
Abstract
A 9-year-old boy was referred to pediatric pulmonology with hemoptysis. There was history of a possible foreign body aspiration event that had occurred 4 months previously. Computed tomography scan of the chest demonstrated right lower lobe atelectasis. However, flexible fiber-optic bronchoscopy did not reveal any foreign body in the airway. Over the following month, there were two additional episodes of hemoptysis. In consultation with pediatric surgery, the child went to the operating room for video-assisted thoracoscopy. This revealed that there was an aspirated grass head that had migrated to the lung periphery.
Introduction
M
Here, a case is presented of foreign body aspiration of a grass head that was not suspected initially. However, with persistent hemoptysis and computed tomography (CT) scan abnormality, further evaluation was pursued, and a foreign body was eventually recovered from the lung periphery.
Case Report
A 9-year-old male was referred to the pediatric pulmonology clinic with hemoptysis. He started with a cough associated with frank hemoptysis at school 9 days prior to presentation. The following day, he had a coughing spell at home with another episode of frank hemoptysis. He was seen in the emergency room and had an episode of cough with frank hemoptysis there as well. A chest x-ray demonstrated a right lower lobe infiltrate, and a complete blood count had values that were normal. He was started on a course of azithromycin for 5 days. Hemoptysis persisted despite the antibiotic treatment.
Further history elicited that the boy had been playing outside 4 months previously and suddenly had an episode of difficulty breathing with a sensation that “something shot down his throat.” His older brother performed the Heimlich maneuver on him, which resulted in an episode of vomiting. He had no complaint of coughing, shortness of breath, fever, or wheezing in the interim until the occurrence of hemoptysis 9 days prior to presentation.
Given this history of recurrent hemoptysis, he underwent further investigation to explain the cause of his symptom. A chest CT scan was performed with intravenous contrast at an outside hospital that showed an area of probable atelectasis in the right lower lobe (Fig. 1). He was seen in the pediatric pulmonology clinic on the following day.

Computed tomography scan of the chest, demonstrating airspace opacity in the right lower lobe.
In clinic, physical examination showed a well-developed, well-nourished Caucasian male. Head and neck, cardiac, abdomen, and neurologic examinations were unremarkable. There were unlabored respirations with no retractions. The lungs were clear on auscultation.
A flexible fiber-optic bronchoscopy was subsequently performed 2 days later to explore for a foreign body in his airway. Normal upper airway anatomy was noted, and there was no evidence of tracheomalacia, bronchomalacia, or vascular compression. There were, however, scattered areas of blood seen in the right lower lobe bronchi. No foreign body was seen with a Pentax FB1570K (5.5 mm outer diameter) flexible fiber-optic bronchoscope. The scope was then changed to a Pentax EB1170K (3.8 mm outer diameter) for further evaluation of the airway with this smaller bronchoscope, enabling visualization up to the fourth generation bronchi of all subsegments of the right lower lobe, with no foreign body seen (Fig. 2). Bronchoalveolar lavage of the right lower lobe was performed and was noted to be slightly bloody. Bacterial, fungal, and mycobacterial cultures were negative.
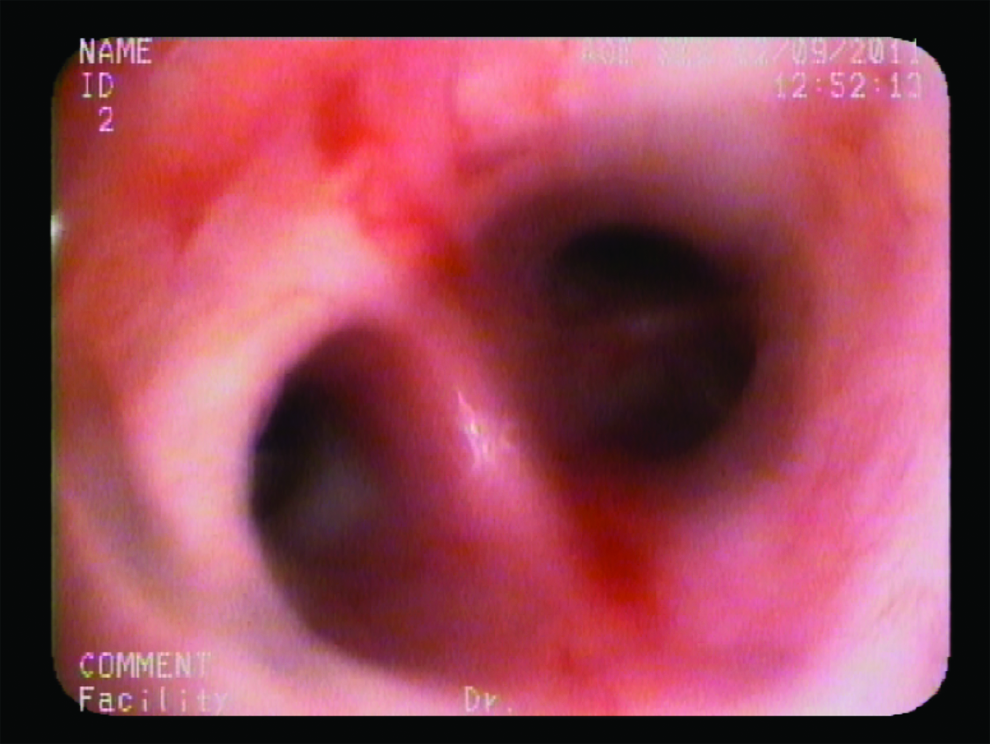
Flexible fiber-optic bronchoscopy image of right lower lobe bronchi, demonstrating lack of observable foreign body.
