
Abstract
The incidence of food allergies in the pediatric age group is increasing. Food allergy may sometimes cause potentially life-threatening anaphylactic reactions. The purpose of this study was to determine the incidence and clinical characteristics of hazelnut allergy in schoolchildren. A questionnaire was distributed to 20,800 children, aged 6–18 years, attending schools from primary to high. In the first stage of the study, parents were requested to complete the prepared form. A skin prick test (SPT) and prick-to-prick (PTP) test were applied to all children who agreed to participate in the study. Next, a double blind placebo-controlled food challenge (DBPCFC) was applied to subjects with positive skin tests. Children with negative skin tests were administered an open food challenge (OFC). Children with positive results from the OFC took the test again to confirm the results. Of the 20,800 distributed questionnaires, 15,783 (75.9%) were returned. The SPT resulted positive in seven of these and the PTP test resulted positive in eight. DBPCFCs were applied to all 15 children whose skin tests were positive to hazelnut, and these resulted positive in 8. An open oral challenge was applied to all children with negative skin tests and with negative DBPCFC. Finally, eight children were identified as positive for hazelnut allergy, giving an incidence of IgE-mediated hazelnut allergy of 0.051% (95% confidence interval, 0.000219–0.00998). Reaction to DBPCFC was cutaneous in seven children, while skin symptoms and anaphylaxis were observed in one. The incidence of hazelnut allergy in this study was lower than results reported from previous study. Nevertheless, hazelnuts should therefore be considered in cases of food allergy, the most significant cause of allergy in childhood. While dermatological findings predominate in children with hazelnut allergy, care is necessary in respect of severe hazelnut-related reactions seen in children who develop anaphylaxis.
Introduction
T
Hazelnut allergy seen in different geographical regions and in different age groups may cause a range of clinical pictures, from mild allergic symptoms to life-threatening anaphylactic reactions.4,5 Hazelnuts are widely consumed, both alone and in processed foods such as chocolate. Hazelnut allergens can also be found as hidden allergens in some processed foods.6,7
When symptoms are seen or hazelnut allergy is suspected, the family will eliminate hazelnuts from the diet. 8 However, the possibility of hidden allergens in food still leads to stress in the child and the family because of the risk of severe reactions. To determine allergy, a detailed history must first be taken. The level of sensitivity must then be determined in suspected cases. 9
Different incidences of hazelnut allergy have been reported in several studies from across the world. Pediatric studies have reported levels of 0.1%–0.5% in Europe, 4 0.2%–0.5% in the United States, 10 and 0.09% in Russia. 11 A previous study in Turkey, which included adults and a pediatric age group, reported an incidence of 1.76%. 12
Hazelnuts are an important agricultural crop in the Eastern Black Sea region of Turkey. 13 They are widely produced and consumed, both directly and in processed form (chocolate, spreads, oil, etc.) in this region. The purpose of this study was to investigate the incidence and clinical characteristics of hazelnut allergy in children living in the city of Rize in the Eastern Black Sea region of Turkey.
Materials and Methods
This cross-sectional study recruited 20,800 randomly selected 6- to 18-year-old schoolchildren in the city of Rize in the eastern Black Sea region of Turkey during January and February 2013. Random sampling of children from state primary and secondary schools was performed in each age group and there were comparable numbers of boys and girls in all age groups.
This study was carried out in three phases. In phase 1, questionnaires, in phase 2, skin prick tested, and in phase 3, oral challenges were carried out as follows: skin prick test (SPT)-positive children were invited for an oral, double blind placebo-controlled food challenge (DBPCFC), while SPT-negative children were invited for an open challenge that was followed by a DBPCFC in case of a positive reaction. Verbal and written informed consents were obtained for SPTs and oral challenges from both parents and children.
Approval for the study was granted by the Ethics Committee of R.T.E. University.
Each child took home a standard questionnaire to be completed by the parents/caregiver and child. The questionnaire began with questions on the child's demographics (age and sex). We then asked respondents the following question: “Has your child ever had an adverse reaction to hazelnut within two hours following consumption?” If the answer was “yes,” respondents were then asked to indicate which symptoms occurred following hazelnut intake from a list, including cutaneous, nasal, ocular, bronchial, gastrointestinal, laryngeal, cardiovascular, and other symptoms. The last question requested consent for the child's participation in further analyses, including SPTs and oral challenges.
