
Abstract
This pilot survey was designed to evaluate the characteristics of anaphylactic events and epinephrine autoinjector (EAI) use in children in U.S. schools. A cross-sectional, web-based, pilot survey of schools participating in the EPIPEN4SCHOOLS® program (Mylan Specialty L.P., Canonsburg, PA) assessed characteristics of anaphylactic events and EAI use during the 2013–2014 academic year. Respondents reported 757 anaphylactic events experienced by students; student grade level was noted for 724 events. Of these events, 32.3% (234/724) were experienced by students in grade school, 18.6% (135/724) by students in middle school, and 49.0% (355/724) by students in high school. Frequency of food-related triggers was consistently high across grade levels. However, many events experienced by students in high school (22.3%, 79/355), middle school (15.0%, 20/135), and grade school (14.1%, 33/234) had an unknown trigger. In 36.0% of schools (2008/5579), only the school nurse and select staff received training to recognize anaphylaxis; most staff or all staff received training in 28.9% (1610/5579) and 30.9% (1722/5579) of schools, respectively. In a majority of schools (54.2%, 3003/5544), only the school nurse and select staff were permitted to administer epinephrine, whereas most staff or all staff were permitted to administer epinephrine in 15.8% (876/5544) and 21.9% (1212/5544) of schools, respectively. Risk of anaphylaxis may be particularly high during adolescence, and some students encounter staff members who are untrained in anaphylaxis recognition or management, or both. These findings support the need for continued anaphylaxis training for the protection of all students, staff, and visitors.
Introduction
A
Despite the increasing risk of severe allergic reactions and anaphylaxis in U.S. schools, preparedness for addressing such emergencies among school staff may still be lacking. A study on severe allergic reactions in schools revealed that school staff were unaware of life-threatening allergies in nearly 1 in 4 cases, resulting in a failure to have individualized action plans and physician orders for epinephrine for the affected students. 7 Results from a survey of school nurses showed that school nurses scored notably lower on objective knowledge tests concerning anaphylaxis, compared with tests concerning diabetes and asthma, 2 other disease states commonly associated with emergencies in the school setting. 8 Specifically, school nurses lacked awareness regarding appropriate administration of a second dose of epinephrine to manage an anaphylactic reaction, which may be important for treating prolonged or biphasic reactions. 8 Together, these data emphasize the need for school staff to be prepared to assess and treat students who may experience anaphylaxis and severe allergic reactions at school.
In 2012, the EPIPEN4SCHOOLS® program (Mylan Specialty L.P., Canonsburg, PA) began providing EpiPen® Auto-Injector (epinephrine injection) 2-packs and/or EpiPen Jr Auto-Injector 2-packs (Mylan Specialty L.P.) and training materials to qualifying public and private U.S. schools, inclusive of pre-kindergarten (pre-K), kindergarten, elementary, middle, and high schools. A major goal of the program is to improve access to EAIs for children and adults in school settings. As previously reported, 32,387 schools participating in the EPIPEN4SCHOOLS program were asked to complete a survey on the use of epinephrine and treatment of anaphylaxis during the 2013–2014 school year. 9 Of the 6019 responding schools, ∼1 in 10 reported an anaphylactic event. Herein, we assessed the characteristics of students who experienced an anaphylactic event as well as the school staff who were trained in the management and recognition of anaphylaxis.
Methods and Materials
Study design and sample preparation
An exploratory, web-based, cross-sectional pilot survey of U.S. schools participating in the EPIPEN4SCHOOLS program during the 2013–2014 academic year was conducted. The survey consisted of a brief online questionnaire that was completed by the person best suited to respond regarding all occurrences of severe allergic reactions and treatment(s) administered at each school. The effective sample for the survey consisted of 32,387 public and private U.S. schools for which there was either a physical or e-mail address at the school or contact level. BioRidge Pharma maintains the database of schools registered with the EPIPEN4SCHOOLS program and provided logistical mailing services during the administration of the survey. The protocol for communicating with potential respondents varied on the basis of the number of schools for which the listed contact was responsible. Reminders to complete the survey were sent weekly, beginning 1 week after the initial request, through e-mail to all schools that had not completed the survey.
