
Abstract
Studies show that neurogenic inflammation is implicated in the pathogenesis of chronic cough. Neurotrophins (NTs) regulate the synthesis of neuropeptides, which cause neurogenic inflammation. There is growing evidence suggesting their involvement in airway inflammation. The role of the brain-derived neurotrophic factor (BDNF), a member of the NT family, is not clear in chronic cough. The aim of this study was to evaluate the role of BDNF in children with nonspecific isolated chronic cough and to compare the differences between patients with asthma and healthy controls. In this case–control study, we included 30 patients with chronic cough (5–15 years) as the patient group. As the control group, 28 asthma patients under control, 30 children with asthma attacks, and 30 healthy children were included. Serum BDNF levels were measured by ELISA in all groups. The median of BDNF levels was 708.12 pg/mL (155–974) in the patient group, 952.94 pg/mL (220–1,018) in the controlled asthma group, 852.09 pg/mL (355–1,036) in the uncontrolled asthma patients, and 572.65 pg/mL (213–818) in the healthy children group. There were differences in the patient group and control groups regarding the BDNF levels (for the patient group and the controlled asthma group, P = 0.0014; for the patient group and the uncontrolled asthma patients, P = 0.0009; for the patient group and healthy children group, P = 0.05). The BDNF levels of asthma patients were statistically different from healthy children (P = 0.0001). Neurogenic inflammation was implicated in the pathogenesis of chronic cough. In patients with chronic cough, high BDNF levels may support the presence of asthma.
Introduction
N
Cough is a complex neural reflex.7,8 Whatever the underlying reason is, it is known that there is airway inflammation in chronic cough.1,7,9,10 There is an increase in histamine levels of bronchoalveolar lavage fluid and levels of cys-LT, LTB4, myeloperoxidase, and tumor necrosis factor alpha in sputum samples from patients with persistent cough. 11 In the airway, activation of C-fiber receptors that play a role in cough reflex leads to the release of neuropeptides, and thus, the neurogenic inflammation, which is the reason of cough, is commenced.1,8 NTs are able to influence the neuronal phenotype of pulmonary innervation with a shift toward C-fibers. 9 It is known that NGF starts neurogenic inflammation and regulates the synthesis of neuropeptides in sensory nerves. 1 The effect of NTs on the development of airway hyperresponsiveness is well described.6,12,13
The role of BDNF, which is a member of NT family, has not yet been clarified. Studies performed on a limited number of adults have evaluated the relationship between BDNF and chronic cough; however, the results obtained were insufficient in terms of clarifying the relationship.1,7,9 The aim of this study was to evaluate the role of BDNF in children with nonspecific isolated chronic cough and to compare the differences between patients with asthma and healthy controls.
Methods and Materials
The present study was performed at the Pediatric Allergy Department of Baskent University, Adana, Turkey. Patients between 5 and 15 years old and who applied with complaints of nonspecific isolated chronic cough were included as the patient group. The control groups consisted of healthy children and asthmatic patients with uncontrolled asthma or controlled asthma. Informed consents were taken from all groups. The study was approved by the Baskent University Research Board of Medicine and Health Sciences (Project No: KA09/284).
Study inclusion criteria:
A. Patient group:
1. Dry cough lasting more than 8 weeks 2. No findings suggesting specific disease 3. Physical examination within normal limits 4. Chest radiograph and pulmonary function tests (PFT) within normal limits
B. Control group
B1. Patients with controlled asthma: Patients who are followed up by our department with diagnosis of asthma and their disease being under control in accordance with the Global Initiative for Asthma (GINA) guidelines. 14
B2. Patients with uncontrolled asthma: Patients who are followed up by our department with diagnosis of asthma and who applied to our Emergency Department with worsening of symptoms, and evaluated as uncontrolled asthma in accordance with GINA guidelines. 14
B3. Healthy children group: Children who applied to our hospital's outpatient clinics for general control and who did not have cough, asthma symptoms, history atopy, and pathological finding on systemic physical examination.
