
Abstract
The measurement of sweat chloride concentration (sweat test) remains the gold standard for the diagnosis of cystic fibrosis (CF). For infants with a positive newborn screening test for CF, the sweat test is the next step to confirm the diagnosis. However, there are several reports in the literature regarding conditions that are known to be associated with false positive or false negative sweat tests. This systematic review of the literature summarizes the evidence available regarding these conditions. Interpretation of sweat test results should be done in the context of patient's clinical presentation and associated comorbidities. Additional research is needed for conditions that may affect sweat chloride concentrations.
Introduction
C
The Gibson Cooke Method utilizes a piece of gauze soaked in pilocarpine solution that stimulates the sweat glands, followed by application of dry gauze for 30 min to collect a minimum of 75 mg of sweat. The Macroduct method utilizes agar gel discs with pilocarpine for stimulation, but it only requires a minimum of 15 μL of sweat that is collected into a microbore tubing. The measurement of sweat chloride concentration is done with a chloridometer that uses coulometric titration, as per the standards recommended by the Clinical and Laboratory Standards Institute (CLSI). 1 For infants under 6 months of age, the normal sweat chloride concentration is <30 mmol/L; 30–59 mmol/L is intermediate; and ≥60 mmol/L is considered abnormal. 2 For children over 6 months of age and adults, <40 mmol/L is the normal range of sweat chloride concentration; 40–59 mmol/L is intermediate; and ≥60 mmol/L is abnormal. 2
This test has become especially important as a confirmatory test now that CF is part of standard newborn screening across the United States. For all infants with a positive newborn screening test for CF, the sweat test is the next step to confirm the diagnosis and start CF-specific treatment. Given the significant impact of the diagnosis of CF on patients and their families, it is important to ensure that the sweat test is performed correctly and its results can guide appropriate decision making.
Sweat testing has been performed in clinical practice for the last 50 years. During that time, numerous instances have been reported in the literature where the test has been reported to be intermediate or positive when patients did not have the typical manifestations of CF (false positive), or rarely reported to be negative when they did have some clinical concern about possibly having CF (false negative). The list of these conditions that are associated with either false positive or false negative sweat tests has grown significantly over time, as shown in Table 1. However, it is important to note that most of the conditions that have been listed as the cause of false positive sweat test were reported much before the discovery of the CFTR gene in 1989 and lack confirmatory genetic testing to rule out atypical forms of CF.
CFTR, cystic fibrosis trans-membrane conductance regulator; KID, keratosis, icthyosis and deafness.
Another drawback in these reports is the use of various older nonstandardized methods of sweat collection and testing that were in vogue in the 1950s and 1960s, such as thermal sweating, urecholine iontophoresis, overnight sweat collection, skin electrical conductivity testing and so on. Now that the technique of pilocarpine iontophoresis has been standardized based on the defined rates of sweating and volume of sweat to be collected, there is much more uniformity in collecting sweat samples. The purpose of this review is to critically analyze the strength of the evidence behind each listed condition that causes a false positive or false negative sweat test so that providers can interpret test results correctly in any clinical situation. We have performed a systematic review of the literature to compile all the possible conditions that have been reported to cause a false positive or false negative sweat test result and have critically analyzed these articles.
Methods
To identify articles describing various causes of false positive and false negative sweat tests, we conducted a systematic review of the literature using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 3 Using predefined search terms (“Sweat Test,” “False Positive,” “False Negative,” “Sweat Chloride,” “Cystic Fibrosis”) in different combinations, we performed the same literature search on 5 databases: PubMed, Scopus, CINAHL (EBSCOHost), Web of Science, and Cochrane Library.
From the references identified during the initial search, 2 of the authors screened all the studies to remove duplicates, review articles, and so on and to select the ones that were most relevant to the subject of this systematic review. After identifying these selected references, full text versions were obtained from Shiffman Library at Wayne State University and all the individual references were also screened for any other additional studies or articles (cross-references) that were cited by these selected references. After finalizing the complete list of articles to be included in the review, each article was reviewed by one of the authors to extract the information about the various reported false positive and false negative causes of elevation of sweat chloride concentrations. This systematic review was registered with International Prospective Register of Systematic Reviews (maintained by University of York Center for Reviews and Dissemination, at www.crd.york.ac.uk/PROSPERO/) (Protocol No. CRD42015025529).
Further analysis of the likelihood of a reported condition being a true cause of false positive or false negative sweat test was categorized on the basis of the following:
<3 reported cases: Unlikely 3–9 reported cases: Probable, but needs validation 10 or more reported cases: Likely
However, in the presence of genetic testing for CFTR mutation that has ruled out the diagnosis of CF, a reported cause can be considered as “Likely” irrespective of the number of cases reported. All the references selected for this systemic review were then graded into either 1 of these 3 categories, based on the data extracted from the published reports.
Results
The results of the systematic review have been presented in Fig. 1. From the studies that were finally included in the systematic review, we have listed the various conditions identified as the cause of false positive or false negative sweat tests in Table 1. Further analysis of each of these conditions and their grading of the likelihood (based on the methodology described above) has been provided in Table 2. Review of the reported conditions revealed a lot of heterogeneity in the sweat testing procedure, with many of the older publications using urecholine iontophoresis or obtaining sweat samples from other body sites (such as the back) that are no longer recommended for the sweat testing procedure.
