
Abstract
Background:
Recent discovery of the Th17 pathway is providing new opportunities for understanding chronic immune-mediated diseases. The Th17 pathway has been historically associated with chronic inflammatory diseases such as psoriasis, multiple sclerosis, and rheumatoid arthritis. Among Th17 cytokines, pathogenic roles of IL-17A and IL-17F in asthma have been well described. Recently, the number of peripheral blood Th17 cells was found to correlate with disease severity in patients with atopic dermatitis (AD). This study aimed to investigate serum IL-17F levels in children with AD and to correlate this with severity of the disease.
Methods:
Enzyme-linked immunosorbent assay was used to measure IL-17F levels in the sera of 228 patients with AD and 62 control children. The SCORing Atopic Dermatitis (SCORAD) tool was used to determine the severity of disease.
Results:
The mean serum level of IL-17F in children with AD was significantly higher than that in the control group (p<0.05) Serum IL-17F levels were also higher in patients with severe AD than in those with mild AD (p<0.001), and IL-17F levels and SCORAD scores were positively correlated (p<0.05).
Conclusions:
Serum IL-17F level might be a useful marker in children with AD.
Introduction
A
Th17 cells produce cytokine of the Th17 cytokine family, consisting of six members named IL-17A to IL-17F. In humans, IL-17A and IL-17F levels have been shown to be involved in chronic inflammatory diseases such as psoriasis, multiple sclerosis, and rheumatoid arthritis. Recently, IL-17F has been reported to activate eosinophils to release profibrotic cytokines involved in tissue inflammation and repair.7,8 Increased production of IL-17F has been reported in stimulated peripheral blood mononuclear cells and bronchoalveolar lavage fluid from asthmatics. 9 Furthermore, upregulated IL-17F gene expression has been reported at sites of allergen challenge, and an H161R variant in the IL-17F gene was associated with protection against asthma in a cohort from Japan. 10 Neutrophil inflammation in the lung, mediated by IL-17F, was found to be steroid resistant, and IL-17F-related immune pathology may explain some aspects of the heterogeneity in asthma. 11 To date, few studies on the role of IL-17F in the pathogenesis of AD have been performed. In this study, the association of IL-17F levels in the sera of children with AD severity was investigated.
Methods
Subjects
The study included 290 children (Mage=5.50±4.06 years; 182 boys) who visited the allergy clinic for AD or a general health work-up at the Severance Children's Hospital from January 2006 to June 2013. AD was defined according to the Criteria of Hanifin and Raijka. 12 The severity of AD was determined using the SCORing Atopic Dermatitis (SCORAD) index system. 13 Two pediatric allergists made the AD diagnosis and performed the SCORAD assessment. There was no difference in the scoring between the two pediatricians. In this study, 228 children with AD were subdivided according to severity of AD, with cases classified according to SCORAD as mild (<15), moderate (between 15 and 40) and severe (>40) AD. Of AD cases scored, 129 patients (56.6%) had severe AD, 49 (21.5%) had moderate AD, and 50 (21.9%) had mild AD. The control group comprised 62 children (32 boys) with no history of AD or other allergic disease. At initiation of the study, serum total IgE levels, peripheral blood white blood cells (WBC), eosinophil counts, and neutrophil counts were determined. Total IgE levels were measured using a fluorimmunoenzyme assay (the CAP system FEIA; Phamacia & Upjohn Diagnostic AB, Uppsala Sweden) according to the manufacturer's instructions. Specific IgE levels >0.35 kUA/L were considered positive. A hematology analyzer (NE-8000; Sysmax, Kobe, Japan) was used to count peripheral blood WBC, eosinophils, and neutrophils automatically. This study was approved by Severance Hospital's Institution Review Board, and informed consent was obtained from parents of the children included in this study.
Evaluation of serum interleukin 17F
Blood samples were taken from all participants and separated by centrifugation at 400 g for 10 min. Serum samples were stored at −70°C until testing. Serum levels of IL-17F were measured using commercially available enzyme-linked immunosorbent assay kits (catalog #DY1335; R&D system, Minneapolis, MN), according to the manufacturer's instructions. The minimum detection level of IL-17F was 312 pg/mL.
Statistical analysis
Statistics analysis was conducted with SPSS Statistics for Windows v20.0 (IBM Corp., Armonk, NY). Data were compared between groups by Student's t-test and one-way analysis of variance. Due to the lack of normal distribution of peripheral blood WBC, eosinophil count, neutrophil count, and serum IL-17 level, its values in two and more subgroups were compared with the Mann–Whitney U-test and Kruskal–Wallis test. Linear regression was used to correlate serum IL-17F levels with serum total IgE, SCORAD, and total eosinophil count. Because the data for serum total IgE levels in AD patients were not normally distributed, a logarithmic transformation value was used for analysis. Age as a confounding factor was adjusted in the models. A p-value of <0.05 was considered statistically significant.
