
Abstract
Purpose:
Recent studies have reported that CD19+CD20+CD27+CD43+CD70-CD5− B cells produce IgG, IgA, and IgM antibodies to Streptococcus pneumoniae (Spn). In one adult patient with specific antibody deficiency (SAD), the percentage of CD5− CD19+CD20+CD27+CD43+CD70− B cells was decreased. The percentages of CD5−of CD19+CD27+CD43+CD70− B cells in children with SAD were examined in this study.
Methods:
Clinical and immunologic studies were obtained from a review of medical records. The percentages of CD5− of CD19+CD27+CD43+CD70− B cells were determined by flow cytometry.
Results:
Patients with SAD had significantly decreased percentages of CD5− of CD19+CD27+CD43+CD70− B cells. There was a significant correlation between decreased percentage of CD5−of CD19+CD27+CD43+CD70− B cells and decreased percentage of protective antibody titers to Spn.
Conclusion:
Decreased percentage of CD5− of CD19+CD27+CD43+CD70− B cells were identified in patients with SAD and correlated with decreased antibody responses to Spn.
Introduction
I
Recent studies in mice have reported that B-1 cells, identified by expression of CD19+CD20+CD27+CD43+CD70−, may play a role in anti-Spn antibody production. 1 In a murine model, Haas et al. 5 demonstrated that B-1a (CD5+CD11b+B220+) cells were primarily responsible for natural antibodies to Spn, whereas B-1b (CD5−CD11b+B220+) cells were responsible for acquired antibody responses to Spn. Thus, the B-1a cells are responsible for constitutive (predominantly IgM) antibodies to TI antigens.
Previously, Barrett et al. 6 reported in children that CD5− B cells secrete IgG, IgA, and IgM anti-Spn antibodies. Subsequent studies determined that B-1 cells could be further subdivided by whether CD5 was expressed: CD5+ (B-1a) and CD5− (B-1b cells). 1 The B-1b cells produce IgG, IgA, and IgM antibodies to Spn after antigen stimulation. In humans, Griffin et al. 7 reported the existence of B-1 cells characterized by the expression of CD19+CD20+CD27+CD43+CD70−. These cells were further characterized by expression CD5, and presumed to be human CD5+ (B-1a) and CD5− (B-1b) cells. Recently, Verbinnen et al. 8 reported that in healthy adults and children, CD5−CD19+CD20+CD27+CD43+CD70− B cells secrete IgG, IgA, and IgM to Spn and that these cells increased following Spn immunization. Furthermore, they noted these CD5− B cells were decreased in an adult patient with specific antibody deficiency (SAD), and did not increase following pneumococcal immunization.
Recently, Bossuyt's group raised concern that in humans CD20+CD27+CD43+CD70− cells may not be B-1 cells as previously thought, but rather may be pre-plasmablasts. 9 They reported that gene expression profiles of the CD20+CD27+CD43+CD69− cells cluster closer to CD20−CD27+CD43+ plasmablasts than to the CD20+CD27+CD43−CD69− memory B cells. Covens et al. 9 further reported that in humans in addition to spontaneously secreting IgG, IgA, and IgM similar to plasmablasts, the presumed B-1 cells also secreted predominantly IgG antitetanus antibodies following immunization, reminiscent of memory B-2 cells undergoing differentiation.
Whether CD19+CD20+CD27+CD43+CD70−CD5− cells in humans actually represent B-1b cells or pre-plasmablasts remains unclear. However, the previous finding of decreased CD5−CD19+CD20+CD27+CD43+CD70− B cells in an adult SAD patient prompted the examination of CD5−CD19+CD27+CD43+CD70− B cells in pediatric patients with SAD. If this B-cell subpopulation in fact consisted of pre-plasmablasts, it would not be entirely unexpected that CD5− B-cell percentages would be decreased in SAD patients. Additionally, if this B-cell subpopulation in fact consists of human B-1b cells, it would be interesting to observe whether these cells are decreased in SAD.