Information on familial atopy (a history of asthma, allergic rhinitis, and/or atopic dermatitis in the father, mother, or any of the siblings) and atopic diseases such as asthma, rhinitis, and atopic dermatitis of the children who were invited for SPTs was obtained at the clinic by means of an interview with the parents and by searching healthcare records of the children.
Among the children who reported an adverse reaction to hazelnut, the following were invited for SPTs: (1) those who experienced any reaction following consumption of hazelnut that previously caused a reaction, (2) those who avoided hazelnut after the reaction, and (3) those who consented to participate in further evaluation. All the children with suspected IgE-mediated hazelnut allergy who consented to participate were invited for SPTs to hazelnut and a battery of aeroallergens [Dermatophagoides pteronyssinus (Dp), Dermatophagoides farinae (Df), cat, dog, Alternaria, grass pollen mix, weed pollen mix, and tree pollen mix]. SPTs were carried out with commercially available extracts of standard hazelnut allergens (Allergopharma, Reinbek, Germany) and aeroallergens (ALK, Horsholm, Denmark). A prick-to-prick (PTP) skin test with hazelnut was also performed. For PTP test, a solution was prepared by using 1 g of hazelnut powder diluted in 4 mL of normal saline. Results were expressed as positive if the mean diameter was 3 mm or more in the presence of a negative control and a positive histamine reaction after 15 min.
All SPT-positive and/or PTP test-positive children were invited for DBPCFC following a 7-day elimination diet. Diet list also included all possible hidden sources of hazelnut.
Hazelnut for challenges was freshly prepared for each child. Challenge protocols were developed on the basis of the currently available literature.14–16 The titrated doses used for hazelnut were of the same magnitude: 0.1, 0.3, 0.6, 1.5, 2.5, 5, and 15 g, in total 25 g of the hazelnut.
In brief, children received challenge capsules of placebo or hazelnut on 2 different days in a randomized order. The clinical dietician alone performed the randomization and prepared the challenge. The recognition and perception of hazelnut and placebo to be used in the DBPCFC were masked by prepreparation in medication capsules.
DBPCFC was considered positive if a single or a combination of the clinical reactions, including cutaneous, nasal, ocular, bronchial, gastrointestinal, laryngeal, cardiovascular, and other symptoms, was noted.
Food challenge was not performed when a patient failed to provide informed consent or when a patient had a convincing history within the last year of severe anaphylaxis to hazelnut.
Negative DBPCFCs were followed by open challenges. Patients were instructed not to eat hazelnut between the negative DBPCFC and open challenges. In the open challenge, patients received a larger quantity of hazelnut (30–50 g).
Challenges were stopped at the discretion of the evaluating physician when objective signs and symptoms indicated a positive response, and medications were administered as needed. A previously described scoring system was used to determine the severity of the challenge reactions, which were scored as minimal, mild, moderate, or severe. 17 The dose interval was 15 min. Children were observed at least 2 h following the last dose of the challenge.
Statistical analyses
All analyses were performed using SPSS statistical software version 10.0 (SPSS, Inc., Chicago, IL). A descriptive analysis was used for the characterization of the study population. The prevalence of responses was compared with the Pearson χ2 test (with the Yates correction when applied) or the Fisher exact test when needed. The odds ratio (OR) and its 95% confidence interval (CI) were calculated.
Results
Of the 20,800 questionnaires distributed, 15,783 were returned (75.9%). Based on the responses, 36 children (0.23%; 20 males, 55.5%; mean age 11.4 ± 3.7; range 6–18 years) were identified as positive for possible hazelnut allergy. The demographic characteristics of these children are shown in Table 1. Further tests were refused by three children identified as positive for hazelnut allergy on the basis of the questionnaire (Fig. 1).