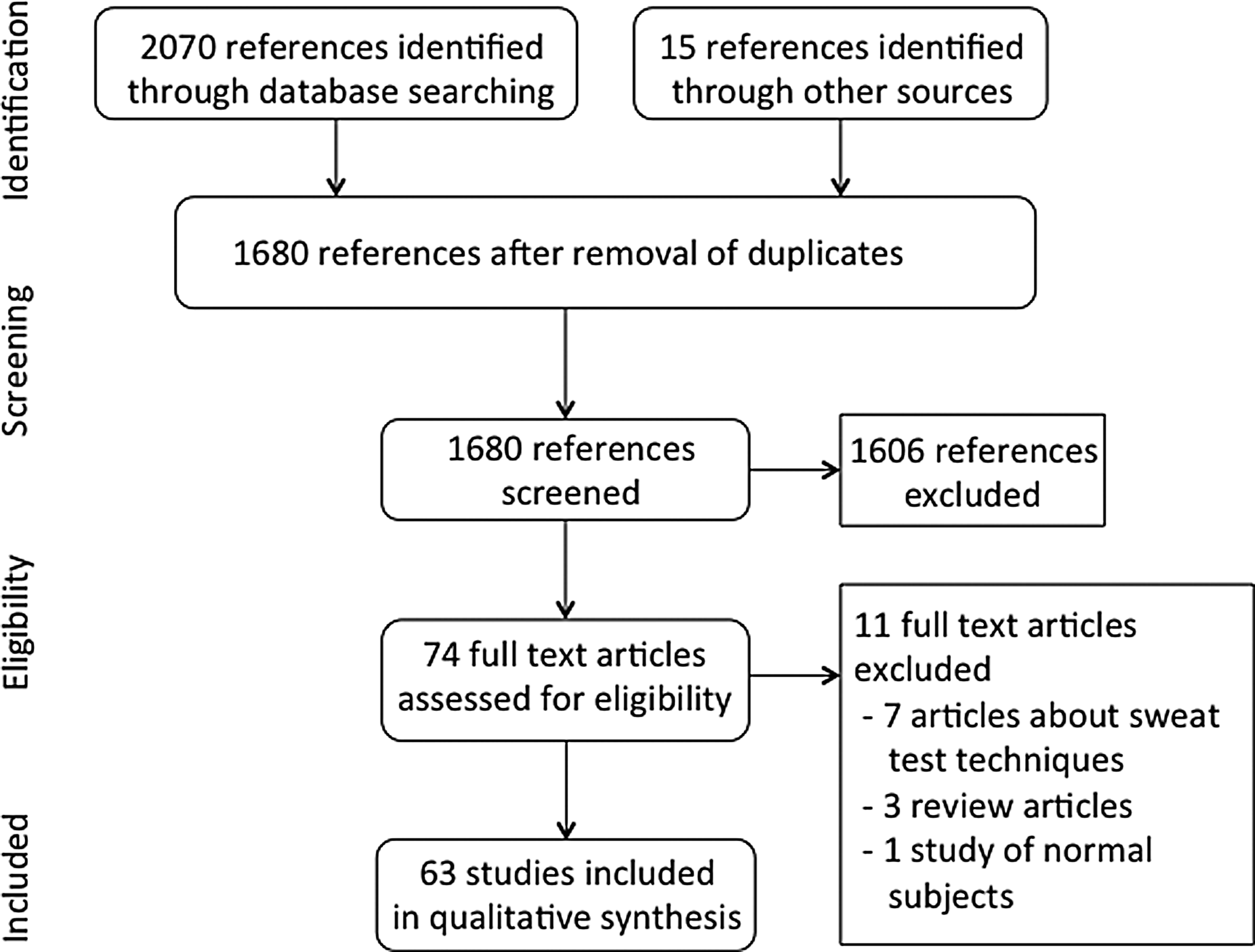
Results of the systematic review of the various reported causes of false-positive and false-negative sweat tests.
Analysis of Reports of False-Positive Sweat Tests
Technical factors
The updated CLSI guidelines document 1 provides details on the technical sources of error in measurement of sweat chloride concentration. LeGrys 4 reported that evaporation of sweat samples, contamination of the skin site, and erroneous dilution and calibration methods could result in false positive results. Foote et al. 5 reported the case of falsely positive elevation of sweat chloride in a patient for whom amethocaine (Ametop) gel was applied on the forearms as a local anesthetic before venipuncture. A repeat sweat test that was performed the next day after cleaning the skin in the same patient revealed normal results.
Dermatologic
Atopic dermatitis
Kibel 6 first reported atopic dermatitis as the cause of a false positive sweat test in a letter to the editor, where the author's experience with sweat testing in 10 patients with atopic dermatitis was described. While there were no details reported regarding the method of sweat testing, only 4 out of 10 subjects with atopic dermatitis had positive sweat tests (>60 mEq/L), and that too when the test was done on affected skin. The author did report normal sweat chloride results for those same individuals when testing was done on unaffected skin. The author also reported that they did not use weeping areas of the skin to avoid contamination with serum, and discontinued topical steroids 48 h before testing when performing sweat test on affected skin.
Subsequently, Brand et al. 7 published a case report of an infant with severe eczema and generalized lymphadenopathy in 1996 where they reported sweat test performed on the back and forearm of their index case, and found abnormal sweat chloride values on both locations. They concluded that their patient did not have CF (based on 13 panel test of CF mutations, and electrophysiological studies done from rectal biopsy specimen) and suggested that sweat testing should be done on unaffected skin only in individuals with atopic dermatitis. In response to this case report, Besnard et al. 8 wrote a letter to the editor in the same year reporting another case of a 5-month-old infant with protein losing enteropathy, recurrent pulmonary infections, generalized lymphadenopathy, hepatosplenomegaly, and severe eczema where they initially noted elevated sweat chloride concentrations (80 mmol/L), which subsequently became normal later in the course of admission (30 mmol/L). The authors were finally able to exclude CF in this patient based on nasal potential difference measurements, which were normal. However, no details regarding the method of sweat testing were provided in this report. Raeburn 9 also wrote a letter to the editor to comment on Brand et al.'s case report, but focused on communication with parents in such situations. Sweat testing on the back is not recommended, and it is important to avoid areas with eczema lesions on the forearms to avoid erroneous results.
Toxic
Arsenic toxicity
One recent report from Bangladesh 10 where groundwater is contaminated with arsenic and a significant proportion of the population has developed arsenic toxicity over time, elevated sweat chloride concentrations were noted in 11 individuals that did not have any other features of CF. This study used sweat conductivity (which is generally not recommended for diagnosing CF) for screening these individuals. For the 11 individuals with positive sweat conductivity results, further measurement of sweat chloride was followed by its analysis through an automated analyzer and it did show elevated concentrations. Genetic testing was done for these individuals and none of them were found to have 2 CF causing mutations. It is likely that this effect might be mediated through CFTR degradation by arsenic that has been shown to occur in vitro, and individuals with long-term arsenic toxicity have also been reported to have frequent gram-negative lung infections and development of bronchiectasis over time.
Psychosocial
Munchausen syndrome by proxy
The first report of an unusual case of Munchausen Syndrome by Proxy leading to an initial diagnosis of CF was by Orenstein and Wasserman, 11 where the child's mother manipulated the sweat test results and stool fat analysis to mislead the clinician. She fabricated the history by reporting symptoms consistent with CF, and was finally caught during her child's hospitalization when she tried to obtain a sputum sample from another CF patient in the hospital parking lot and pass it off as her own child's sample. Following this discovery, the child was removed from parents' custody for 6 months, and showed no further symptoms or signs compatible with CF and had rapid weight gain without any therapies. A more recent report by Leonard et al. 12 described the variability noted in patient's sweat electrolyte values and they found normal sweat chloride concentrations twice when the sweat test was performed in mother's absence. The authors reported using sweat potassium concentrations as a discriminatory factor as the mother may have tried to contaminate the skin site to fabricate the sweat test results. These reports highlight the need to be vigilant about the technique for performing the sweat test.