Results
Demographics, blood count, and IgE levels of subjects
Children with AD were younger than the control subjects (M±SD=7.93±3.9 years vs. 4.84±3.9 years; p<0.001). Children in the severe AD group were older than those in the moderate AD group (M±SD=5.36±4.1 years vs. 3.42±3.4 years; p=0.002). There were no significant differences in the sex ratio between the AD and control groups. Both blood eosinophil counts and WBC counts (median [interquartile range]) were significantly different between children with AD (465/μL [290–770/μL] and 9,080/μL [7,430–11,105/μL]) and controls (170/μL [100–275/μL] and 7,175/μL (6,180–8,732/μL)], with p<0.001. For serum total IgE (median [interquartile range]), children with AD had higher levels (143.0 [52.7–601.5 kU/L]) than those of the control group (31.0 [14.2–82.4 kU/L]) in this study, with p<0.001. There was no difference in neutrophil counts between the two groups. Demographic, blood count, and serum total IgE data are presented in Table 1.
Data are represented as mean±standard deviation (min–max) or median (interquartile range). p-Values were calculated in the adjusted analysis using multiple linear regression with an adjustment for age. A p-value of<0.05 was considered statistically significant.
Control group is different from AD group. †Differences between each of the three severity categories and the control group.
Comparison of IL-17F between AD and control groups
The serum IL-17F level (median [interquartile range]) of children with AD (5.96 ng/mL [2.10–15.80 ng/mL]) was significantly higher than that of the controls (3.13 ng/mL [0.95–8.75 ng/mL]), with p=0.005 (Fig. 1A). IL-17F was also significantly higher in the sera of patients with moderate (6.41 ng/mL [2.24–19.9 ng/mL]; p=0.001]) and severe AD (7.65 ng/mL [2.90–18.0 ng/mL]; p<0.001) than in those with mild AD (1.17 ng/mL [0.34–8.73 ng/mL]; Fig. 1B).
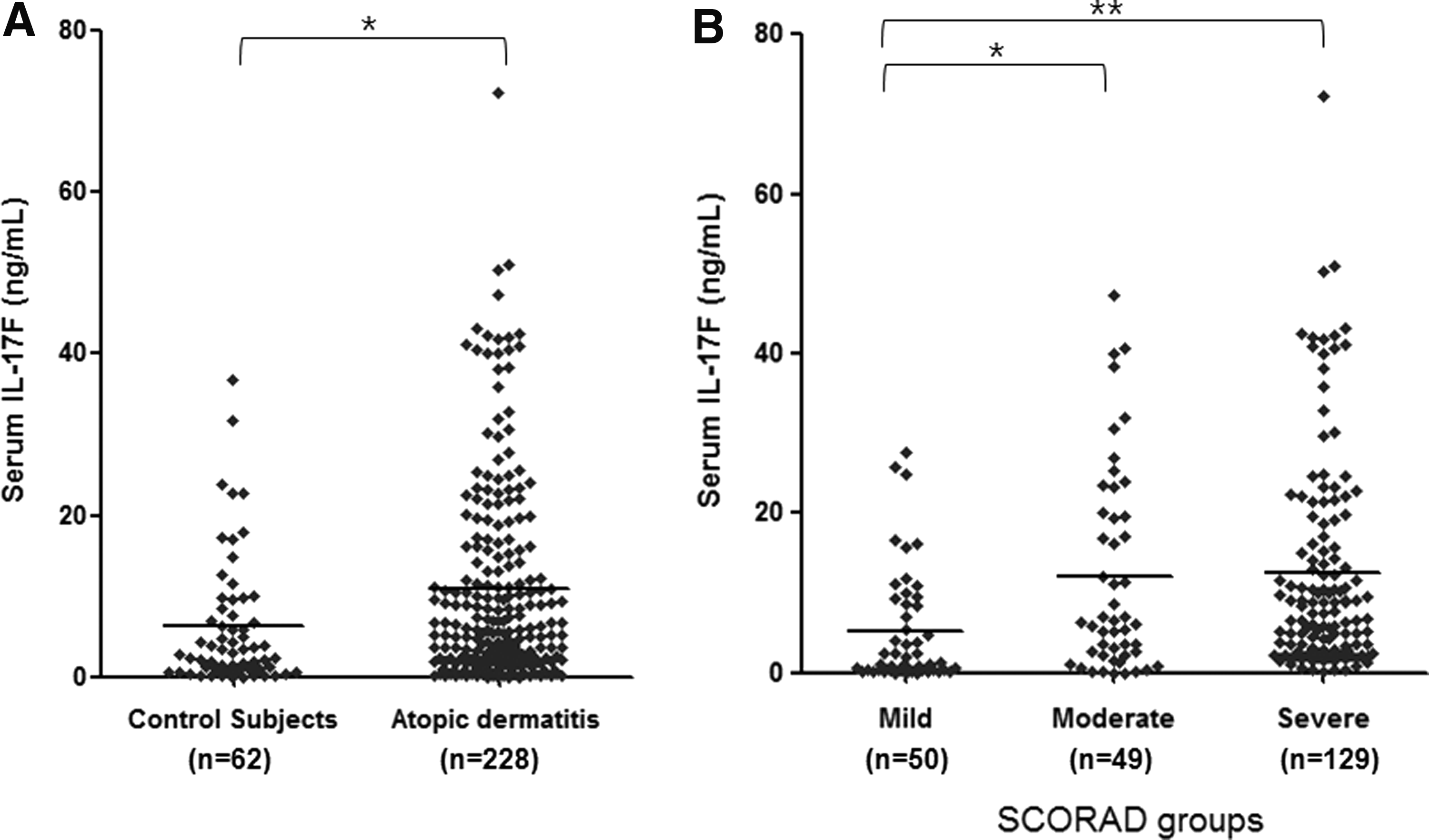
Interleukin (IL)-17F levels in the sera. (
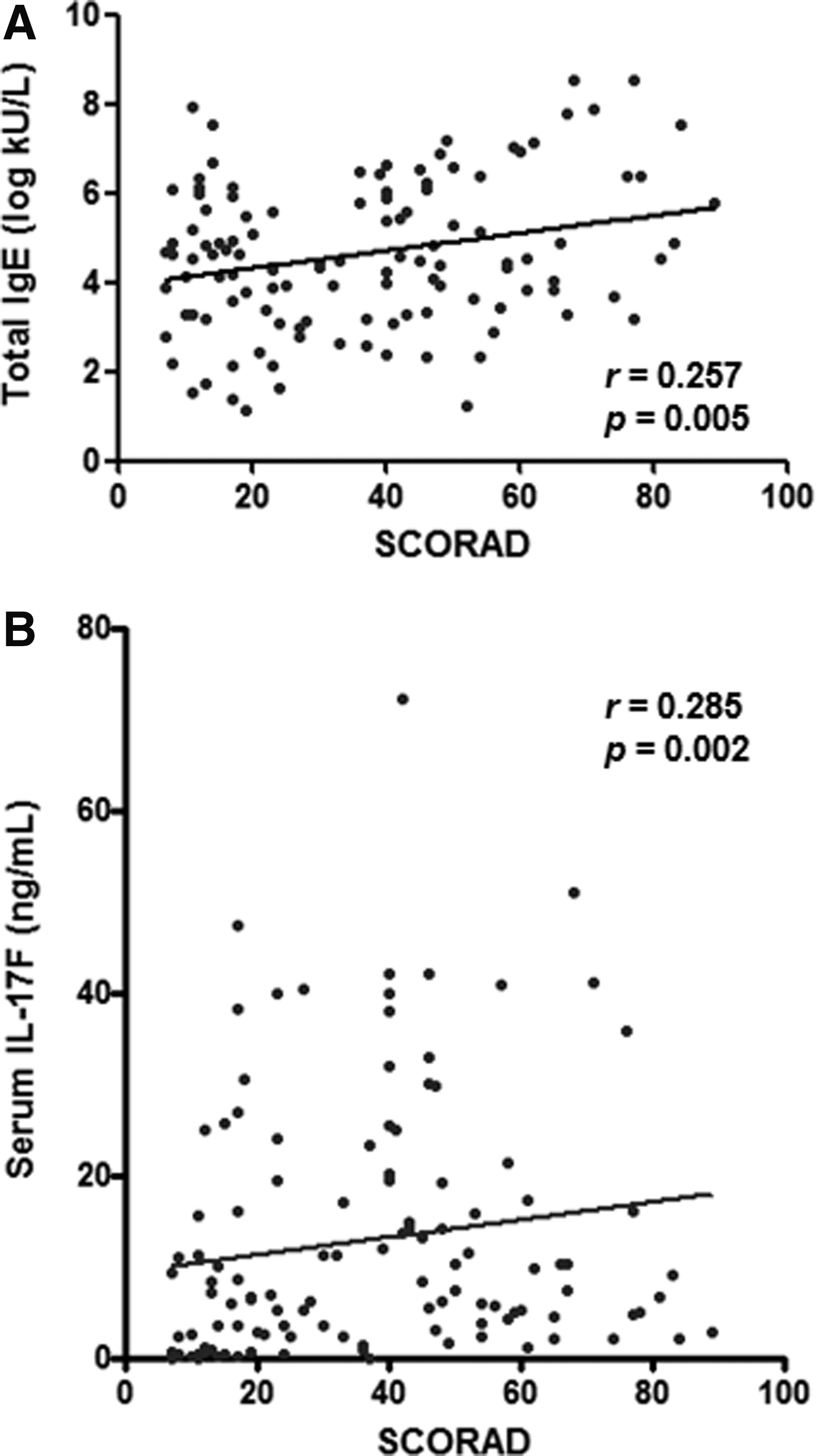
Correlation of serum IL-17F levels with total IgE levels and disease severity
In the AD group, total IgE levels were positively correlated with SCORAD (r=0.257, p=0.005; Fig. 2A). Similarly, serum IL-17F was positively correlated with SCORAD in the AD group (r=0.284, p=0.002; Fig. 2B). However, there was no correlation between serum IL-17F levels and serum total IgE levels, blood eosinophil counts, or neutrophil counts.