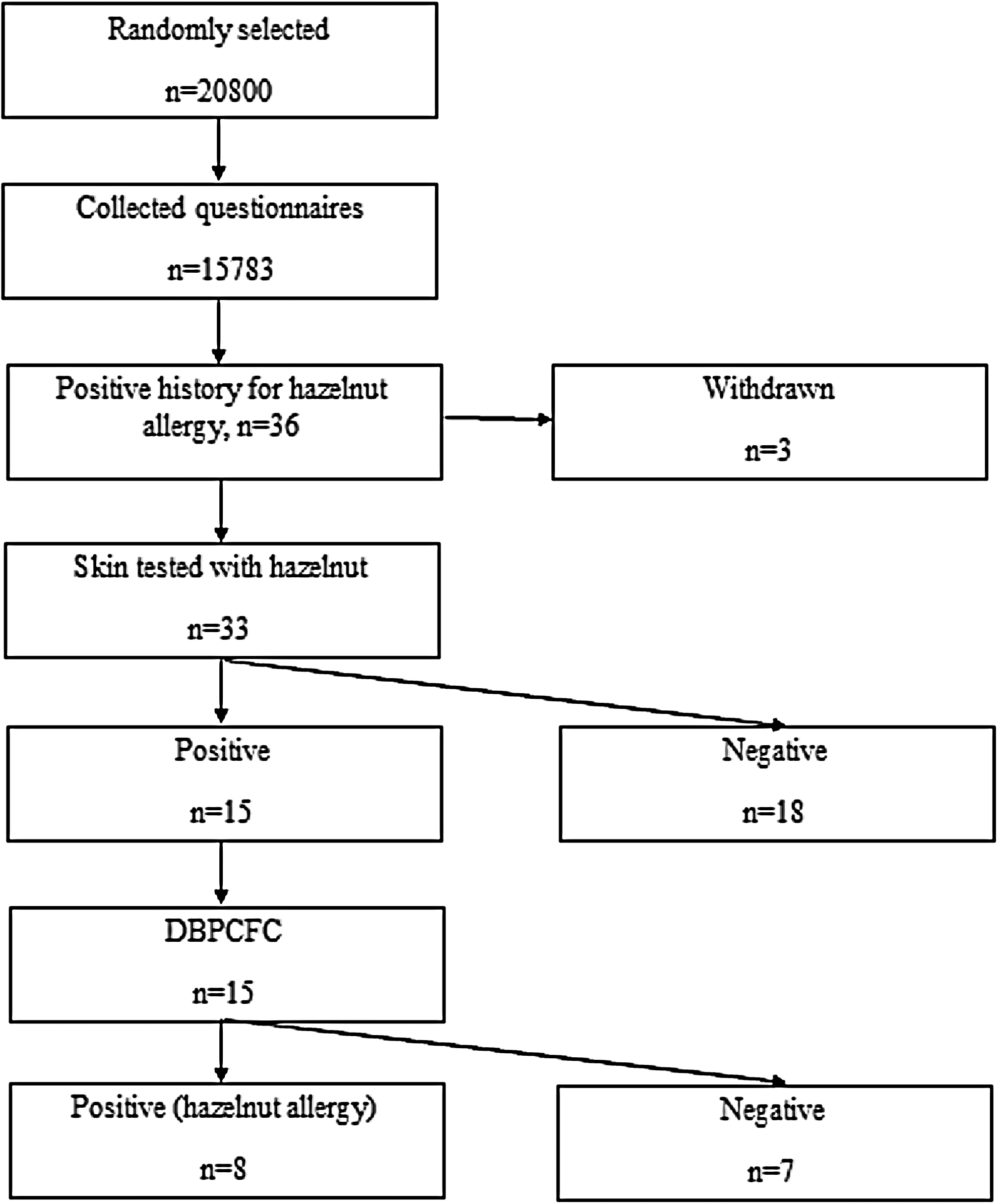
Flow chart of the study.
Of the 36 children with possible hazelnut allergy, 33 consented to further evaluation and were invited for skin tests. Further evaluation was declined by three children (Table 2).
SPT, skin prick test; PTP, prick-to-prick; DBPCFC, double blind placebo-controlled food challenge.