The study was submitted to the RTI Institutional Review Board (IRB) for approval, which determined that the research activity did not constitute research involving human subjects as defined by the U.S. Code of Federal Regulations (45 CFR 46.102). The approval of these activities by the RTI IRB was not necessary; therefore, an exemption was granted. The study design and sample preparation have been previously described in greater detail. 9
Survey development and administration
This was a self-administered web-based survey consisting of 16 questions, several of which were asked about each specific anaphylactic event (Table 1). The time frame for completion was between May 21 and July 9, 2014. A toll-free telephone number and e-mail address were provided in case technical assistance was needed. In an effort to respond to calls in a timely manner, staff members were located at offices in 3 time zones. When callers left voicemails, project staff would respond to calls at the end of each day. A weekly reminder e-mail message was sent to schools that had not yet completed the survey, through July 1, 2014. Development and administration of the survey were previously described in greater detail. 9
EAI, epinephrine autoinjector.
Data analysis
Descriptive analyses were performed for the following characteristics of reported anaphylactic events: grade of the student at the time of the anaphylactic event; presence of known allergies; trigger that caused the anaphylactic event; medication used to treat the anaphylactic event (eg, epinephrine, antihistamines); source of the EAI used for treatment (ie, school stock, individual); and transportation to a hospital after the anaphylactic event. Additional descriptive analyses of characteristics intended to contextualize participating schools included school staff who were trained to recognize an anaphylactic event and school staff who were allowed to administer an EAI. Relative frequency was calculated by dividing the total number for each response category of the variable of interest across all schools by the combined number of responses (including those that the respondent marked as “unknown”) across all schools. Missing responses were excluded from the analysis.
Results
Anaphylactic events among the student population
Survey participants indicated the grade for 95.6% of anaphylactic events experienced by students (724/757). Of these 724 anaphylactic events, 32.3% (n = 234) were experienced by students in grade school (pre-K through fifth grade), 18.6% (n = 135) were experienced by students in middle school (sixth through eighth grade), and 49.0% (n = 355) were experienced by students in high school (9th through 12th grade) (Fig. 1A). Most anaphylactic events were experienced by students in 10th grade (15.6%, 113/724), followed by students in 9th (13.4%, 97/724) and 11th grade (11.6%, 84/724; Fig. 1B). Students in second and third grade experienced the fewest anaphylactic events (4.7% each, 34/724; Fig. 1B). Of the students who experienced an anaphylactic event and for whom the grade was known to the respondent, 72.1% (522/724) had a known allergy and 20.7% (150/724) had no known allergies. In 7.0% of the events (51/724), the respondent did not know if the student had a preexisting allergy. The students who experienced an anaphylactic event and had known allergies were mostly in 1st (8.6%, 46/538), 9th (10.8%, 58/538), 10th (15.8%, 85/538), 11th (12.5%, 67/538), and 12th grade (8.6%, 46/538; Fig. 2). Most students who experienced an anaphylactic event and had no known allergies or whose allergy status was unknown to the respondent were in 8th (10.0%, 20/201), 9th (19.4%, 39/201), 10th (13.9%, 28/201), and 11th grade (8.5%, 17/201).

Distribution of anaphylactic events reported by
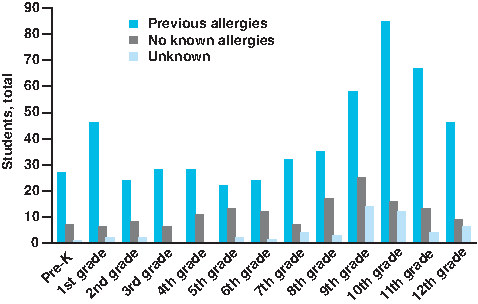
Number of previously known allergies reported by student grade level. pre-K, pre-kindergarten. Color images available online at www.liebertpub.com/ped
Anaphylactic triggers
Triggers of anaphylactic reactions were similar among all grade levels (Fig. 3). Of the 721 events with data on the trigger, most events were caused by food (66.3%, n = 478), followed by unknown triggers (18.3%, n = 132), insect bites or stings (9.3%, n = 67), and environmental or medical triggers (6.1%, n = 44). The proportions of anaphylactic events triggered by food and insect bites/stings decreased among students in 9th through 12th grade compared with students in pre-K through eighth grade. Conversely, the proportions of environmental and unknown triggers increased among students in 9th through 12th grade compared with students in pre-K through eighth grade. Among high school students, ∼1-quarter of anaphylactic events (22.3%, 79/354) was reported to be of unknown origin. Of these, the majority occurred among students in 9th and 10th grade. Percentages of anaphylactic events of unknown origin were 14.1% (33/234) and 15.0% (20/133) for students in grade school and middle school, respectively.