There was no explanation for the hemoptysis or the appearance of atelectasis on the chest CT scan. The family was told to contact pediatric pulmonology if there were continued symptoms.
In the next month, there were two more episodes of frank hemoptysis. In consultation with pediatric surgery, the decision was made for the boy to go to the operating room for thoracoscopic exploration.
Utilizing video-assisted thoracoscopic surgery (VATS), an incision was made at the mid-axillary line at the 5th intercostal space. The scope was passed into the thoracic cavity, and additional 5-mm ports were placed anterior to this, inferiorly and ventral to the initial port, and dorsally and inferiorly to the initial port. There were dense adhesions along the edge of the right lower lobe to the diaphragm and chest wall. After a difficult dissection of these adhesions, a piece of plant leaves (grass head) approximately 3 cm in size was encountered (Fig. 3). The foreign body was removed, and the right lower lobe underwent a wedge resection because of extensive adhesions and hemorrhagic lung tissue due to the presence of grass head within the lung parenchyma for several months. No migration channel was noted within the lung specimen by the pathologist or the surgeon. He had an unremarkable recovery following surgery and was discharged home.
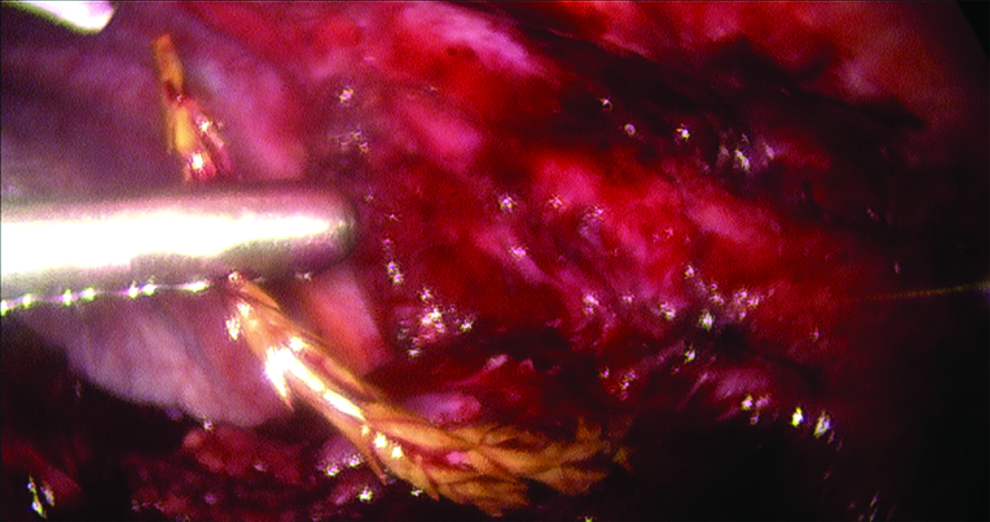
Video-assisted thoracoscopic view of hemostat grasping foreign body.
Discussion
A very high index of suspicion is essential in the management of any foreign body aspiration. When a large object causes near complete airway obstruction of the trachea, respiratory distress, cyanosis, loss of consciousness, and death can occur in quick succession unless the object is dislodged. When the degree of obstruction is incomplete or beyond the carina, the presentation may be less dramatic. In some instances, a history of initial dyspnea, choking, or cough with foreign body aspiration can be easily missed if not specifically inquired for or not suspected. An asymptomatic interval following the initial aspiration further complicates the clinical picture.