Of these 33 children, 30 (90.9%) reported cutaneous symptoms, 5 (15.2%) nasal, 3 (9.1%) bronchial, and 2 (6.7%) gastrointestinal symptoms. Systemic reaction was reported in seven (21.2%) children. Five of these had cutaneous and nasal symptoms, two had cutaneous and bronchial symptoms, and one had cutaneous, nasal, and bronchial symptoms.
Atopic disease was reported in 15 (45.5%) children. Allergic rhinitis was present in 12 of the 33 children (36.3%), asthma in 8 (24.2%) and atopic dermatitis in 4 (12.1%).
Familial atopic disease was reported in 17 (51.5%) children. Asthma was reported in 10 family members, allergic rhinitis in 9, atopic dermatitis in 5, and food allergy in 1.
Hazelnut skin tests were positive in 15 (45.5%) children. SPT was positive in seven of these, and PTP test was positive in eight. In five children, both SPT and PTP test were positive. In addition, SPT for house dust mites was positive in nine children (9/33, 27.3%), for tree pollens in seven (21.2%), for grasses in three (9.1%), and for weeds in two (6.1%).
DBPCFCs were applied to all 15 children whose skin tests were positive to hazelnut and resulted positive in 8 (53.3%). The characteristics of the children with positive DBPCFC findings are shown in Table 3. The reaction to DBPCFC was cutaneous in seven children (pruritus and urticaria in all and angioedema in three) and systemic (ie, anaphylaxis) in one (urticaria followed by cough, sneezing, and wheezing). An antihistamine drug was administered to all children with a cutaneous reaction and all were observed for at least 2 h following the reaction. The child with anaphylaxis was treated with a 0.01 mg/kg dose of intramuscular adrenaline and an antihistamine. Although all symptoms resolved within 30 min after administration of adrenaline, the patient was kept under observation for 8 h.
Asthma and/or allergic rhinitis and/or atopic dermatitis and/or food allergy in father and/or mother and/or siblings.
Adr, adrenaline; AH, antihistamine; DBPCFC, double blind placebo-controlled food challenge; Df, Dermatophagoides farinae; Dp, Dermatophagoides pteronyssinus.
An open oral challenge was applied to all children with a negative skin test and negative DBPCFC, and resulted negative in all.
On the basis of these results, the incidence of IgE-mediated hazelnut allergy in the study group was 0.051% (8/5,783; 95% CI 0.000219–0.00998).
Discussion
This is the first broad population-based study in Turkey to investigate the incidence of parentally reported and clinically confirmed IgE-mediated hazelnut allergy in schoolchildren aged 6–18 years.
In a study from Turkey by Orhan et al., the level of parental-reported IgE-mediated food allergy in the 6–9 age group was 5.7%, but following analysis using DBPCFC, the real allergy rate was determined as 0.08%. 18 In an adult study from Canada, questionnaires for prevalence estimates for perceived, probable, and confirmed food allergy revealed rates of 1.77%, 1.68%, and 1.03%, respectively, for peanuts and tree nuts. Following SPT and specific IgE examination, the rates were reported as 1.73%, 1.59%, and 0.69%, respectively. 6 In our study, although the number of children with parental-reported hazelnut allergy was 36 (0.23%), the overall incidence of clinically confirmed hazelnut allergy was 0.051% (95% CI 0.000219–0.00998).
Symptoms of hazelnut allergy reported in the literature include oral allergy syndrome (96%) followed by dermatological (12%), respiratory system (10%), and rhinoconjunctivitis (6%) symptoms. 14 In a study from the Tomsk region of Russia, oral allergy syndrome was the most common symptom (75%–80%), followed by gastrointestinal disorders (60%–80%) and itching skin rash (25%–50%). 11 Symptoms in the children determined positive for hazelnut allergy in our study consisted of dermatological (87.5%) and systemic (12.5%) reactions. The most frequent symptoms were dermatological and, in contrast to reports in the literature, OAS was not observed.