Types of triggers of anaphylactic events among students by grade level. Color images available online at www.liebertpub.com/ped
Treatment of anaphylactic events
Of the 719 anaphylactic events that were experienced by students and for which data on EAI usage and grade level were reported, only 568 (79.0%) received treatment with an EAI. Data on the use of EAIs were reported as unknown for 1 student. Of the 568 students who were treated with an EAI on school property, 269 were treated with an EpiPen Auto-Injector from the school's stock; 268 were treated with a personal EpiPen Auto-Injector; 22 were treated with an EAI other than an EpiPen Auto-Injector; and 9 were treated with an EAI of unknown type or source. Those who most frequently received treatment with an EAI were students in 10th grade (88.5%, 100/113), followed by students in 12th (83.6%, 51/61) and 9th grade (80.2%, 77/96) (Fig. 4); students in pre-K were treated least frequently with an EAI (58.3%, 21/36). Information on the use of a second EAI was reported for 544 anaphylactic events; of these, a second EAI was used for treatment in 39 events (7.2%, 39/544). For 27 of the anaphylactic events, the respondent did not know if a second EAI was used. Of the events treated with EAIs, the use of a second EAI was most frequent in 11th grade (15.4%, 10/65), pre-K (14.3%, 3/21), and 10th grade (13.0%, 13/100), whereas the frequency in other grade levels ranged from 0% (second, third, and seventh grades) to 10% (first grade).
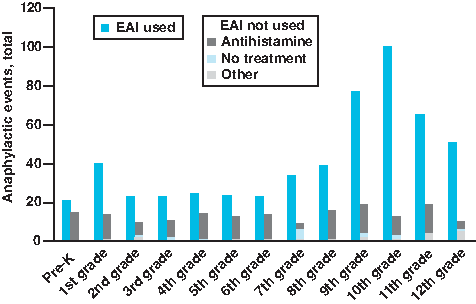
Use of EAIs or alternative therapies for treatment of anaphylactic events by student grade level. EAI, epinephrine autoinjector; pre-K, pre-kindergarten. Color images available online at www.liebertpub.com/ped
A total of 178 anaphylactic events (24.6%) were reported as not being treated with an EAI. Of these, 80.3% (143/178) received antihistamines, 10.7% (19/178) received some other treatment, and 7.9% (14/178) received no treatment. The frequency of antihistamine use was generally higher in grade schools (29.5%, 69/234) compared with middle schools (23.0%, 31/135) and high schools (12.1%, 43/355). The observed frequencies of antihistamine use ranged from 6.6% among students in 12th grade (4/61) to 41.7% among pre-K students (15/36). Treatment received was reported as unknown for 2 of the anaphylactic events.
Of the 723 anaphylactic events with data on hospital transportation and student grade level, 580 students (80.2%) were transported to a hospital after experiencing an anaphylactic event. The majority of students (75.3%, 437/580) were transported by ambulance, whereas almost one-quarter (24.7%, 143/580) was transported by some other means (eg, parent, guardian). In 1.0% of the events (6/580), the respondent did not know if the student had been taken to the hospital after experiencing an anaphylactic event. Students in middle school were transported to the hospital less frequently (71.9%, 97/135) compared with students in either grade school (80.8%, 189/234) or high school (82.8%, 294/355).
Training and administration of medication by school staff
A total of 5579 responding schools with available grade-level information provided information on staff members who were trained to recognize anaphylaxis. Among grade schools (pre-K through fifth grade), 36.7% (734/1999) trained the school nurse and select staff, 32.2% (644/1999) trained all staff, 28.1% (562/1999) trained most staff, and 1.4% (28/1999) trained only the school nurse (Fig. 5A). These proportions were similar among middle schools (sixth through eighth grade) and high schools (9th through 12th grade); however, some variation was observed among schools with alternative grade-level combinations (Fig. 5A). Among schools with pre-K through 12th grade, only 22.9% (62/271) trained the school nurse and select staff; by contrast, the proportion of schools with 6th through 12th grade that trained the school nurse and select staff was nearly 2-fold higher (43.0%, 139/323). Overall, only 1.1% of schools (59/5579) listed select staff other than the school nurse (eg, coaches, athletic trainers, first responders, office staff) as staff members who were trained to recognize anaphylaxis. A minority of schools (0.1%, 7/5579) trained no staff, and 1.1% of schools (61/5579) responded “I'm not sure.”