Medical history was taken from patients and the control group. Physical examination, PFT, and chest radiographs were performed. Patients with a specific reason for their cough (like cystic fibrosis, immune deficiencies, primary ciliary disorders, protracted bacterial bronchitis, recurrent pulmonary aspiration, neuromuscular or neurodevelopmental disorder, inhaled retained foreign body, tuberculosis, anatomical disorder, lung malformation, interstitial lung disease) were excluded from the study. Peripheral blood sample was taken for total eosinophil count (TEC), IgE, and BDNF levels in the beginning of the study. The eosinophil percent in the whole blood count performed by the closed system tube method (Abbott CELL-DYN 3700) was multiplied by the white cell count to calculate the number of eosinophils in a mm3. Total IgE measurement was performed by the electrochemiluminescence immunologic assay method. Serum BDNF levels were measured in serum prepared from peripheral blood by the ELISA method and MILLIPORE brand (USA) kits, the graphs were read at the TECAN Sunrise device (Catalog No: CYT306, Made in Austria) at 450 nm for evaluation, and the results were obtained in pg/mL. Our laboratory is included in the EQAS External quality control program with Lab Code No: 3584.
The patient group was followed up in our department at 18 months. During patient follow-up, atopic status was determined by the skin prick test (SPT). In the SPT, allergen solutions of Allergopharma at standard activity and concentration (positive control, negative control, D. Farinae, D. Pteronyssinus, Pine, Olive, Tree mix1, Tree mix II, Grass mix, Mediterranean herbs, Grass mix+Cereals, Alternaria, Aspergillus, Cladosporium, Cat, dog, sheepswool, budgerigar, latex, cockroach) were used. Atopy was accepted as positive in the presence of at least 3 mm indurations when compared with the negative control. 15
Statistical analyses
SPSS 16.0 software was used for statistical analyses. Coherence for normal distribution was investigated and tested for all variables and subgroups. For variables that were not in accordance with normal distribution, median values and range were given. The t-test and Mann–Whitney U test among parametric and nonparametric methods, respectively, were used for paired comparisons, and the Kruskal–Wallis method was used for multiple comparisons. The relation between parameters was determined by Spearman's rho correlation coefficient analysis. Chi-square tests were used for the comparisons of definitive groups. All tests were performed at 95% significance level, the rate of error (alpha = 0.05) was determined and tested in a two-sided manner, and when P < 0.05, the difference was accepted as statistically significant. The ErrorBar, BoxPilot, and Scatter-Dot methods were used for graphic illustrations.
Results
The patient group consisted of 30 children with isolated chronic cough (Group A), including 15 (50%) girls aged 9.45 ± 2.44 years (min–max; 5–14), and a mean coughing period of 3.63 ± 2.55 months (min–max; 2–12). Median values for TEC and IgE levels were 230/mm3 (min–max; 12–700) and 99 IU/mL (min–max; 3–528), respectively. Atopy was determined in 8 (26.7%) patients in SPT. Median BDNF level was 708.1 pg/mL (min–max; 155–974).
Age and genders of chronic cough, controlled asthma, asthma attack, and healthy children are seen in Table 1. Median level of BDNF was found as 952.9 pg/mL (220–1,018), 852.1 pg/mL (355–1,036), and 572.6 pg/mL (213–818) in Group B1, B2, and B3, respectively. Fifty-three (91.4%) of asthmatic patients had atopy in the Groups B1 and B2. Significant differences were determined at BDNF levels between the patient group and control groups. Table 2 shows the statistical comparison of the BDNF levels of patient and control groups, while the distribution of BDNF levels in these groups is given in Fig. 1.
