
Abstract
Background:
Hidalgo County, located in Health Service Region 11 in the Rio Grande Valley near the Texas–Mexico border, has a high asthma hospitalization rate, with an age-adjusted hospitalization rate of 13.4% (12.5–14.3%) per 10,000.
Methods:
A longitudinal nonrandomized design was used, and a holistic and home-based approach was developed and implemented in the County to educate a targeted population of families with children diagnosed with asthma.
Results:
There were statistically significant improvements in knowledge, asthma symptoms, asthma management, quality of life, general knowledge of asthma, and healthcare utilization effectiveness. A trend was demonstrated in the improvement of overnight hospital stays, which dropped from 6% at baseline to 1% at follow-up. A significant change was also observed in the percentage of families reporting that their child required a clinic or doctor visit in the previous 4 weeks due to problems with asthma, with the percentage of families reporting a clinic or a doctor visit dropping from 50% at baseline to 31% at follow-up. The percentage of families reporting asthma attack incidents decreased by 30% between the first and last visits, and those reporting symptoms of wheezing or whistling while breathing declined by 23%. Significant improvements were observed in the physical health of children, including their ability to participate in physical activities, as well as improvement in the families' emotional health.
Introduction
I
In 2010, the Hidalgo County population was 774,773, an increase of 36.1% from the 2000 U.S. Census. Almost 90.6% were Hispanic, 3 and approximately 34.8% of persons were below the poverty line compared with 17.6% in the rest of the State. 4 High rates of uninsured families (38.6%) and low educational attainments among residents of South Texas also contribute to a lack of healthcare access and utilization. 3
Also, approximately 400,000 Texans live in colonias, which are substandard housing communities in unincorporated, irregular rural settlements located along the United States–Mexico border. 5 Health risks are created in some homes in colonias due to their poor maintenance and location (near agricultural fields), which is further exacerbated by increased rates of chronic diseases such as asthma. The latter has been extensively documented in environmental health literature,6–8 and suggests that home characteristics should be considered when providing asthma education. A successful asthma management strategy involves behavioral and environmental adjustments,9,10 along with the usual therapeutic measures, and emphasizes asthma trigger control in the home environment as a valuable tool to include in a comprehensive educational program.11–13 This article reports on results obtained from an asthma education intervention focused on a holistic and home-based approach that was utilized with 89 residents of colonias, and includes quality of life results, healthcare utilization, behavioral changes made after the educational intervention, and satisfaction of participants regarding education received.
Methods and Materials
Participants and setting
This study was a longitudinal, non-randomized design, using a snowballing technique for recruitment, which included the delivery of five surveys to assess asthma knowledge, quality of life, asthma triggers and management, and satisfaction with the intervention. The program was implemented from September 2012 to August 2014, and participants comprised 89 children and their parents living in Hidalgo County. Eligibility criteria for participation in the study were families with children ranging in age from 1 to 17 years old who had been diagnosed with asthma by a medical provider. Two promotoras (community health workers) were trained to provide the asthma and healthy homes education and to administer the surveys to participating parents in their respective homes. The Institutional Review Boards of Texas A&M and the University of North Texas Health Science Centers reviewed and approved the study protocols. Informed consent was obtained from parent(s) with an asthmatic child.
Measurements
The curriculum provided was based on a holistic educational intervention offered to participants that focused on asthma (information on the signs and symptoms of asthma, management of the disease, identification of common triggers, the adequate use of asthma medications, actions to take in case of an asthma attack, and fundamental components of an asthma action plan).14,15 The curriculum also included educational components from the Seven Principles of Healthy Homes, developed by the National Healthy Homes Training Center and Network, which focuses on how to keep a home dry, clean, ventilated, pest-free, safe, contaminant-free, improving the indoor environment, and decreasing hazardous exposures within the home. 16
Promotoras recruited families with asthmatic children throughout the year in diverse neighborhoods in McAllen, Edinburg, Mission, Alton, and San Carlos, Texas. The criteria for participation in the program were to have one or more children with asthma, between 1 and 17 years old, willing to receive education, and agreeing to allow promotoras to visit them three times during the study.