Methods
Patients
Patients who met the criteria below were identified and enrolled during 2012–2013 from the Pediatric Allergy and Immunology Clinic at Cardinal Glennon Children's Medical Center at Saint Louis University. Information on the presence of atopic dermatitis, asthma, allergic rhinitis (positive IgE to aeroallergens corresponding with symptoms), recurrent otitis media (four or more per year), recurrent sinusitis (two or more per year), pneumonia, skin infections (abscess, cellulitis), and sepsis (positive blood culture of S. pneumoniae) was recorded. The diagnosis of pneumonia and sinusitis may not have been documented radiographically. Surgical procedures of myringotomy and tympanostomy tubes (M&T), tonsillectomy and/or adenoidectomy (T&A), and functional endoscopic sinus surgery (FESS) were also recorded. We recorded treatment with prophylactic antibiotic and the use of intravenous (IVIG) or subcutaneous gammaglobulin (SCGG) therapy.
Subjects included 44 patients with SAD and 17 age-matched controls. (SAD was defined as normal serum IgG, IgA, and IgM levels, normal antibody responses to protein antigens but specific antibody deficiency to Spn immunization10,11 in children aged ≥2 years. Response to Spn was considered normal if the Spn antibody level was ≥1.3 μg/mL for ≥50% of the serotypes of children aged 2–5 years and ≥70% of the serotypes of children aged ≥6 years. 12 Control subjects were children referred for evaluation of recurrent infections who had normal IgG levels and normal antibody response to S. pneumoniae immunization.
The study was approved by the Saint Louis University Investigational Review Board. Study subjects received no compensation for their participation.
Immunoglobulin studies
Serum IgG, IgA, IgM, IgE, IgG subclasses, antidiphtheria antibody, antitetanus antibody, anti-Haemophilus influenzae type B (HiB) antibody, anti-Spn antibody levels, CD19+CD27+ memory B cells, and CD19+CD27+IgD− switch B-cell assays were performed as previously reported. 13 Patients had yearly analysis of B cells and memory and switch B cells performed. For analysis, the most recent study was chosen for analysis.
CD5− B cells
Measurement of CD5− B cells was performed as described by Verbinnen et al. 8 and Griffin et al. 7 Peripheral blood mononuclear cells (PBMCs) were isolated by Ficoll-Hypaque density centrifugation whereby 1×105 PMBCs in 0.5 mL of phosphate-buffered saline containing 2% fetal calf serum were stained with 20 μL of the following conjugated monoclonal antibodies obtained from Becton-Dickinson: CD19-FITC, CD27-Pacific Blue, CD43-APC, CD70-PE, and CD5-Per CP Cy-5. Flow cytometry was then performed using a five-color BD Biosciences LSR II flow cytometer, with data captured by BD FACS Diva and analyzed by FloJo software. First, gating was performed in forward scatter (FSC) and side scatter (SSC) to select lymphocytes. The CD19+ cells were then gated to select B cells; this was followed by gating on the CD19+CD27+CD43+ (B-1 cells). This population was further gated on the CD19+CD27+CD43+CD70− cells (presumed B-1 cells). This population was then analyzed for CD5+ (presumed B-1a) and CD5− (presumed B-1b) cells and were expressed as percentages of CD19+CD27+CD43+CD70− (B-1) cells. Verbinnen et al. 8 reported that CD5− cells were 20–40% in five adults and 10–42% in five children prior to Pneumovax® immunization.
Statistical analysis
The data were expressed as percentage of subjects, mean±standard deviation (SD) for demographic data and immunologic studies, and mean±standard error (SE) for CD5− B cells. A Student's t-test was performed. Spearman regression analysis was performed examining the relationship of CD5− B cells and Spn responses. For percentages of patients, Fisher's exact test for independence was used. p-Values ≤0.05 were considered significant using GraphPad InStat software package.