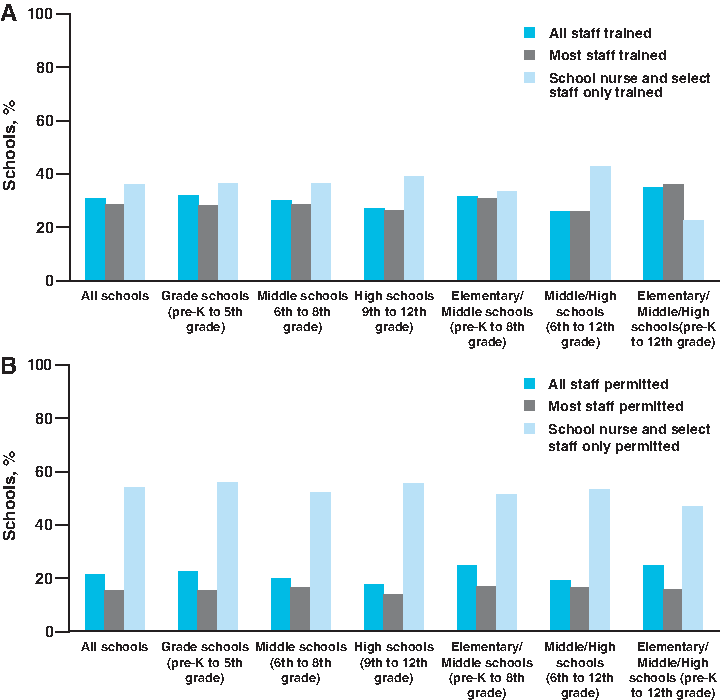
School staff
Overall, more school staff members were trained to identify signs and symptoms of anaphylaxis than were permitted to administer epinephrine. A total of 5544 responding schools with available grade-level information provided information on staff members who were permitted to administer epinephrine (Fig. 5B). Proportions of grade schools (pre-K through fifth grade), middle schools (sixth through eighth grade), and high schools (9th through 12th grade) that permitted only the school nurse and select staff to administer epinephrine were 56.4% (1117/1980), 52.7% (337/639), and 56.0% (554/989), respectively (Fig. 5B). Proportions of schools that permitted most staff (grade schools: 15.9%, 314/1980; middle schools: 16.6%, 106/639; high schools: 13.5%, 134/989) or all staff (grade schools: 22.5%, 445/1980; middle schools: 20.0%, 128/639; high schools: 17.8%, 176/989) to administer epinephrine were considerably lower (Fig. 5B). Overall, few schools (1.7%, 94/5544) listed other select staff (eg, health aides and wellness staff) as staff who were permitted to administer epinephrine, and only 0.5% (30/5544) responded “I'm not sure.”
Discussion
Data from this pilot survey support published reports indicating that anaphylactic and severe allergic reactions, especially those triggered by food, are not uncommon among students in U.S. schools.5–7,10 EPIPEN4SCHOOLS survey respondents reported the occurrence of anaphylactic events across all school grade levels, but as other studies have previously indicated, adolescence may be a particularly high-risk developmental stage for anaphylaxis.3,6,11 In our study population, almost 50% of anaphylactic events experienced by students were reported for high school students. Similar findings have been observed in Massachusetts, where the majority of anaphylactic events were observed in teenagers. 10 This finding is also consistent with research suggesting that the odds of a severe allergic reaction are significantly higher for adolescents compared with younger age groups. 3 The survey also revealed that ∼20% of events across all age groups occurred in the absence of an established allergic trigger; the incidence of such events was considerably higher for students in high school compared with other age groups, further highlighting the increased risks associated with adolescence. This pattern has important implications because adolescents are typically not supervised as closely as younger children and may require innovative policies (eg, student anaphylaxis training) to maintain optimal preparedness in upper grade levels.