In the first encounter (baseline), parents were provided with education on asthma and a Children's Health Survey for Asthma was administered. At that time, everyone who participated received an allergen-proof mattress and pillow encasing, and were instructed in their use by a respiratory therapist. The first household visit was done 3 months later by promotoras who taught parents about the healthy homes principles and did a walk-through of the home with them in order to identify asthma triggers. The purpose of the second visit (6 months later) was to assure that the parent was continuing with the asthma triggers prevention in the household. The third visit (9–12 months later) was to review and walk through the house again to identify changes that the family had made to decrease asthma triggers, and to administer follow-up surveys. In addition, promotoras provided parents information on the Medication Assistance Program (MAP) that offers free or low-cost medication to individuals who are uninsured and underinsured. The number of MAP participants in the target population was small, since many were unaware of the program's existence. 17 The study utilized five assessment tools, described in Table 1. which contains information pertaining to the time of their application. The tools were (1) the Healthy Homes Pre/Post-Test Survey, (2) the Children's Health Survey for Asthma (CHSA), (3) the Asthma Home Environment and Triggers Checklist, (4) the Behavioral Changes Survey, and (5) the Post-training Satisfaction Assessment.
Statistical analysis
Data were initially entered into Excel worksheets, and then imported and analyzed in IBM SPSS Version 21 Statistics software. The Healthy Homes Pre/Post-Test survey items were coded as 0 for incorrect and 1 for correct, then summed for a total score. t-Tests were used to determine whether changes between pre and post versions were significantly different.
The CHSA instruction manual guidance was used to calculate the five subscales. t-Tests were used to determine whether differences between first and last CHSA subscales were significantly different. CHSA items associated with asthma symptoms, healthcare utilization, and sleep disruption due to asthma were all compared using the non-parametric McNemar test to determine if changes between first and last assessments were significantly different. Due to the lack of a normal distribution of continuous data elements, CHSA items were recoded dichotomously and analyzed nonparametrically. CHSA items associated with asthma attacks, whistling symptoms, overnight hospitalizations, and emergency department (ED) and doctor visits associated with asthma were coded as 0 if absent and 1 if present one or more times during the prior 4 weeks. Similarly, items measuring the presence of parent and child sleep disruption due to asthma, measured on an ordinal scale, was recoded as 0 if absent and 1 if present a little, some, most, or all of the time.
Simple descriptive statistics was used to summarize the Asthma Home Environment and Trigger Checklist, the Behavioral Changes Survey, and the Post-Training Satisfaction Assessment.
Results
Among the 94 families who enrolled in the 2013–2014 study, 89 completed the program, giving a retention rate of 95%. Given the longitudinal nature of the program, this retention rate is very high and demonstrates the promotoras' skill in engaging families for a sustained period. Nearly all of the 89 families who completed the program were Hispanic (97.8%), and reported household incomes were <$30,000 per year. Ninety-one percent were single-family households, and 60% said they owned their homes. On average, children began showing signs of asthma early, and were diagnosed between 2 and 3 years of age. Children were grouped into four age-based categories: 1–4 years old (32%), 5–8 years old (26%), 9–12 years old (27%), and 13–16 years old (15%). Parents were not knowledgeable about the severity of their child's asthma, as it is a medical term utilized by physicians for clinical diagnosis, and it refers to different classifications of asthma severity (intermittent and persistent: mild, moderate, and severe).
At intake, 29% of participants reported using their asthma controller medication every day, and at last follow-up, this was unchanged.
Socioeconomic characteristics
Results from the socioeconomic characteristics section of the intervention survey show that 87.64% were married couples, with 75.2% living below the poverty line and public insurance as their primary source of health coverage (70.9%). Additionally, 27% of the respondents identified their usual form of prescription payment as either out of pocket or copayment that were paid in cash or by credit card. Table 2 details participant demographics, and Table 3 shows the educational level of each child's parents.