Environmental deprivation/psychosocial failure to thrive
Christoffel et al. 13 reported 5 cases of elevated sweat chloride levels in children with environmental deprivation. All patients underwent sweat testing during a clinical workup for failure to thrive. Sweat testing was done via the Gibson/Cooke method. They present the case of 1 child noted to have failure to thrive, with subsequent improvement while under care. They also presented data from 4 other similar cases. The children ranged in age from 1 to 6 years and all had evidence of environmental deprivation. All had elevated sweat chloride levels initially and normalized shortly after they were identified, before significant weight gain. The authors acknowledge that intermediate sweat chloride levels are often difficult to interpret, and any patient who does not follow a course typical of CF should undergo repeat testing. They also recognize that environmental deprivation is extremely rare as a cause of elevated sweat chloride, and that it is more likely for a patient with elevated sweat chloride levels, clinical illness, and environmental issues to have a diagnosis of CF in addition to requirement for social services. While this evidence does not indicate environmental deprivation as a significant cause for false positive sweat testing, it does reiterate the need for repeat testing in patients with an atypical course and could be considered as a possible source of false positive levels in patients with signs of abuse or neglect. Further studies are needed to confirm this association.
Ruddy and Scanlin 14 identified the case of an infant with failure to thrive related to psychosocial circumstances. The infant presented to them for care due to failure to thrive, along with frequent respiratory infections and a positive sweat test. His symptoms began in the second year of life and he required hospitalization at 18 months due to diarrhea and failure to thrive. He was able to gain weight while hospitalized, but subsequently lost weight again after discharge. Sweat chloride concentration remained elevated during this time of weight loss. On second admission, he had adequate weight gain, and at that time social issues including limited food resources were reported by the family. When caloric intake was restored, his sweat chloride levels normalized, and he was noted to be growing well at 9-month follow-up. As an isolated case report, this is not strong evidence for psychosocial failure to thrive as a cause of false positive sweat tests. However, it does support the need for thorough social history during evaluation. Inadequate caloric intake of various causes may cause false positive results in sweat testing, but more data would be helpful in confirming the association.
Gastrointestinal
Celiac disease
Ruddy and Scanlin 14 described a single case of celiac disease where there was improvement in sweat chloride concentrations noted after initiation of gluten-free diet. This patient had a previously reported normal sweat chloride result of 20 mEq/L, but at the author's institution repeat testing done at admission by Gibson Cooke method had shown a sweat chloride value of 115 mEq/L with low fecal trypsin activity, and blunting of villi on intestinal biopsy. Repeat sweat tests done for the same patient after gluten-free diet were 46 and 49 mEq/L, thus prompting the authors to conclude that Celiac disease is a cause of false positive sweat test. The authors did not perform any genetic testing for this patient but reported improvement in malabsorption and weight gain on a gluten-free diet. They did not speculate on the possible mechanism by which celiac disease may lead to false positive sweat tests.
Neurologic
Autonomic dysfunction
Esterly et al. 15 reported a single pediatric case of Holmes-Adie pupil with abnormal sudomotor innervation that led to several areas of hypohidrosis for this patient. Sweat testing was done in this patient by overnight collection or by exposure to heat, and there was significant variability noted. They also discussed another case with similar findings that also had elevated sweat chloride concentration, although in this latter case sweat testing was done by pilocarpine iontophoresis. Because there was variability in the sweat chloride concentrations of the sweat collected from various body sites of this index case, it is not clear whether this can be truly associated with false positive sweat test.
Medications
Topiramate use
This was a case series published in 2011 by the authors as they noted that patients on topiramate therapy tend to have elevated sweat chloride concentrations. 16 A total of 21 children on topiramate therapy showed elevated sweat chloride concentrations when compared to 20 normal controls that were not receiving this medication. While topiramate did not appear to affect CFTR function in human bronchial epithelial cells, the authors postulated that this effect of topiramate might be mediated via inhibition of carbonic anhydrase (CA) isotypes in the sweat gland ducts.
Prostaglandin E1 infusion
Silverman et al. 17 reported a case of an infant with complex congenital heart disease and multiple congenital anomalies (VATER association), who had sweat testing performed using the Gibson–Cooke method multiple times while he was on prostaglandin E1 infusion. Immediately after its discontinuation on day 58 of life, subsequent sweat chloride values on day 59 and 63 were still elevated (79 and 70 mEq/L), but reverted to normal when tested on day 120 and 151 of life (19 and 13 mEq/L). The infant ultimately died due to sepsis and chronic respiratory failure at 11 months of age, but the authors were unable to repeat this observation in any other case. There have been no further reports regarding this association.
Nutritional
Anorexia nervosa
Luthi and Zurbrugg 18 reported a single case of a 14-year-old girl who presented with initial complaint of malabsorptive symptoms, including postprandial abdominal pain, belching, and loose stools. Symptoms were initially attributed to lactose intolerance, but persisted despite nearly lactose-free diet. She was noted to be 4 standard deviations below her expected weight-for-age, and 1.75 standard deviations below her expected height-for-age. She was hypothermic, bradycardic, and hypotensive on presentation. Initial sweat chloride levels were performed by pilocarpine iontophoresis and were significantly elevated. The child was eventually diagnosed with anorexia nervosa and underwent refeeding via tube feeds, and psychotherapy. Her sweat chloride levels returned to normal range after appropriate treatment.
Beck et al. 19 performed a follow-up prospective study of 17 patients with anorexia nervosa during their hospital stay by performing sweat testing using urecholine iontophoresis. Serum trypsinogen and amylase assays, and thyroid function tests were also performed. Thirteen patients were found to have elevated sweat chloride levels, 8 of which were abnormal (>60 mEq/L) and 5 were between 50 and 60 mEq/L. Clinical status in all patients improved with appropriate inpatient caloric administration. Seven patients were retested and 4 had normal sweat chloride levels, 1 had decrease in her level to intermediate range. Only 1 patient with no psychological improvement and continued nasogastric tube feeds had persistently elevated sweat chloride level. While there are a small number of patients reported, it should be considered in the appropriate clinical setting. Larger studies would help to confirm this association.