Results
Patients
There were 44 patients with SAD and 17 control subjects (Table 1). Demographic analysis revealed that SAD patients and control subjects were comparably matched for age, sex, and ethnicity (Table 1). Likewise, the prevalence of asthma, allergic rhinitis, and atopic dermatitis was similar in SAD patients and controls. Tonsillectomy and/or adenoidectomy (T&A) was significantly more frequent in SAD patients compared to controls (55% vs. 18%; p=0.011). However, M&T tube insertion and FESS was similar in both groups. Regarding infections, compared to controls SAD patients had increased frequencies of sinusitis (95% vs. 71%; p=0.015) and pneumonia (55% vs. 12%; p=0.003). However, there was no difference in the frequencies of otitis media, skin infections, or sepsis. Prophylactic antibiotics were used more frequently in SAD patients compared to controls (80% vs. 53%; p=ns), and IVIG was used significantly more in SAD patients (64% vs. 0%; p=0.009).
p-Value was determined by t-test. For percentages of patients, Fisher's exact test for independence was used. A p-value≤0.05 was considered significant. Data presented as mean±standard deviation (SD) or percentage (%).
AD, atopic dermatitis; AR, allergic rhinitis; FESS, functional endoscopic sinus surgery; IVIG/SCGG, intravenous or subcutaneous gammaglobulin; M&T, myringotomy and tubes; OM, otitis media; SAD, specific antibody deficiency; T&A, tonsillectomy and/or adenoidectomy.
Immunologic studies
Immunologic studies are presented in Table 2. Serum IgG, IgA, IgM, IgE, and IgG subclass levels were normal and comparable in SAD patients compared to control subjects. Similarly, antibody titers to diphtheria toxoid, tetanus toxoid, and Haemophilus influenzae type B were normal in SAD patients and control. However, SAD patients had significantly decreased protective antibody responses to S. pneumoniae serotypes compared to controls (40±19% vs. 82±9%; p<0.0001). CD19+ B cells, CD27+ memory B cells, and IgD−CD27+ switch B cells were comparable in SAD and control subjects (Table 2). The frequency of mannose binding lectin deficiency was nonsignificantly increased in 35% of control versus 25% of SAD patients, as was IgA deficiency (12% vs. 5%.)
Data presented as mean±SD or percentage (%). p-Value was determined by t-test. For percentages of patients, Fisher's exact test for independence was used. A p-value ≤0.05 was considered significant.
MBL, mannose binding lectin.
CD19+CD27+CD43+CD70−CD5− cells
In Figure 1, the correlation was examined between CD5− expressed as a percentage of CD19+CD27+CD43+CD70− B cells and the percentage of protective antibody titers to Spn serotypes following immunization to unconjugated S. pneumoniae in SAD and 17 control subjects. Analysis revealed a significant correlation between decreased percentages of CD5−of CD19+CD27+CD43+CD70− cells and decreased percentages of protective Spn responses (p=0.0018, r=0.3914). Interestingly, the data also demonstrated that three healthy control subjects had decreased CD5− CD19+CD27+CD43+CD70− B-cell percentages (<20%) but maintained protective S. pneumoniae antibody responses (≥70% of protective serotypes). Conversely, there were six patients with CD5−CD19+CD27+CD43+CD70− B cells >20% but with decreased S. pneumoniae antibody responses (<50% of protective serotypes). As seen in Figure 2, percentages of CD5−of CD19+CD27+CD43+CD70− B cells were significantly decreased in patients with SAD patients compared to control subjects (14±11% vs. 26±9%; p=0.0002). Decreased percentages of CD5− of CD19+CD27+CD43+CD70− B cells also demonstrated a direct correlation with the decreased percentages of CD19+CD27+ memory B cells (r=0.3612, p=0.004; data not shown) and CD19+IgD−CD27+ switch B cells (r=0.3294, p=0.0095; data not shown).