Survey findings also suggest that deficits may exist in school staff training programs to recognize and properly treat anaphylaxis. Responding schools across all grade levels most frequently provided training for only the school nurse and select staff to recognize symptoms of anaphylaxis; less than one-third of grade, middle, and high schools provided training for all staff members on the recognition of anaphylaxis. An important implication of this finding is that many students, regardless of grade level, will routinely encounter staff members who are not trained in any aspect of anaphylaxis recognition. There was also a notable disparity between the proportions of schools that trained all staff to recognize anaphylaxis and those that permitted all staff to administer an EAI for treatment of anaphylaxis. Overall, less than one-quarter of schools permitted all staff to administer an EAI; this proportion was lowest among high schools at 17.8%. Thus, it may not be uncommon for a student to encounter a staff member who is trained to recognize symptoms of anaphylaxis but not permitted to treat the reaction with an EAI. In a study of anaphylactic events in the Chicago Public School district, it was found that 23.7% of EAIs were administered by someone other than the school nurse, 12 further demonstrating the importance of widespread training among school staff.
A final key finding was that many anaphylactic events were not treated with an EAI, the only approved first-line therapy for such life-threatening reactions. Although responding schools demonstrated some awareness of the severity of anaphylaxis and its proper treatment by participating in the EPIPEN4SCHOOLS program, more than 20% of students across all grade levels who experienced an anaphylactic reaction were still not treated with an EAI. Incidence of antihistamine use instead of EAIs was highest among grade school students and lowest among high school students. Higher levels of independence and greater experience with recognizing and managing severe allergic reactions may be factors in the increased usage of EAIs among high school students. It is a significant source of concern, however, that the usage of antihistamines instead of EAIs reached 29% in grade schools overall and exceeded 40% among students in pre-K, groups of students who are highly dependent upon school staff for the management of medical emergencies. Together, these data emphasize the importance of anaphylaxis preparedness training for school staff supervising students of all grade levels, particularly with respect to recognition of the signs and symptoms of anaphylaxis and the use of epinephrine as the optimal first-line therapy for life-threatening severe reactions.
Study limitations
Survey methodology was a key limitation of this study, given that surveys may be inherently subject to various measurement errors, such as systematic and random variance that stems from respondents (eg, failure to carefully read a question) and variance that stems from questionnaire design (eg, ambiguously worded questions and answers). For example, one of the potential response options for the question of trigger type was “unknown”; in this survey, it was not possible to differentiate between triggers that were unknown only to the respondent and those that were unknown to both the respondent and the student. Surveys also have the potential for response bias when general response rates are low or when response rates from a specific subpopulation make up a disproportionately large part of the sample. In the case of this exploratory survey, the response rate was 19%. The surveys were distributed to schools late in the school year with a 6-week window of time for completion, which may have contributed to the low response rate. Finally, the data reported by study participants were limited by the level of detailed information recorded for the cases of anaphylaxis and subject to respondent recollection of the events. A study is currently being conducted with a larger pool of participants in the EPIPEN4SCHOOLS program and an extended study period to address some of the limitations discussed above.
Institution at Which the Work Was Performed
BioRidge Pharma maintains the database of registered schools that participate in the EPIPEN4SCHOOLS program; during the administration of this pilot survey, BioRidge Pharma worked with RTI to provide logistical mailing services for letters sent to participating schools. Surveys were completed online by participants and submitted to RTI.
Footnotes
Acknowledgments
This study was supported by Mylan Specialty L.P. BioRidge Pharma maintains the database of registered schools that participate in the EPIPEN4SCHOOLS program; during the administration of this pilot survey, BioRidge Pharma worked with RTI to provide logistical mailing services for letters sent to participating schools. Editorial assistance was provided under the direction of the authors by Michael Hast and Jennifer Rossi, MedThink SciCom, with support from Mylan Specialty L.P. Funding source: This study was supported by Mylan Specialty L.P.
Author Disclosure Statement
M.V.W. has served as a consultant for Mylan Specialty L.P. and Merck; has served as a board member for the Allergy and Asthma Network Mothers of Asthmatics; and has received grants, fees, or support from Mylan Specialty L.P., Merck, CSL Behring, AstraZeneca, Shire, Salix, Novartis, Teva, GlaxoSmithKline, Dyax, and Optinose. M.E.B. has served as a consultant for Mylan Specialty L.P. M.J.W. is a paid employee of Mylan Specialty L.P. and may hold stock within the company. S.S., D.G., S.H., K.H., P.S., and K.M. have no conflicts of interest to declare.