In this case, the initial history was suspicious of foreign body aspiration. The symptomless period followed by hemoptysis necessitated further work-up, and ultimately resulted in acquisition of a grass head from the lung periphery.
In many cases, recurrent hemoptysis is evaluated with angiography. However, in this case, a focal area of consolidation was noted on CT scan, and thus the surgeon was more suspicious of a localized area of disease, which led to the decision to proceed with VATS, as presented in this case.
A grass head aspiration and subsequent migration is a very rare occurrence. Previous case reports explain how this migration occurs based on the botanical characteristics of the grass head or inflorescence. The peculiar arrangement of firm and sharp spikelet, set at an acute angle to the rigid stem, encourages the one-way travel of the grass head until it reaches the chest wall.
An article published by Jackson 2 describes grass heads having the “power of spontaneous self-propulsion.” The two distinct clinical types of cases described were (1) the “lodging” type in which inflorescences remain in the respiratory passages, and (2) the “extrusive type” in which the inflorescences migrate to the periphery of the lung, penetrate the lung parenchyma, pleural layers, and intercostal muscles, and finally reach the chest wall, as seen with the present patient.
Foreign body aspirations may present as recurrent pneumonia, atelectasis, and/or persistent abnormal chest x-ray finding. However, presentation of grass inflorescence aspiration is more unusual, since there is no specific chest x-ray finding, and, as in this case, flexible bronchoscopy failed to demonstrate a foreign body in the airway. The presentations have also varied, with some patients presenting with hemoptysis and some with atelectasis.
A case report published by Hilman 3 described three patients requiring thoracotomy before recovery of the grass head, and one patient coughing out the grass inflorescence en route to the hospital. Another case report published by Karagöz 4 described a grass inflorescence that presented as a suspected soft tissue tumor. The child had a history of grass inflorescence aspiration 2 weeks prior to admission. On exam, there were diminished breath sounds from the right lower lobe. Chest CT scan confirmed a soft-tissue swelling of the right posterior chest wall with a hypodense area within the soft-tissue mass suggesting a foreign body, and also focal consolidation of the right lower lobe adjacent to the soft-tissue swelling. A sonography confirmed a hyperechoic foreign body under the skin. After 5 days of treatment with antibiotics, the abscess under the skin was drained, and the grass inflorescence was extracted.
A case report by Dilege 5 reported an adult male patient who was admitted with fever, dyspnea, and chest pain. A left pleural effusion and destroyed left lower lobe was noted in his chest CT scan. After chest tube drainage, massive hemoptysis developed that required an emergent thoracotomy. A bronchopleural fistula, destroyed left lower lobe, and the head of an oat were detected in the pleural space. Another case report by Newson 6 details a case of a 7-month-old boy who developed tension pneumothorax following aspiration of four grass heads. The baby had to undergo thoracotomy because the rigid bronchoscope was not able to extract the foreign body.
Maayan 7 reported five cases of oat head aspiration in children that resulted in serious complications due to the unidirectional migration of the oat head to the periphery of the lung. The complications reported included pneumothorax, pneumomediastinum, recurrent hemoptysis, chronic lung disease, bronchiectasis, lobectomy, bronchopleural and bronchocutaneous fistulae, pleural effusion, empyema cavity, and osteomyelitis of the rib. Lastly, Yellin 8 described a case of foreign body aspiration in an adolescent male who aspirated a wild oat head that migrated to the right pleural cavity and caused a severe persistent empyema. It resolved only after a thoracotomy and removal of oat head.
In summary, a strong suspicion and a thorough history is key in the management of any foreign body aspiration. A physician is encouraged to explore and identify the etiology of patient symptoms such as hemoptysis, wheezing, persisting cough, or signs such as persisting atelectasis, pneumonia, localized bronchiectasis, or persisting chest image finding, which was emphasized in this case. A high index of suspicion resulted in the CT scan, bronchoscopy, and subsequent thoracotomy leading to the ultimate discovery of the grass head in the lung periphery.
Lastly, when there is suspicion of foreign body aspiration that occurred outdoors, consideration should be given to the aspiration of plant species, more specifically grass head, with the possibility of migration of the foreign body into the lung parenchyma if it is not initially visualized in the airway on bronchoscopy. This should alter the approach and further management of foreign body aspiration.
Footnotes
Acknowledgment
We thank the boy and his family for permission to submit this case report.
Author Disclosure Statement
No competing financial interests exist.