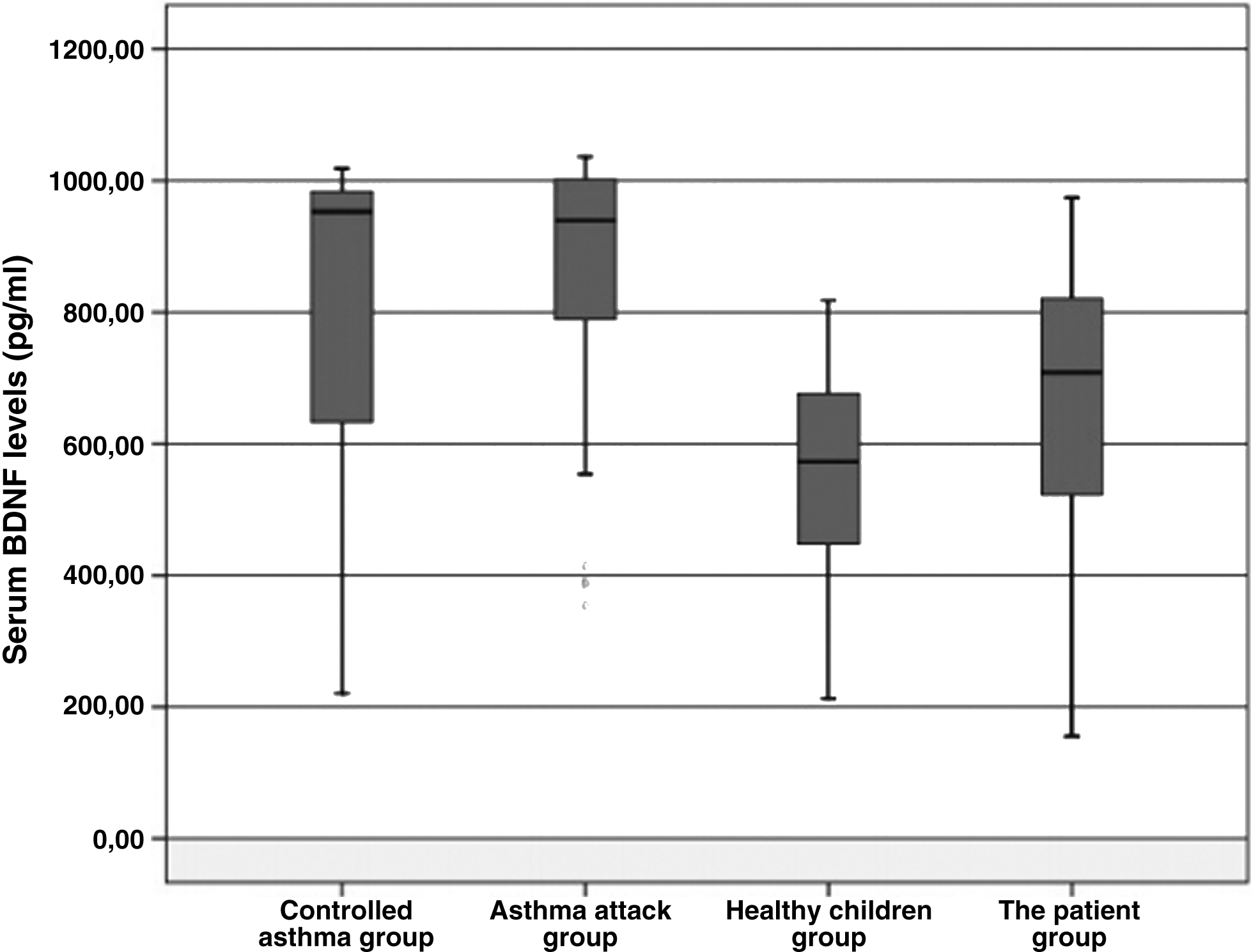
The distribution of brain-derived neurotrophic factor (BDNF) levels of chronic cough, controlled and uncontrolled asthma patients, and healthy children.
P < 0.05 is accepted to be statistically significant.
Median (min–max).
BDNF, brain-derived neurotrophic factor.
BDNF levels in atopic and nonatopic patients were 936.2 pg/mL (154.8–1,026.2) and 762.13 pg/mL (316.3–1,036), respectively (Table 3). There was a significant difference between groups (P = 0.05).
P < 0.05 is accepted to be statistically significant.
In the patient group, BDNF levels were not related with IgE, TEC, patients' age, and coughing periods. In the patient group, high TEC was positively correlated with IgE (r = 0.50, P < 0.01).
After 18 months of follow-up, 12 patients with nonspecific chronic cough were diagnosed with asthma. The BDNF level of these patients with nonspecific chronic cough diagnosed with asthma was 677.36 pg/mL.
Discussion
This study included patients with nonspecific isolated chronic cough. Physical findings, PFT, and chest X-Ray were normal, and there was only chronic dry cough complaint. Thus, we excluded patients with classic asthma from our patient group. However, we could not exclude patients with cough variant asthma (CVA). In fact, according to the literature, CVA and nonspecific isolated cough have similar definitions. 16 The primary complaint in CVA patients is dry cough, like isolated chronic cough. Bronchial provocation tests may reveal the presence of hyperreactivity in CVA. 16
Chaudhuri et al. studied serum and sputum NT levels (NGF, BDNF, NT-3) in nonsmoking patients with chronic cough and healthy adults and found no significant difference between groups. 1 BDNF has been implicated in the pathogenesis of bronchial hyperresponsiveness. 17 In literature review, there is no study evaluating the BDNF levels in children with chronic cough as far as we are concerned. In the present study, although the BDNF levels of patients with nonspecific isolated cough were different from healthy children, the difference was not statistically significant.