Protein calorie malnutrition
Mace and Schanberger 20 were the first to report a case of severe malnutrition that had 4 initial abnormal sweat test results (all were performed by Gibson–Cooke method), which became normal 2 years after he had been on pancreatic enzyme replacement therapy. The patient's enzyme replacement therapy was discontinued and the initial abnormal sweat test results were attributed to his malnutrition. Rodrigues et al. 21 conducted a cross-sectional study of 32 healthy children and 36 children with malnutrition where they measured sweat electrolytes using Gibson–Cooke method. While none of the normal or malnourished children had abnormal sweat chloride values (>60 mmol/L), there were 2 normal controls and 6 malnourished children with intermediate sweat chloride values. The authors also reported that all the malnourished children had sweat sodium to chloride ratio of <1, and the sum of sweat sodium and chloride never exceeded 140 mmol/L. Beck et al. 22 retrospectively analyzed all the sweat tests performed over a 2-year period and found that of the 14 subjects without CF that had malnutrition at the time of testing, 11 had abnormal results (>60 mmol/L), which reverted to normal after improvement in their nutritional status. More recently, Yigit et al. 23 used sweat test conductivity in a cohort of 90 children with various grades of protein calorie malnutrition (PCM) and found that 6 (20%) of those with Grade 3 PCM had abnormal sweat conductivity values. All the patients showed normal results after recovery from the acute phase of malnutrition. Since genetic testing was not performed in any of these reports, it is not possible to confirm the diagnosis of CF in any of the subjects.
Immune
Hypogammaglobulinemia
Corkey and Gelfand 24 reported 3 patients with immunoglobulin deficiencies who had elevated sweat chloride concentrations detected via urecholine iontophoresis-based sweat tests. One patient had initial elevated values followed by intermediate values later; while another had normal values of sweat chloride on follow-up. The third patient had persistently elevated sweat chloride results. None of these subjects had genetic testing done and no specific immunodeficiency syndrome was diagnosed in any of the 3 patients. The authors concluded that the initial diagnostic work up of any patient with recurrent respiratory infections should include an assessment of immunoglobulin levels besides a sweat test to rule out CF. However, the variability seen between these 3 patients and the lack of genetic testing makes it difficult to confirm hypogammaglobulinemia as the cause of elevated sweat chloride concentrations.
Systemic lupus erythematosus
Hadler et al. 25 published a report in 1972 of a 23-year-old male patient with systemic lupus erythematosus (SLE) who was found to have elevated sweat chloride levels. He presented with renal disease and was found to have hypokalemia out of proportion to the degree of renal impairment, diagnosed with a disorder of potassium excretion. He underwent a series of electrolyte studies, including sweat electrolytes. His sweat chloride by pilocarpine iontophoresis was elevated, within the diagnostic range for CF. The authors did perform sweat testing on 7 additional males with SLE, all had normal sweat levels. It seems that this patient had an abnormality of membrane electrolyte transport affecting a number of cell types. This is not compelling evidence for elevated sweat chloride as sequelae of SLE and more evidence is needed to determine a relationship among the broader population with SLE.
Genetic
Carbonic anhydrase XII mutations
A more recently reported cause of elevated sweat chloride concentrations was first described by Feldshtein et al. 26 in 2010 where they reported an Israeli Bedouin kindred with 7 individuals that had a history of hyponatremic dehydration, poor feeding and slow weight gain in infancy, and elevated sweat chloride concentrations. The pattern of inheritance was suggestive of autosomal recessive heritability, and the authors performed genome-wide linkage analysis for the affected individuals and multiple other family members. Further sequencing of the candidate genes identified the same mutation in CA XII gene, with carriers also showing single copy of the mutation. Of the 16 different subtypes of CA reported in mammals, CA XII is membrane bound and has been found in normal human skin, lung, kidney, prostate, colon, pancreas, ovary, testis, eye, and brain. The authors found this homozygous missense mutation of CA XII to be associated with 70% of the CA activity as compared to the wild type.
Around the same time, another report emerged from Israel 27 that reported similar Bedouin kindred from a different village that had the same homozygous CA XII mutation and multiple members had significantly elevated sweat chloride values with features of salt-craving, but no other features suggestive of CF. An addendum at the end of this report acknowledged the report by Feldshtein et al. and clarified that this was a different family from the one previously reported. It was interesting to note that sweat chloride values ranged between 60 and 279 mEq/L in this kindred, whereas the highest value in Feldshtein kindred was 156 mEq/L. The value of 279 mEq/L reported by Muhammad et al. is highly questionable and may represent technical errors (possible partial evaporation of sweat sample leading to highly concentrated sample).
Pseudohypoaldosteronism
Hanukoglu et al. 28 described 4 patients with pseudohypoaldosteronism secondary to end organ resistance to aldosterone. They all had persistently elevated sweat chloride levels despite therapy. They all also had multiple episodes of lower respiratory tract infections, most frequently during salt wasting episodes. Mora-Lopez et al. 29 similarly described a patient with CF-like presentation, including recurrent lower respiratory infections and elevated sweat chloride, and additional finding of steatorrhea. The patient was initially diagnosed with CF. However, lab values showed hyponatremia and hyperkalemia, raising suspicion for low aldosterone function. Genetic testing was negative for CF, but a mutation related to aldosterone function was discovered. These 5 cases do not provide conclusive evidence of false positive sweat testing in pseudohypoaldosteronism, but the mechanism of disease does make it a likely culprit of false positive tests. Further testing would help to establish this relationship.
Hidrotic ectodermal dysplasia
Familial ectodermal dysplasia is a disorder of teeth, nail, and hair abnormalities. It can be divided into hidrotic and anhidrotic subtypes. The hidrotic form is associated with a variety of congenital anomalies. Robinson et al. 30 presented the pedigree of a family affected by hidrotic type ectodermal dysplasia, manifesting in various family members with symptoms such as sensorineural hearing loss, polydactylism, and syndactylism. In addition, they performed sweat testing on the 5 siblings and their father. Of the 4 affected siblings, 2 showed elevated sweat chloride levels and 2 showed intermediate levels. Only the father and unaffected sibling had normal sweat chloride levels. While the possible impairment of sweat gland function due to ectodermal dysplasia may provide an explanation for abnormal sweat chloride levels, this result has never been reproduced again in any other report. The first author has personally seen 1 patient with ectodermal dysplasia who underwent sweat testing but did not produce any sweat at all when pilocarpine iontophoresis and Macroduct method were used. Hence, the results from Robinson et al. cannot be generalized for all patients with ectodermal dysplasia and further investigation is required to determine any association.