Healthy Homes Pre/Post-Test Survey
Table 4 shows participants' knowledge of asthma, which was tested before and after the training using the Healthy Homes Survey. Overall, 54% of participants were able to increase their test scores by at least one point. Mean pretest scores were relatively high (M = 12.44), and post-test scores were close to the instrument ceiling of 14 (M = 13.42). A statistically significant change was observed between the pre- and post-test scores on the Healthy Homes Pre/Post-Test Survey (t[84] = −5.283, p = 0.000).
Maximum = 14.
CHSA
The CHSA measures three quality of life domains associated with the children (physical health, emotional health, and activities) and two family-level domains (emotional health and activities). Analysis of the five CHSA subscale scores revealed that participants made improvements in all domains, and differences in three of the areas were statistically significant (see Fig. 1). The biggest gain was in the emotional health of the family, which increased by nearly 9%, with physical health increasing by 6%, and activities increasing by 5%. Children's activities and emotional health increased by 2%. There was a statistically significant difference between the average baseline and the last assessment scores on the child's physical health (t[80] = −4.466, p = 0.000), family's activities (t[85] = −4.251, p = 0.000), and family's emotional health (t[87] = −4.274, p = 0.000) subscales of the CHSA assessment tool.

Average Children's Health Survey for Asthma (CHSA) subscale scores at baseline and at the last home visit. *Solid lines indicate statistically significant changes between first and last assessment.