Koskela et al. evaluated serum and sputum NGF and BDNF levels in patients with chronic cough and healthy adults and found no significant difference between groups. However, in the chronic cough group, NGF levels differed between patients with and without asthma. Thus, they suggested that in patients with chronic cough, high NGF levels can support the presence of asthma. 7 In our study, we followed patients with nonspecific isolated cough for about 18 months and diagnosed 12 of them as asthma at the end of this period. These patients' BDNF levels were higher than healthy controls. We believe that in patients with chronic cough, high BDNF levels may support the presence of asthma. Larger studies are required to reach to this conclusion.
In a study performed on adult patients with chronic cough who did not have asthma and a healthy group, the BDNF levels in the BALF were compared and no significant difference was determined. The authors emphasized that this outcome, despite their expectations, can be related with the different methods used for measuring NT levels.1,7 In this adult study, the patients in the chronic cough group had gastroesophageal reflux disease, postnasal drip syndrome, and idiopathic cough diagnoses.1,7,9 We mostly evaluated patients with nonspecific isolated chronic cough, rather than a heterogeneous group leading to chronic cough. We believe that this difference can be related with the physiopathological differences in many different etiologies leading to chronic cough.
Recent studies have shown that NT levels in allergic asthma patients were increased in both serum and sputum samples of asthma patients.2,4,7,18–20 In our study, serum BDNF levels of asthma patients were quite high, compared with healthy children.
In the present study, when the atopy status of the 88 patients (patients with nonspecific isolated chronic cough, controlled and uncontrolled asthma) other than the healthy children was evaluated, 61 of the patients had atopy. The difference between BDNF levels of atopic and nonatopic patients was statistically significant. We planned to make the same comparison in the nonspecific isolated chronic cough group. However, as only eight patients in the chronic cough group had atopy, we could not perform the comparison. Chaudhuri et al. investigated that the NT levels of patients with chronic cough were compared between atopic and nonatopic groups and no significant difference was revealed. They concluded that NTs were related with asthma and allergy and increase in eosinophilic inflammation, but NTs do not increase in neutrophilic inflammation. 1
There are too many studies performed on the NGF levels of adult asthma patients.1,7 Virchow et al. indicated that NT production increased during the late phase response of allergic asthma and was selectively allergen dependent. 21 The effect of NTs on the development of allergic diseases is well described.
In the present study, the highest BDNF levels were observed in controlled asthma. The second highest BDNF levels were observed in asthma attacks. The reason can be the different factors that trigger the attacks seen in our asthma patients. When we evaluated our patients with asthma attacks individually, these attacks were triggered by infection in some, exposure to irritants in others, and exposure to allergens in some others. If we had included only patients with asthma triggered by allergens, the results could have been different. Further research is required on this subject.
Another study performed on the adult age group with the aim of evaluating NT levels in chronic cough reported that the cough period can affect NGF levels. The authors stated that NGF levels can change during short-term cough, and serum NGF levels were positively correlated with the cough period. 1 In nonspecific, isolated, chronic cough patient group, we could not determine any significant relationship between BDNF levels and the cough period. Furthermore, BDNF levels were not related with age, gender, TEC, and IgE levels. This study is a small-sized study, and the timing of the BDNF measurement, the difficulty of correlating BDNF levels to severity of cough, and the intrinsic variability in BDNF levels, even in normal, make it difficult to go beyond association.
Higher BDNF levels can suggest that neurogenic inflammation may play a role in chronic cough. The present study is the first study evaluating BDNF levels in children with chronic cough. BDNF levels were high in asthma and were positively related with atopy. However, detailed future studies are required for clarifying the role of NTs in the physiopathological mechanism of nonspecific isolated cough patients.
Footnotes
Acknowledgment
The study was financed by the Baskent University Research Board of Medicine and Health Sciences (Project No: KA09/284).
Author Disclosure Statement
No competing financial interests exist.