In a study from Turkey, Kaya et al. evaluated histories of atopy of schoolchildren aged 11–15 years with food allergy and their families. Parental-reported food allergy was first determined through telephone interviews. Accompanying allergic diseases in children were subsequently determined using SPT, PTP test and DBPCFC, revealing levels of allergic rhinitis at 36.9%, asthma at 24.1%, and atopic dermatitis at 13.6%. 3 Masthoff et al. identified atopic dermatitis in 87% of families of children (age range 5–9 years) with a history of hazelnut allergy confirmed by DBPCFC, asthma in 52%, and allergic rhinitis in 37%. 9 History of atopy was present in 45.5% of children with hazelnut allergy in our study. A history of hazelnut allergy together with allergic rhinitis was present in 36.3% of parentally reported children, with asthma in 24.2% and with atopic dermatitis in 12.1%. Our results for parentally reported comorbid food allergy and atopic disease were similar to those of Kaya et al. The results by Massthoff et al. for hazelnut allergy with atopic disease were higher than ours, while allergic rhinitis levels were similar. Recent studies have drawn attention to the combination of IgE-associated food allergy and allergic rhinitis. 19 The high rate of hazelnut allergy and allergic rhinitis combination in the current study is in agreement with the literature.
Diagnosis of food allergy requires accurate anamnesis and diagnostic testing with SPT with fresh foods and/or standardized allergen or specific IgE tests. 20 Previous studies have reported a good diagnostic value of PTP test with fresh nuts for diagnosing hazelnut allergy in adults. 14 In our study, hazelnut allergy resulted positive in four (57%) of the seven children with SPT positivity and in six (75%) of the eight children with positivity at PTP test. The gold standard in the diagnosis of food allergy is DBPCFC, although studies have also shown that SPT is also a good indicator of food allergy. 21 Comparing definitive DBPCFC results with SPT and PTP test results, these tests exhibited 57% and 75% diagnostic accuracy. DBPCFC is regarded as the gold standard, however.
Hazelnut allergy rates have been reported of 0.2% in children and 0.5% in adolescents in the United States, 8 0.1%–0.5% in the pediatric age group in Europe, 4 0.09% in the 7–10 age group in Russia, 11 and 1.76% in a study from Turkey, which included adults and a pediatric age group (13–72 years). 12 The prevalence of hazelnut allergy determined in the current study is lower than those reported previously.
The closest incidence of hazelnut allergy to that in the current study was reported in the research from the Tomsk region of Russia. 11 That study was conducted with random samples of primary schoolchildren aged 7–10 years (n = 13,100) using SPT and the serum-specific IgE measurement method to determine hazelnut allergy. The prevalence of hazelnut allergy was low, similar to the finding of the current study. Our study was performed by applying the random sample method to a larger population (20,800), and allergy was definitively determined using DBPCFC. The similarity between the results may be attributed to the studies being conducted in geographically neighboring regions using similar methodologies.
In a study of children in the city of Trabzon in the Eastern Black Sea region of Turkey, Orhan et al. investigated parental-reported IgE-mediated food allergy in the 6–9 age group. They determined a parental-reported level of 3.1%, compared to 2.2% at SPT (most commonly to beef, followed by cocoa and cow's milk). According to the DBPCFC results, none of the children reacted to hazelnuts, which are widely consumed in the Eastern Black Sea region. 18 It is noteworthy that although the region where the study was performed and the population were similar to ours, while different levels of food allergy were identified, no hazelnut allergy was determined. Careful anamnesis focusing on hazelnut allergy, determined in children at the low level of 0.051% in our region, and tests must be performed with greater sensitivity.
In conclusion, the incidence of hazelnut allergy in this study was lower than results reported from Europe, Russia, and the United States. Although dermatological findings predominate in children with hazelnut allergy, care is necessary in respect of severe hazelnut-related reactions seen in children who develop anaphylaxis. Hazelnuts should therefore be considered in cases of food allergy, the most significant cause of allergy in childhood. In addition, a noticeable difference was determined between the proven incidence of hazelnut allergy in this study and the results of previous research.
Footnotes
Acknowledgments
SD presented the hypothesis and designed the study. MA was responsible for writing the report. TK was responsible for the analysis of the data. The authors also thank Hikmet ORHAN for statistical analysis and Carl Austin Nino Rossini for English language editing.
Author Disclosure Statement
No competing financial interests exist.