Data from the CHSA showed a steady decline in asthma severity and asthma symptoms, as indicated by decreases in the proportion of families who reported one or more asthma-related incidents in the 4 weeks prior to home visits during the first, second, and last assessments (see Fig. 2). The percentage of families reporting asthma attack incidents decreased 30% between the first and last visits, and those reporting symptoms of wheezing or whistling while breathing declined by nearly 23%. About 89% of participating families completing an exit survey reported a decrease in the frequency of asthma attacks. The difference in the proportions of the respondents who reported one or more incidents of asthma-related symptoms (wheezing, whistling sound when breathing out) or an incidence of an asthma attack in the 4 weeks prior to the home visit during the first and the last assessment were statistically significant (p < 0.000).
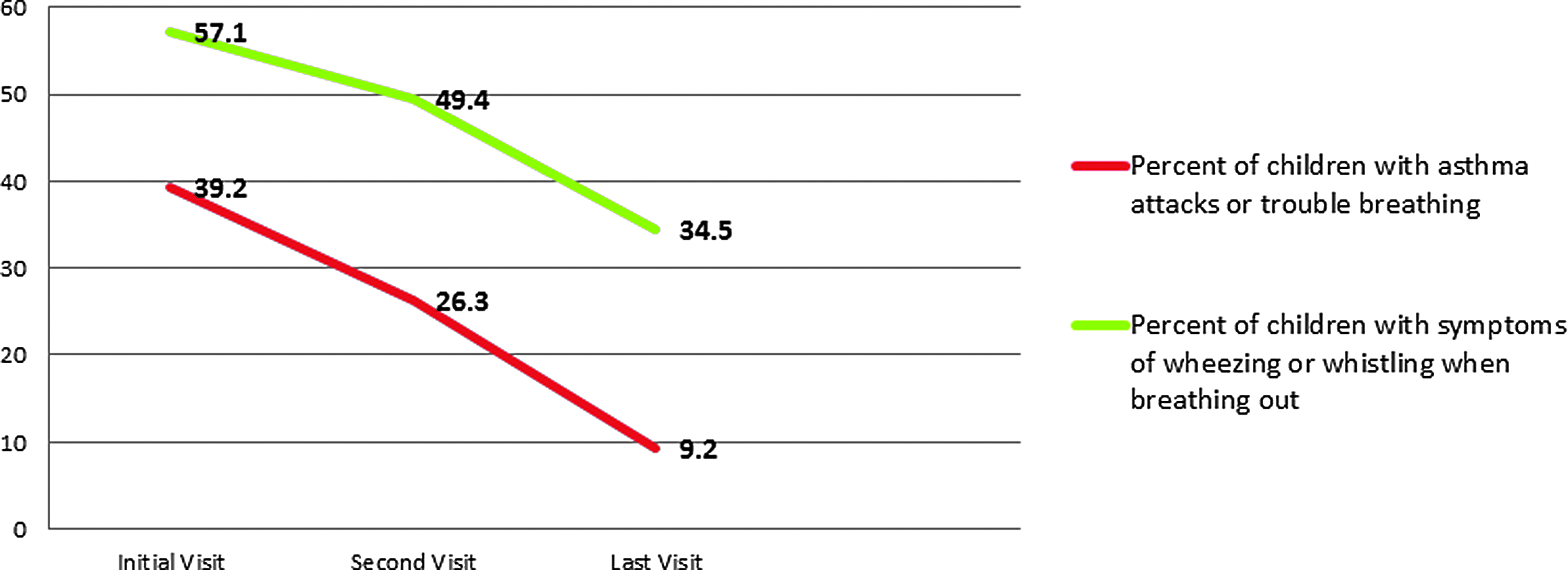
Percentage of respondents who reported one or more asthma-related incident in the 4 weeks prior to the first, second, and last home visits.
Healthcare utilization
Asthma symptoms that require overnight hospitalization or ED visits are proxies of poor asthma management. At baseline, approximately 6% of the families reported overnight or ED hospital visits in the previous 4 weeks. At the last follow-up assessment, ED utilization did not change, but overnight hospital stays dropped to 1%. Although the change in proportion between first and last visits for overnight hospital stays was positive, the difference was not statistically