as well as adiponectin levels in asthmatic subjects.
An increase in BMI is accompanied by a higher FEV1 and FVC but lower FEV1/FVC ratio in both asthmatic and non-asthmatic subjects.3,40–42 Similarly, this study concluded with a negative correlation between BMI and FEV1/FVC ratio in asthmatics. Serum leptin was found to be inversely correlated with FEV1/FVC ratio in the mild/moderate asthma group. 37 Consistent with these studies, it was demonstrated that FEV1/FVC ratio in asthmatics was inversely correlated with the leptin/adiponectin ratio. This finding suggests that obstruction in the airways may be influenced by increased leptin and/or decreased adiponectin. In this study, leptin showed negative correlations with FEF25–75 in obese asthmatic children, as in a recent study showing the same correlation. 23 FEF25–75 has been accepted as an indicator of small airway function and influenced by airway smooth muscle. Since leptin is an inflammatory adipokine that attenuates airway inflammation in asthma, small airways would consequently be influenced in obese asthmatics. Inhaled steroids that have been used by lean asthmatic subjects may help to overcome the inflammation and obstruction in small airways. However, obese asthmatics may not be able to overcome excess inflammation due to increased leptin levels. High serum adiponectin concentrations were associated with higher FEV1/FVC 41 and FEF25–75 values. 23 In this study, a positive correlation was found between adiponectin and FEV1/FVC in obese asthmatics, which also supports the protective role of adiponectin in asthmatic airways.
Eosinophil percentages were significantly higher in asthmatics compared to non-asthmatic children. Besides, obesity is associated with higher eosinophil percentages. In this study, eosinophil percentages of all obese subjects, whether asthmatic or not, were also significantly higher than lean counterparts, which was consistent with the finding that obesity itself increased eosinophil activity. 43
In conclusion, findings of this study suggest that having higher levels of adiponectin may have protective disease-modifying effect(s) in asthmatic children. Anti-inflammatory mechanisms regarding adiponectin may work better in girls compared to boys in this age group. The findings may also contribute to why childhood asthma is more prevalent in boys, which could be explained by differences in hormonal status of pre/peripubertal periods. Additionally, having obesity along with asthma would probably cause a further increase in leptin levels that probably affects small airways.
Footnotes
Acknowledgments
This work was supported by Baskent University Research Fund (KA09/189).
Author Disclosure Statement
No competing financial interests exist.