Fucosidosis type 1
Durand et al. 31 first reported in 1969 the diagnostic studies for 2 siblings with Fucosidosis who had abnormal elevation of sweat chloride concentration, although both of them subsequently had normal sweat tests just before they died. Fucosidosis is characterized by abnormal skin (angiokeratoma corporis diffusum) with anhidrosis, progressive mental and motor retardation, growth abnormalities, and hepatosplenomegaly. The authors described the deposition of an abnormal of material between dermis and hypodermis, which they felt could have altered the sweat electrolytes. No details were provided about the method of sweat collection or determination of chloride concentration in these 2 patients. Later in 1991, Rubin et al. 32 described a case of Fucosidosis who initially had a normal sweat test, but subsequent retesting done on involved and uninvolved areas of the skin (not clear from what parts of the body) showed that sweat chloride was normal from angiokeratotic lesions, but abnormal from uninvolved skin in this patient. The skin biopsy from this patient was reported to have abnormal sweat glands with foamy cells lining the sweat ducts. It is likely that Fucosidosis does cause some changes in sweat electrolyte composition, but the data is based on a very small number of cases.
Familial cholestasis
Lloyd-Still 33 described 2 siblings with cholestatic jaundice and elevated sweat chloride values detected by Gibson–Cooke method. The first child had normal initial sweat tests up to 6 months of age and remained abnormal thereafter, while the second sibling was tested only after 6 months of age and his values remained elevated throughout. Interestingly the author also reported the sweat chloride values for a normal sibling with no liver disease and their parents, and they all showed intermediate elevation of sweat chloride in the 40s. Even though the liver biopsy did not show changes that were believed to be characteristic of CF at that time, no genetic testing was available at that time to confirm the diagnosis.
A year later, Hillemeier et al. 34 described a case of familial progressive intrahepatic cholestasis that also had normal sweat chloride values in the newborn period, but was found to have persistently elevated sweat chloride concentrations at 12 years of age. His sibling with the same liver disease had normal sweat chloride values at 7 years of age. The index case also had history of meconium peritonitis at 4 weeks of age, which the authors speculated might have been related to the patient's liver disease.
Glycogen storage disease type 1
Harris and Cohen 35 reported sweat chloride values in 5 children with glycogen storage disease type 1 (glucose-6-phosphatase deficiency) and noted that all men had intermediate or elevated sweat chloride levels, the 2 women with this disorder had normal sweat tests. The authors reported that all their patients had salt craving, and large bulky stools, but reported intestinal trypsin measurement being normal for 1 subject in which it was measured. They hypothesized that because of the risk of hypoglycemia these children are fed constantly and develop hyperlipidemia, which causes them to have higher electrolytes in extracellular fluid. As a result their sweat chloride is said to be elevated, although they did not explain the differences in sweat chloride concentrations seen between the male and female patients with this condition.
Keratosis, icthyosis, and deafness syndrome
Kumar et al. 36 reported a single case of a 4-year-old boy with keratosis, icthyosis, and deafness syndrome who had 3 sweat tests that were >60 mmol/L, and had negative results from genetic mutation testing for 16 of the most common CFTR mutations. This child was born with a collodion membrane, which was shed after 10 days with underlying abnormal skin that showed features consistent with atypical erythrodermic type of ichthyosis. Because this patient had recurrent pulmonary infiltrates, failure to thrive, and a positive family history of CF, sweat test was performed as part of his diagnostic work up. The authors did try to exclude other causes of false positive sweat test in this patient, but no clear explanation was put forth for the elevated sweat chloride concentration. It is likely that similar to atopic dermatitis, this syndrome involving the skin may have affected sweat gland activity leading to falsely elevated sweat chloride concentrations.
Mucopolysaccharidosis
The report by Durand et al. 37 has been cited for the presence of abnormal sweat chloride concentrations in patients with mucopolysaccharidosis. However, there is only mention of persistently abnormal sweat tests in 2 of the patients in this report, and no specific details were provided regarding the method of testing or the degree of elevation of sweat chloride that was seen in these patients. Hence, this should be confirmed with additional testing in patients with this condition before it can be validated as a true false positive elevation of sweat chloride concentrations.
Klinefelter's syndrome (47XXY)
A case of elevated sweat chloride level in a patient with 47XXY chromosomal abnormality and a number of other symptoms was described by Grand et al. (1966). The patient was a full term infant with initial normal development who developed failure to thrive, recurrent pulmonary infections, and bulky stools consistent with malabsorption shortly after birth. Malabsorptive symptoms improved when given pancreatin. The patient was diagnosed with CF as a child due to these findings. The patient had elevated sweat chloride levels initially and multiple repeat studies after that, some of which showed chloride levels in normal range. Additional findings in this patient throughout his clinical course included progressive deafness, facial abnormalities, seizures, absence of sexual maturation without supplemental hormone therapy, and hypothyroidism.
The authors noted that many of his symptoms had been described previously in Klinefelter's syndrome (47XXY), but pancreatic insufficiency had not been reported. They studied the patient as an adult and found inconsistencies with diagnosis of CF, including the lack of progressive lung disease, copious pulmonary secretions, persistent wheezing, and normal sweat chloride on some occasions. In our opinion, this case report is little evidence to support findings of false positive sweat testing in patients with Klinefelter's syndrome. This patient had a number of atypical symptoms and cannot be generalized to the broader population of patients. Additional studies are needed to determine any relationship between Klinefelter's syndrome (47XXY) and false positive sweat testing.
Triosephosphate isomerase deficiency
Yenicesu et al. 38 described the case of a 15-month-old patient with malnutrition, hemolytic anemia, muscle weakness, and progressive respiratory failure, which also had elevated sweat chloride concentrations at presentation. She had low hemoglobin level, 15% reticulocytosis, significant stomatocytosis on peripheral smear, and her vitamin E levels were also noted to be low. After the first 2 sweat tests were abnormal, she had genetic testing done by gene sequencing, which did not show any CFTR mutations. A repeat sweat test done later in the course was normal, and the authors felt that it may have been related to improvement of her nutritional status with parenteral nutrition. Further evaluation of her hemolytic anemia led to the diagnosis of Triose Phosphate Isomerase deficiency. Because this is a rare condition, it is unclear from this report if it was the initial malnutrition at presentation or the actual enzyme deficiency that was responsible for the falsely positive sweat tests noted initially in this patient.