(
Discussion
IL-17A (also called IL-17) is the founding member and the best studied among the IL-17 family cytokines. 14 Besides being produced by Th17 cells, IL-17 is produced by a variety of cell types, including γδ T cells, NKT cells, NK cells, neutrophils, and eosinophils. 15 The IL-17F gene was discovered in 2001, and is located on chromosome 6p12. 16 IL-17A and IL-17F genes are localized in the same chromosome region, and IL-17F shares the strongest homology to IL-17A.17,18 However, IL-17F seems to function differently from IL-17A in immune response and disease. Interestingly, IL-17A and IL-17F appear to have opposite functions in chronic allergic airway diseases. While IL-17A deficiency reduced expression of Th2 cytokines, IL-17F deficiency enhanced Th2 cytokine expression and eosinophil function in mice. 19 In AD, few studies on the role of IL-17 family cytokines have been performed. An association between SCORAD score and IL-17 (IL-17A) levels (M=32.60 pg/mL, range 28.55–37.85 pg/mL) has been reported previously in a study of a Chinese population. 20 In the present study, serum IL-17F levels were significantly higher in children with AD than they were in healthy children. The results also showed that IL-17F is positively correlated with AD severity. As IL-17F has been reported to be involved in recruitment and activation of neutrophils, the study investigated whether the expression of this cytokines correlates with the blood neutrophil counts. 15 However, no correlation was found between serum IL-17F level and blood neutrophil counts. Hayashida et al. reported that the IL-17+ T cell subset in AD correlated with the levels of IgE and eosinophilia. 3 However, the present study found no correlation between serum IL-17F levels and serum total IgE or blood eosinophil counts.
AD is characterized by impairment in epidermal barrier function and abnormal immunologic cytokine expression in the skin and peripheral blood. Recent studies on the skin barrier role in the development of AD corroborate an “outside–inside” hypothesis. 21 The barrier dysfunction in AD involves two main components: decreased generation of filaggrin and tight junction defects. 21 Gutowska-Owsiak et al. reported a significant decrease in profilaggrin mRNA levels of keratinocytes after cultures were exposed to IL-17A. In addition to Th1/Th2 bias that influences expression of filaggrin, increased IL-17A may reduce the expression of filaggrin in keratinocytes. 22 Constitutive expression of an IL-17 receptor in keratinocytes has been previously reported. 23 Filaggrin-deficient mice were shown to possess increased IL-17 mRNA levels in skin lesions shortly after epicutaneous application of OVA. 24 In light of these findings, it appears that abnormal IL-17F expression in the skin may contribute to barrier dysfunction and lead to an increase in antigen penetration and priming of specific T cells. 25
However, the possibility cannot be excluded that elevation of IL-17F follows dysregulated immunity in AD. IL-17F is produced by cells of both the innate and adaptive responses, suggesting a bridging function between the two. In the skin, IL-17 is a master regulator of antimicrobial peptides (AMPs) and plays a central role in host defense of keratinocytes.26,27 Niebuhr et al. showed that α-toxins from Staphylococcus aureus induce IL-17 production in Th17 cells from atopic individuals. 28 Increased expression of IL-17 that exacerbates the inflammatory response may further contribute to the chronic nature of AD.
The present data indicate that IL-17F may play a role in the pathogenesis of AD. However, this study has some limitations. There were no functional or bioptical assessments of patients. For this reason, further studies should be conducted to examine the pathogenic role of IL-17F in AD.
Conclusion
In summary, this study investigated serum IL-17 levels in children with AD. Serum IL-17F levels are significantly increased in children with AD relative to a control, and IL-17F levels correlate with AD severity. The study suggests that serum IL-17F may play a role in AD pathogenesis.
Footnotes
Acknowledgments
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (grant number: HI11C1404).
Author Disclosure Statement
No competing financial interests exist.