significant. Nonetheless, it is worth noting that among the five families who reported overnight stays at the baseline assessment, none reported hospitalizations at the last assessment. Given the cost of overnight hospitalizations, these results may hold substantive significance and warrant further investigation. Furthermore, among the five families with ED visits at baseline, none reported ED usage at the last assessment. Of the four families reporting ED visits in the last assessment, none reported ED visits at baseline.
The CHSA also asks parents to report the number of visits to clinics or doctors' offices due to asthma-related problems in the previous 4 weeks. Among the 80 families who answered these questions at the first and last assessments, a third (n = 27) reported clinic usage at baseline and no clinic usage at the last assessment (see Fig. 3). The percent of participants with one or more clinic visits dropped significantly from 51% at baseline to 31.3% at last follow-up (p < 0.05).
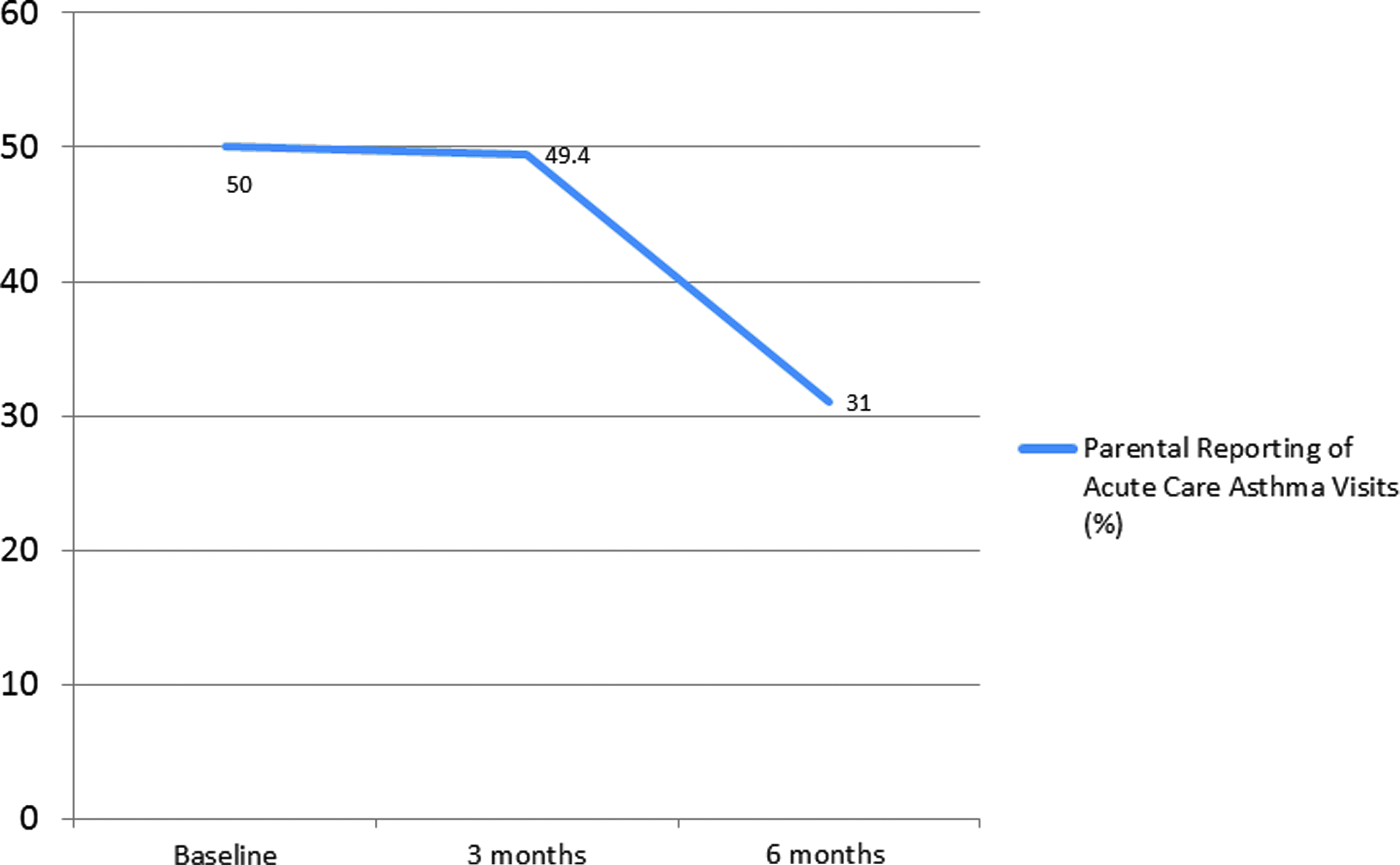
Parental reporting of acute care asthma visits.
Other quality of life improvements
Participating parents and their children demonstrated a reduction in the effects of asthma related to sleep. Half of the parents and nearly half of the children who reported sleep problems at baseline were no longer experiencing sleep disruption at the last assessment (see Fig. 4).
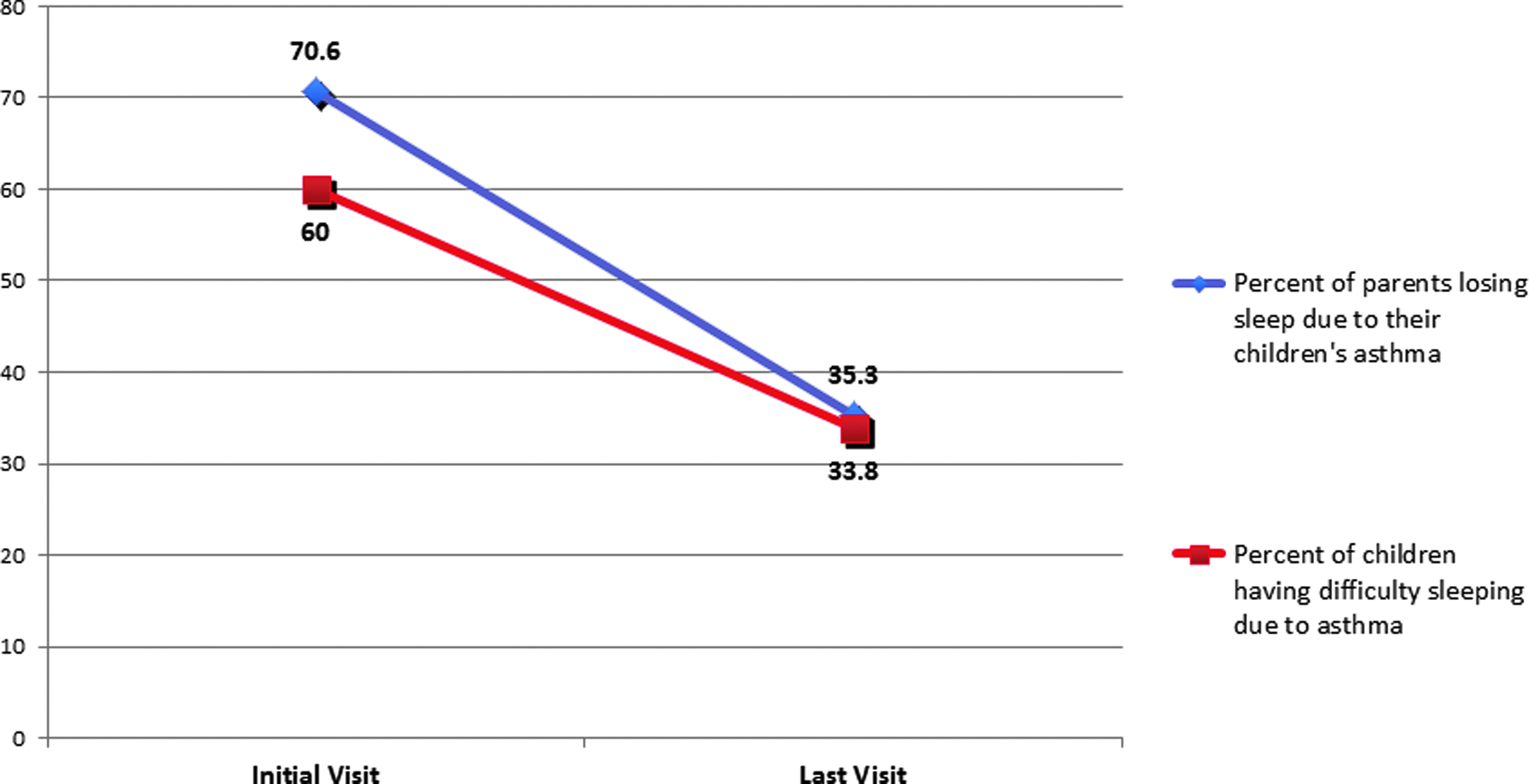
Sleep improvements for parents (n = 85) and children (n = 80).
When collapsed into categories of lost sleep or difficulty sleeping versus no lost sleep, or no difficulty sleeping, changes between the first and last assessments were statistically significant for both measures (p = 0.000).
Asthma home environment and triggers checklist
During the first visit, parents where asked about types of asthma triggers that are problematic for their children. The most prevalent triggers identified were cigarette smoke (12.5%), strong smells (44.3%), and pollen (73.6%).
Behavioral changes survey
All participants reported at least one behavioral change, and the vast majority (89%) indicated they had made a change in the previous 4 weeks. Among 32 healthy homes strategies ranging from roof repairs to avoiding pesticide use, participants reported using an average of 19 strategies. The most commonly cited were frequent home cleaning, not allowing smoking in the home, and opening windows for ventilation. The behavioral change involving not allowing smoking inside homes increased from 83.7% at baseline to 89.9% at 3 months post-training. Additionally, five families reported that they repaired the water leaks in their homes, and two other families reported that they were no longer using gas stoves for heating.
Post-Training Satisfaction Assessment
Participant feedback was collected using the Post-Training Satisfaction Assessment. These results showed that almost all participants were satisfied with: (1) the individual who provided the training (96.5%), (2) information provided during the training (98.9%), and (3) the program overall (97.6%). Nearly all participants (94%) agreed that the information presented increased their knowledge about asthma, and 39.8% reported they would have liked more educational visits.