Mauriac syndrome
Rosenfeld et al. 39 reported a single case of 6-year-old girl with type 1 diabetes who presented with severe edema, malnutrition and hepatomegaly, and also had features suggestive of diabetic ketoacidosis at admission. Sweat chloride was abnormally high on day 3 of admission, and even though it was collected by Gibson–Cooke method, the sweat sample was diluted with lithium sulfate. Subsequent repeat sweat chloride levels after initiation of insulin therapy showed normal levels. Therefore, it is unclear from this report whether the malnutrition, state of diabetic ketoacidosis, or perhaps underlying liver dysfunction was contributing to the abnormal sweat electrolytes. However, reversal of the results to normal after initiation of insulin therapy suggests that this transient elevation of sweat chloride concentrations does not appear to be related to the diabetic state but more likely due to the malnutrition that this patient had. Even though diabetes can be a part of CF, this patient had no features of malabsorption, and genetic testing was not available at that time. Another report by Polack et al. 40 also suggested that the transient elevation of sweat chloride values seen in Mauriac syndrome may be due to the associated malnutrition, and less likely to be due to the syndrome itself.
Trisomy 21
Pop et al. 41 described the case of a child with Down syndrome, cholelithiasis, and elevated sweat chloride levels. During the course of admission chest X-ray showed a right upper lobe opacity and sweat test was performed, showing elevation on 2 separate occasions. Genetic testing confirmed Trisomy 21 with robertsonian translocation, but was negative for common CF genes. This patient was not reported to have recurrent respiratory illness or symptoms of malabsorption. This case report does not provide compelling evidence of false positive sweat testing in patients with Trisomy 21. More information regarding the patient's clinical course, including any development of new symptoms and repeat sweat chloride testing would be helpful in determining the relevance of this case. Studies evaluating sweat chloride levels in patients with Trisomy 21 as compared to the general population and those with CF would be necessary to establish an association.
Shwachman–Diamond syndrome
Brown and Buchdahl 42 reported a single case of an infant with failure to thrive and pancreatic insufficiency who initially had an elevated sweat chloride concentration, but became normal on repeat testing on 2 other occasions. The patient was eventually confirmed to have mutations causing Shwachman–Diamond syndrome. The child's mother had cleaned the child's arms with holy water from Lourdes River before the sweat tests, which may have possibly contributed to the initial abnormal sweat test. Besides other associated abnormalities, Shwachman–Diamond syndrome can have similar presenting features (due to pancreatic insufficiency), and should be considered in the differential diagnosis of CF. However, other than this isolated case report (where there was likely a technical error in the first sweat test) there are no reports of sweat chloride concentrations being abnormal in children with this syndrome.
Endocrine
Untreated hypothyroidism
In 1968, Madoff 43 described a patient who presented with failure to thrive, intractable vomiting, and rash within the first few months of life. Sweat chloride test was positive during the workup for failure to thrive and the patient was treated with replacement enzymes and respiratory intervention. He continued to be symptomatic and was subsequently found to be hypothyroid and placed on replacement hormones, with normalization of sweat chloride after reaching therapeutic doses. Strickland 44 subsequently performed sweat electrolyte testing on 13 patients with hypothyroidism and found elevated sweat electrolytes in 5 of them, including 2 of 12 with elevated sweat chloride. All results normalized after treatment with thyroid hormone replacement.
Squires and Dolan 45 described a 11-year-old girl with poor growth, persistent cough, and cold intolerance, found to have elevated sweat chloride on laboratory evaluation. She was also found to have autoimmune hypothyroidism. They proposed thyroid hormone effect on chloride channels as a possible mechanism. While larger trials would help to establish a relationship between untreated hypothyroidism and sweat chloride, these reports support the need for repeat testing and an index of suspicion in patients with elevated sweat chloride, particularly if they have clinical signs of hypothyroidism or fail to respond to treatment.
Hypoparathyroidism
Morse et al. 46 described a family of individuals with hypoparathyroidism who were found to have elevated sweat chloride levels. Five of 11 siblings were affected with hypoparathyroidism, abnormal dentition, and significantly elevated sweat chloride levels. Four siblings had pernicious anemia and 2 had steatorrhea. Since there is only 1 report limited to 1 family, more studies are needed to determine the effect of hypoparathyroidism on sweat chloride values.
Untreated Addison's disease
Chan and Gwee 47 published the case of a single patient who presented with darkening skin and salty sweat, found to have low blood pressure, hyponatremia and hyperkalemia during workup. Due to his complaint of salty tasting sweat while working, sweat test was performed. The sweat chloride on a sample obtained from his back was elevated at 71 mmol/L. He was diagnosed with Addison disease and started on glucocorticoid and mineralocorticoid therapy. Upon repeat sweat testing, his chloride level had normalized. A single isolated case study does not provide sufficient evidence of association between untreated Addison disease and elevated sweat chloride and the sweat collection in this patient was performed on the back, which is no longer considered an acceptable method. However, the pathology of this disease makes elevated sweat electrolytes a plausible finding. A larger study of patients with Addison disease is necessary to determine whether this is a common cause of false positive sweat chloride levels.
Renal
Nephrogenic diabetes insipidus
Lobeck et al. 48 described a single case report of a boy with nephrogenic diabetes insipidus that had shown consistently elevated sweat chloride level that reverted to normal after the initiation of diuretic therapy. Sweat was collected by pilocarpine iontophoresis with Gibson–Cooke method on several consecutive days, before and after the initiation of therapy.
Pyelonephritis
A single report 49 of a child with single kidney who developed pyelonephritis had abnormal sweat test result during the acute phase of the illness, but became normal 3 weeks after treatment with IV antibiotics. This patient showed normal pancreatic function, negative respiratory cultures, and negative results for CFTR genotyping. Given that there are no other similar reports and the patient had normal subsequent sweat test results, it is less likely to be a true case false positive elevation of sweat chloride concentrations.
Analysis of Reports of False-Negative Sweat Test
Technical factors—dilution of sweat sample
Dilution of the collected sweat specimen with deionized/distilled water drops that are used to clean the skin after the pilocarpine iontophoresis can falsely lower the sweat chloride concentrations. Normally, the skin should be allowed to dry completely after the application of deionized water, and only then should the collection device be put on the skin. Inappropriate processing of the sweat sample in the lab with improper measurements of acid diluent may also lead to falsely negative sweat test results.