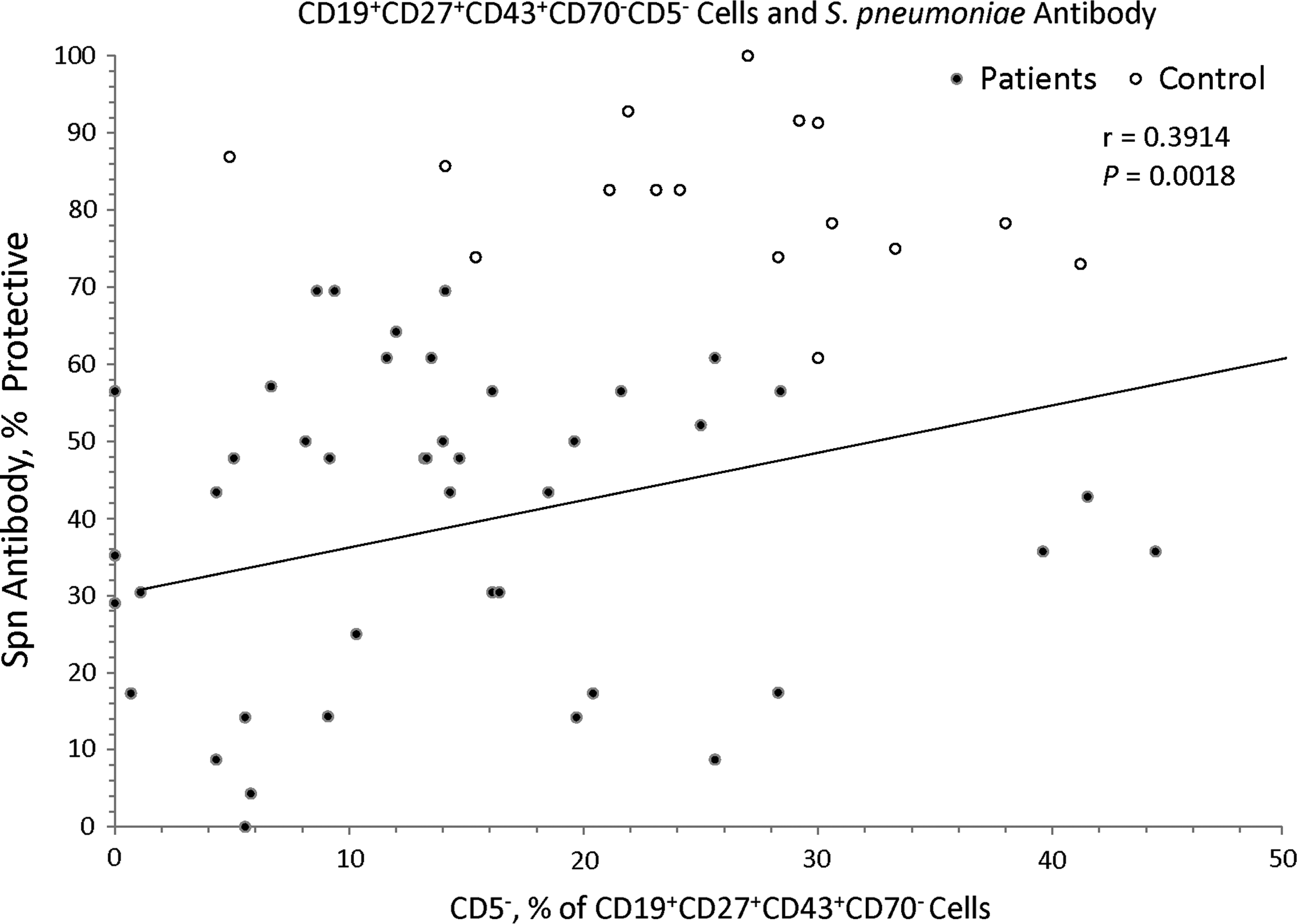
Correlation of CD5−CD19+CD27+CD43+CD70− B cells and antibody responses to Streptococcus pneumoniae expressed as percentage of serotype with protective antibody (≥1.3 μg/mL) following immunization with unconjugated S. pneumoniae. The data include specific antibody deficiency (SAD) and control pediatric subjects. Spearman regression analysis of patients and controls showed that there was a significant correlation of percentages of CD5−of CD19+CD27+CD43+CD70− cells and percentage of serotypes with protective S. pneumoniae antibody level (p<0.0018). The data also demonstrate that there were decreased CD5− percentages (<20%) but protective S. pneumoniae antibody responses (≥70% of protective serotypes) in three control subjects, and CD5− cells ≥20% with decreased S. pneumoniae antibody responses (<50% of protective serotypes) in six patients.