Discussion
Asthma adversely affects the overall quality of life of children during their formative years and can negatively impact not only their physical and emotional health, but also their attendance in school and their ability to participate in sports and other activities. Families may also be affected through missed time from work, activity limitations, and emotional and economic strain. The present findings suggest that the majority of parents can improve their overall knowledge of asthma and healthy homes (asthma triggers and how to decrease them at home) with a short, basic training over a brief period, as other studies have reported.11,18,19 Out of the 89 participants reached through promotora visits, 59.7% increased their knowledge, which was an improvement from the results obtained in the pretest 3 months earlier. All participating households received three visits from promotoras who provided them with allergen-proof mattress and pillow encasings. Additional resources for decreasing triggers were included in the healthy homes principles included in the training curriculum such as tips on how to maintain a home properly and “recipes” for inexpensive, eco-friendly products that can be utilized for cleaning purposes. Parents reported that knowledge gained from the education provided them with the ability to help their children by reducing exposure to asthma triggers, which significantly decreased asthma attacks. Similar results have been reported in other studies that have focused on reducing asthma triggers by using healthy homes principles.11,20–22 It is important to note that those receiving the educational intervention in each household were mostly stay-at-home mothers. Among the results obtained in this study, researchers believe that for those families who are underinsured or not insured, the only way to access healthcare for their children is via the ED, and thus this may be why utilization of these types of services remained unchanged. The stable amount of asthma clinic visits may be attributed to the fact that these children had routine follow-up visits with their medical provider for the purpose of refilling medication and general monitoring of their asthma status. Parents were not knowledgeable about their child's asthma severity. Based on the results obtained with the use of their asthma medication, more education is needed for children and their parents regarding the importance of the daily use of their controller medication. A smoking cessation intervention was not implemented in this study. However, since it is a critical component for asthma management, it will be addressed in future studies.
Study limitations
The use of self-report instruments for the pre- and post-tests could have led to some biases. Further, the use of a nonvalidated true–false survey can create bias. The follow-up for the 89 heads of households was difficult at times because this was a hard-to-reach population. The healthcare utilization section of the study is limited by both self-report and the time periods referenced by the medical questions (e.g., 4-week intervals). The measurement of actual ED and clinic visits, including hospitalizations for the year before and after the intervention, would more accurately determine whether the utilization of these services changed. Since the CHSA references only the previous 4 weeks, interpretation of these data is limited. Hospital utilization is infrequent, and measuring only periodic 4-week intervals makes it difficult to detect changes over a longer period. The lack of a control group limits the comparison of results.
Conclusions
The results from this study demonstrate that improvements in the areas of healthcare utilization, asthma symptoms, quality of life impact on families, and participants' knowledge of asthma and use of management strategies is possible. Assessment of the asthma intervention and implementation shows that the intervention targeted at high-risk families using the promotora model is useful in engaging these families over time. Based on these results, participating families who live in environmentally substandard housing located in colonias may benefit from an integrated training approach, thereby decreasing the risk of asthma episodes.
Footnotes
Acknowledgments
This project was undertaken with funds obtained under Contract No. 2010-034647 from the Texas Asthma Control Program (TACP), which is funded by the Centers for Disease and Control, and located within the Chronic Disease Branch under the Texas Department of State Health Services, and the Environmental Protection Agency through grant #2012-23-461541. The authors wish to extend their gratitude to all participating parents. Special acknowledgment and thanks go to respiratory therapy students from South Texas College, as well as their instructors, for their help in educating children with asthma. Additional thanks to Yvette Ysaguirre and Zaida Rosa Rojas, Registered Respiratory Therapists from Rio Grande Regional Hospital, for their collaboration and the training they provided to study participants. The authors wish to acknowledge the data management and analysis assistance of Goutham Ghanta, BDS, MPH, and Darius Taylor, MPH.
Author Disclosure Statement
No competing financial interests exist.