Technical factors—inadequate sweat production
The minimum volume required for adequate analysis of sweat chloride concentrations requires at least 15 μL per arm using the Macroduct method; or at least 75 mg when collected using the Gibson-Cooke method. Barnes and McNaught 50 reported a review of sweat chloride testing performed at their hospital over a 10-year period. At the time of their report, 50–100 mg of sweat was considered adequate for diagnosis of CF. The authors compared results of 68 patients who had multiple sweat tests performed. All patients had sweat tests that produced more than 100 mg of sweat and at least 1 test with <100 mg of sweat production. In patients with less than 50 mg sweat produced, there were 15 with false negative tests, later confirmed to have CF after repeat testing. Two were reported in the “doubtful” range, with results of 50–70 mmol/L. These confirmed previous findings. They also found 5 false negative tests and 3 doubtful tests among children with 50–99 mg of sweat, later confirmed to have CF on repeat testing. This indicates that higher amounts of sweat production improve accuracy of sweat chloride testing.
Specific mutations
Highsmith et al. 51 performed laboratory evaluation by polymerase chain reaction of messenger RNA of 23 patients with clinical diagnosis of CF with negative sweat chloride testing. They found that 13 of those patients from 8 families and 3 different ethnic backgrounds carried the same mutation, 3849 + 10 KbC→T. This indicated that the aforementioned gene could be contributing to the clinical picture of false negative test results and clinical disease.
Castellani et al. 52 reported the cases of 2 patients with persistent hypertrypsinogenemia at birth but negative sweat chloride levels on sweat testing. The patients both continued to have poor growth and respiratory symptoms, and colonization by typical bacteria. They underwent genetic testing due to continued concern for the disease. The first patient was found to have R553X and D1152H mutation. The second was found to have compound heterozygosity for F508del and 3849 + 10 KbC→T.
Padoan et al. 53 did a retrospective chart review to evaluate false negative sweat tests in their institution over a period of 5 years and 9 months. They found 6 infants who were labeled as false negatives during infancy, 5 of whom were carriers for ΔF508. They all returned with symptoms and signs consistent with CF. On further genetic testing, they found the following mutations: R117H (3 patients), 3849 + 10 KbC→T, R117L, L997F, and A309D. All infants were subsequently diagnosed with CF. Only 2 had repeat sweat chloride levels within the diagnostic range, while 1 additional patient had an increase from previous sweat chloride without being in diagnostic range.
Tummler et al. 54 reported a case of a patient with the R553X/F508del-R5553Q mutation, who had initially normal sweat chloride levels despite classic clinical features of CF. Due to this fact, the diagnosis was delayed until age 7 when her sweat chloride levels were measured at 100–120 mmol/L.
Hypohidrotic ectodermal dysplasia
Welsh et al. 55 reported an isolated case of a child with failure to thrive and chronic cough, suspected of having CF. He underwent multiple sweat tests before sufficient sweat quantity was obtained. It revealed a normal sweat chloride level. Due to continued concern for CF, genetic testing was sent and he was found to have 3 mutations known to be associated with CF. He was subsequently diagnosed as having the disease. However, his clinical picture was complicated by hypohidrosis, hypotrichosis, and conical teeth. Further genetic testing revealed hypohidrotic ectodermal dysplasia. The low sweat output from this disease seemed to play a part in the difficulty of diagnosis and potentially contributed to his false negative test. This is in contrast to case reports of children with the hidrotic form, who may have false positive tests. More information regarding sweat chloride levels of children with ectodermal dysplasia is needed.
Mineralocorticoid treatment
Treatment with mineralocorticoid agents can lead to reduction in measured sweat sodium concentrations in normal individuals, but was believed to cause no change in patients with CF. The fludrocortisone suppression test was first reported in 1983 as a means to investigate whether administration of 5 mg dose of fludrocortisone in adults with elevated sweat sodium concentrations is able to suppress their sweat sodium levels to the normal range.
9-alpha-fludrocortisone is a synthetic mineralocorticoid with moderate glucocorticoid potency that is used for the treatment of adrenal insufficiency and other disorders associated with low blood volume (postural orthostatic tachycardia syndrome). In normal individuals, a loading dose of fludrocortisone is expected to suppress serum aldosterone levels, which may have an impact on their sweat chloride concentrations, but individuals with CF do not show this response. The study by Hodson et al. 56 included 25 adults with CF and 25 normal controls, and the authors only studied changes in sweat sodium concentrations and not chloride concentrations.
However, Pereira and Orson 57 reported their experience with use of 9-alpha-fludrocortisone in children with CF and measured sweat sodium concentrations before and after the administration of this agent for 2 days. They noted that sweat sodium concentrations increased by >30% in 3 out of 7 subjects with CF, and 1 subject had a 10.8% increase. Again the usefulness of this test for all age groups and conditions needs to be studied further.
Young age
Multiple authors have documented false negative results when performing sweat testing on young infants. Roberts et al. 58 also commented on this during a study evaluating the use of immunoreactive trypsinogen (IRT) for newborn screening. Sweat testing was performed as a confirmatory test on all infants with 2 raised IRT levels. They noted 8 infants with normal to intermediate levels, which were subsequently found to have elevated sweat chloride levels. However, no further information is provided, as this was a secondary finding in their study.
Doughty et al. 59 described a single case of a child with positive IRT level on newborn screen and family history of CF in a sibling. He underwent sweat testing at 6 weeks of age, which showed normal sweat chloride. Repeat IRT remained elevated. He had poor growth without respiratory or malabsorptive symptoms until age 2. Repeat sweat testing at age 2 showed elevated sweat chloride. These results indicate the importance of repeat testing, particularly with high clinical suspicion of CF and initial testing done at a young age.
Parad et al. 60 studied sweat quantities and levels in 1,214 infants who were reviewed by newborn screening methods. They found that the majority of infants (80%) had sufficient sweat quantity for testing. They also reported a linear regression curve of mean sweat values by age in weeks at testing. They found that most infants are able to produce adequate sweat by 2 weeks of age. Given the time from birth to reporting of newborn screen results, it is unlikely that many infants have testing performed before 2 weeks, and they are more likely to be tested within 2–3 weeks of life. While the testing on these infants may produce adequate samples, technical difficulty based on age could still contribute to false negative tests. More data is needed to confirm this.