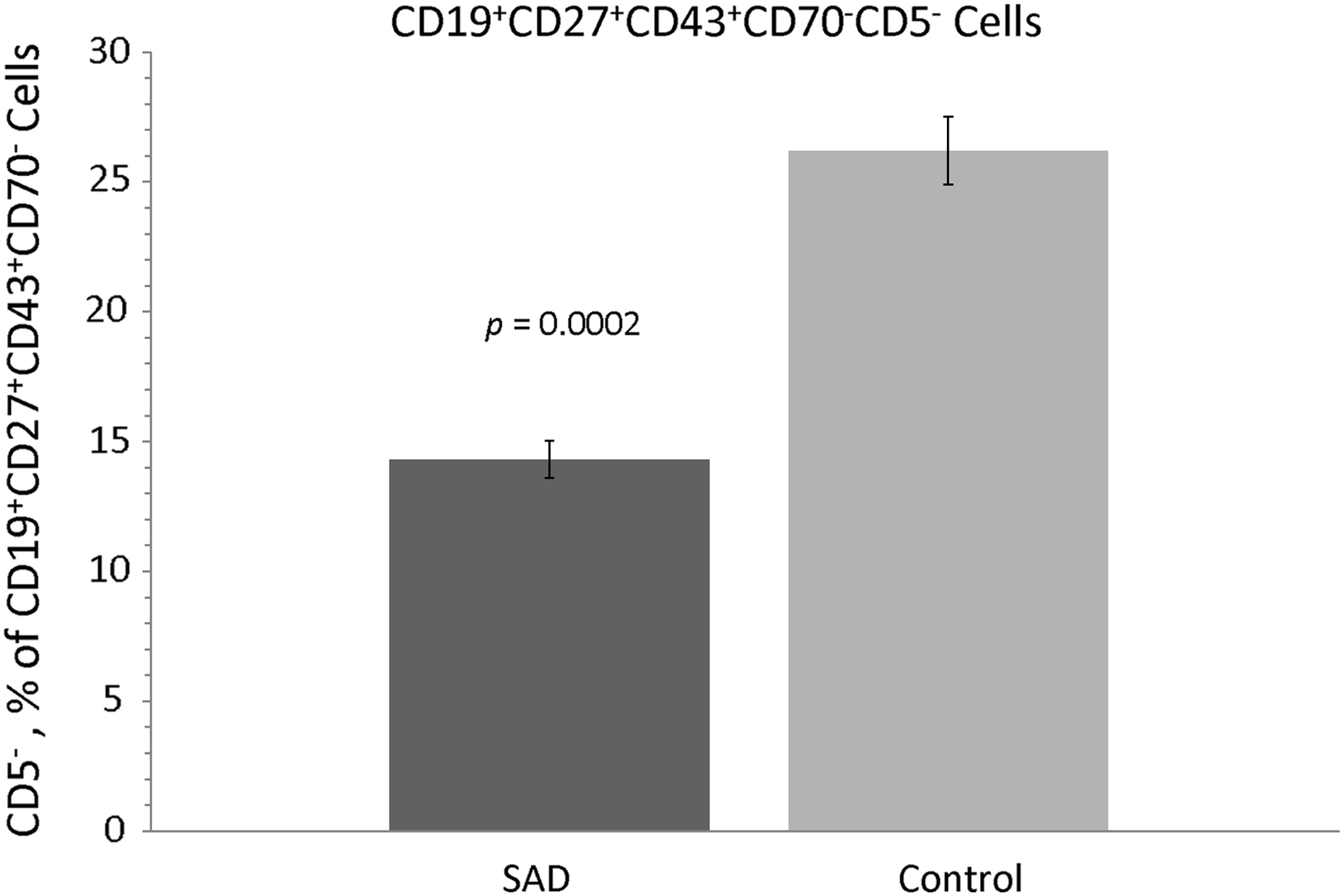
Percentages of CD5− of CD19+CD27+CD43+CD70− B cells in SAD and control subjects. The percentages of CD5− of CD19+CD27+CD43+CD70− B cells were significantly decreased compared to controls (p=0.0002). Data are expressed as mean±standard error.