Edema
MacLean and Tripp 61 reported the case of an infant with CF who had normal sweat electrolyte levels during an episode of edema. The infant was born full term with no complications, but subsequently developed many episodes of loose stools. Dietary change provided some relief, but the infant required hospitalization shortly thereafter due to significant edema. He also had frequent cough. Family history was positive for CF in a sibling. The child had low sweat chloride levels during the episode of edema, but after therapy, levels were elevated. They remained elevated on recheck at 17 months of age.
Vlachos 62 subsequently reported on an infant with similar findings. She was a full-term infant, admitted to the hospital at 10 weeks of age with edema, cough, and pallor. She was found to be anemic and hypoalbuminemic, but was discharged home after replacement of blood and protein and a course of antibiotics. Sweat chloride levels at that time were within normal limits. She returned to the hospital 3 weeks later and was diagnosed with bronchopneumonia. Sweat chloride tests were repeated and she had 2 tests with significantly elevated results.
Guglani et al. 63 recently reported the results of sweat tests performed in children with acute onset idiopathic nephrotic syndrome who had presented with diffuse edema and had sweat testing performed within 24 h of admission. Initial sweat tests performed when the subjects were edematous and follow-up testing done in the same subjects 3 months later when their nephrotic syndrome was in remission showed normal results.
Hypoproteinemia
There have been a few case reports61,64 of false negative sweat testing in children with CF and edema, for which hypoproteinemia has been postulated as the cause. A recent study by Guglani et al. 63 (see previous section on Edema) for sweat tests done in patients with acute onset idiopathic nephrotic syndrome (which is generally associated with significant edema and hypoproteinemia as well) did not show any significant change in sweat chloride concentrations in paired samples of 8 patients during acute phase of the disease and during its remission.
Penicillin therapy
Griffiths and Bull 65 reported the case of a child who had negative sweat testing while undergoing cloxacillin therapy. She had multiple admissions early in life due to respiratory and gastrointestinal complaints. She had elevated fecal fat at 3 years of age, but no intervention occurred at that time. She continued to be symptomatic, particularly with respiratory complaints, and was seen by the author at 11 years of age. Multiple sweat tests were negative, but subsequently became positive after discontinuation of antibiotic therapy. Notably, the first sweat test had normal sweat chloride and the patient was not on antibiotics at that time. The author does comment, however, that the sample may have been of an insufficient quantity of sweat. This single case does not prove a causative effect between penicillin therapy and sweat test outcomes. It is prudent to consider medication effects on testing, but further studies would indicate whether or not this was an isolated event.
Discussion
We have separated the causes of false positive and false negative sweat tests based on a systematic review of the available literature (Table 1) into 3 categories of “likely,” “probable but needs validation,” and “unlikely” based on the number of cases reported and use of genetic testing to exclude CF. While many of these conditions are rare and not generally seen in day to day practice, it is important to have a comprehensive understanding of all the factors that affect sweat chloride testing. In the current era of advanced genetic testing capabilities, it is possible to reduce the likelihood of missing true cases of CF through confirmatory genetic testing. However, there is still a very small chance of missing previously unreported mutations that may not be detectable by current testing methods. Further assessment of patients with suspected false positive sweat tests may be required to help identify potential underlying causes of false positive sweat tests when the diagnosis of CF has not been established through conventional tests. Cystic Fibrosis Foundation guidelines for diagnosis of CF 2 suggest that the sweat test should be repeated at least one more time on a different day for confirmation, as there have been reports of transient elevation of sweat chloride concentrations that have subsequently become normal.
Rosenstein and Langbaum 66 described their experience at a single center where 277 patients were evaluated over a 15-year period (1971–1985) and in 8 patients who had initially elevated sweat chloride concentrations subsequent testing revealed normal sweat chloride values. All these 8 subjects had shown at least 2 positive sweat tests that had been done in other centers before their referral. Given that this report is from the era before the discovery of the CF gene, none of these subjects had undergone any genetic testing to assess for any of the mutations that may be associated with normal sweat chloride concentrations (see Table 1). In addition, genetic testing may not be necessary in every patient if the diagnosis can be established on the basis of clinical features and abnormal sweat chloride concentrations and/or other ancillary tests (such as nasal potential difference, rectal biopsy to measures CFTR activity in Ussing Chamber, lung function testing, chest imaging, respiratory cultures, bronchoscopy, etc.). However, some of these ancillary tests (such as nasal potential difference measurements) may only be available at a limited number of centers.
Therefore, it is important to ensure that an abnormal sweat test result in the absence of other supporting clinical evidence for CF should be repeated. This has been noted in several individual case reports for conditions such as Addison's disease, Pyelonephritis or Shwachman–Diamond syndrome, where 1 initial sweat test was abnormal, but subsequent ones remained normal. It is also interesting to note that 1 of the subtypes of ectodermal dysplasia (hidrotic type) has been identified as a cause of false positive sweat test, whereas the hypohidrotic form of ectodermal dysplasia may cause a false negative sweat test. It could be related to the differing skin manifestations of this condition, but this condition is very rare and as long as sweat testing is not being performed on abnormal skin surfaces, it should not lead to confusion in most clinical situations.
Similarly in situations where there are clinical features suggestive of CF, but the sweat test remains negative, other investigations may be required and could include repeating the sweat test several times, excluding other conditions that are known to be associated with a false negative sweat test result (as shown in Tables 1 and 2), and CFTR genotyping or gene sequencing to look for the presence of CFTR mutations that are either associated with normal sweat chloride concentrations or may not have been recognized/reported before. If genetic testing is inconclusive, then ancillary tests to check for CFTR dysfunction should be considered.
This review has several limitations in that majority of publications included are from the era before genetic testing became available for CF. That limits the ability of many of these publications to rule out CF in their reported cases before attributing the conditions as a cause of false positive/false negative sweat test with any degree of certainty. Majority of these cases are from several decades ago and patient follow-up and outcomes may no longer be available. Even though we performed an extensive review of the literature, there is a possibility that we may have missed a few publications/conditions. The grading of the evidence regarding each of the conditions is somewhat subjective and may have to be based on more objective criteria for evaluating each condition.
Conclusions
The sweat test still remains the gold standard for the diagnosis of CF. However, it has its limitations in detecting milder phenotypes of CF that may be associated with intermediate or normal sweat chloride concentrations, or rarely being falsely positive or negative due to other non-CF conditions. Interpretation of sweat test results should be done in the context of patient's clinical presentation and associated comorbidities. Additional research is needed for conditions that may affect sweat chloride concentrations.
Author Disclosure Statement
No competing financial interests exist.