Discussion
Barrett et al. 5 reported in children that CD5− B cells secreted IgG, IgA, and IgM anti-Spn antibodies following Spn immunization. Subsequently, in 1999, Antall et al. 14 reported that patients with SAD had increased percentages of CD5+ and decreased CD5− B cells compared to normal controls. However, CD5+ B cells were normal in patients with IgG subclass deficiency and common variable immunodeficiency (CVID). Recently, Verbinnen et al. 8 reported decreased percentages of CD5−of CD19+CD20+CD27+CD43+CD70− B cells in a patient with SAD. The mean percentage of CD5−of CD19+CD27+CD43+CD70− B cells in our control subjects was comparable to that reported in the pre-immunization patients of their study. To our knowledge, this is the first study examining CD5−CD19+CD27+CD43+CD70− B cells in children with SAD. Compared to controls, percentages of CD5−of CD19+CD27+CD43+CD70− B cells were significantly decreased in patients with SAD. There was a significant direct correlation between the percentages of CD5−of CD19+CD27+CD43+CD70− B cells and protective Spn IgG antibody responses. Interestingly, there were also some exceptions, as a few healthy individuals were found to have decreased percentages of CD5−of CD19+CD27+CD43+CD70− B cells with normal Spn responses, and six SAD patients had appropriate percentages of CD5−of CD19+CD27+CD43+CD70− B cells with decreased Spn responses. This finding was also observed in one control patient in the study by Verbinnen et al., 8 indicating that although decreased percentages of CD5− of CD19+CD27+CD43+CD70− B cells are associated with SAD, it is not the only important variable. In addition, decreased percentages of CD5−of CD19+CD27+CD43+CD70− B cells correlated with decreased memory and switch B cells.
Limitations to this study are acknowledged. Baseline immunologic evaluation was performed prior to the measurement of percentages of CD5−of CD19+CD27+CD43+CD70− B cells. Also, CD5−CD19+CD27+CD43+CD70− B cells were not examined before and after pneumococcal immunizations. So it is not known if these cells would have increased immediately post immunization. A prospective study would be needed to address these issues. The percentage of CD5− of CD19+CD27+CD43+CD70− B cells identified was performed gating on CD19+ B cells, whereas Verbinnen et al. 8 and Griffin et al.7,15 gated on CD20+ B cells. Thus, plasma cells and plasmablasts may have also been included in the analysis of these cells. Given the existing conflicting evidence as to whether CD19+CD20+CD27+CD43+CD70− cells represent human B-1 cells or plasmablasts, it is not possible to be entirely certain whether the evaluation of CD5−CD19+CD27+CD43+CD70− cells in this study measured human B-1b cells or pre-plasmablasts. Notwithstanding, it would be interesting that children with SAD had decreased plasmablasts. The finding of significantly decreased percentages of CD5−of CD19+CD27+CD43+CD70− B cells among children with SAD is a novel and compelling observation, whether these cells actually represent human B-1b cells or pre-plasmablasts. Additionally, further studies characterizing B-cell populations are necessary to advance the comprehension of and potentially advance the management of B-cell immunodeficiencies.
In conclusion, the percentages of CD5−of CD19+CD27+CD43+CD70− B cells were decreased in children with SAD. It was previously reported that in children with SAD, many patients may “outgrow’ this immunodeficiency. 11 Thus, future longitudinal studies may be interesting to examine whether CD5−CD19+CD27+CD43+CD70− B cells normalize as patients “outgrow” SAD and the potential future utility of these cells as clinical markers.
Footnotes
Acknowledgments
We appreciate the participation of the patients in this study. The study was supported by the Jeffrey Modell Foundation Diagnostic and Research Center for Primary Immunodeficiency at Cardinal Glennon Children's Medical Center at Saint Louis University.
Author Disclosure Statement
No competing financial interests exist.