
Abstract
Picture-based Asthma Action Plans show promise for overcoming parental literacy barriers and improving child asthma outcomes, but it is uncertain how parents respond to pictures of specific medications, which may be particularly important for improving disease self-management. Thus, we assessed parent attitudes toward an asthma-related picture-based medication plan (PBMP) in an urban academic pediatric clinic and examined attitudes by literacy level. Surveys were administered to a convenience sample of parents of children presenting to an urban pediatric pulmonary clinic for asthma consultation between March and August 2011. The Rapid Estimate of Adult Literacy in Medicine-Short Form (REALM-SF) was administered to parents. Parents indicated their level of agreement with 9 statements on the potential usefulness of the PBMP: (1) before being shown a PBMP; and (2) after seeing the doctor. McNemar's tests showed that the proportion of high-literate parents (≥9th grade reading level) who endorsed the potential benefits of the PBMP after the clinical encounter was significantly higher than before the clinical encounter. A high proportion of low-literate parents (<9th grade reading level) consistently endorsed the PBMP before and after the clinical encounter. Among a diverse sample seen in an urban asthma clinic, parents of all literacy levels endorse PBMPs as useful, especially after using them in clinical encounters.
Introduction
A
Recently developed picture-based AAPs offer a promising solution to overcoming parental literacy barriers and improving children's asthma outcomes.10–12 Several studies in the health education literature have documented that patients pay more attention, demonstrate better comprehension, have better recall, and are more likely to carry out (ie, adhere to) depicted health behaviors when verbal health information is presented along with pictures compared to text/speech alone. 13 Moreover, these pictorial effects appear to be greater for patients with lower health literacy.13–15 A limitation of the current research on picture-based AAPs is failure to include pictures of specific medications (ie, picture-based medication plan [PBMP]), which may be particularly important for improving disease self-management.
A consistently noted feature of effective pictures in health communication is cultural relevance, 13 highlighting the importance of field testing pictorial health information within the target population. 16 Thus, in the current study, our specific aim was to assess parent attitudes toward an asthma-related PBMP in an urban outpatient academic pediatric clinic that serves an innercity population disproportionately affected by pediatric asthma. Moreover, we examined the extent to which attitudes vary by health literacy level, to determine whether the potential PBMPs had for overcoming literacy barriers can be realized.
Materials and Methods
Enrollment procedures
The Johns Hopkins Children's Center provides outpatient asthma care to children in the Baltimore, Maryland metropolitan area. For this study, a convenience sample of parents of patients with asthma was recruited from the outpatient clinic between March and August of 2011. Patients presenting for an asthma consultation by pediatric pulmonologists were invited to provide information for a registry that was established to characterize asthma morbidity of patients in the pediatric pulmonary clinic and to collect clinical data to validate an asthma questionnaire.17,18 A trained research assistant (RA) explained the study, screened interested parents/patients for eligibility, and obtained informed consent from caregivers and assent from children older than 8 years of age. Interested parents were eligible for the current study if: (1) their child had doctor-diagnosed asthma, and (2) their child was 21 years of age or less. The Johns Hopkins University Institutional Review Board approved this study.
Picture-based medication plan
Following national asthma guidelines, 19 the senior author (S.O.O.) constructed a PBMP at a 4th grade reading level (Fig. 1). Pictures of controller and rescue medications are included in the PBMP. The physician circles the medications the patient is to take, then fills in simple written directions. A RA showed the PBMP to parents before the family saw their doctor. During the clinical encounter, the doctor completed the PBMP and explained it to the family.
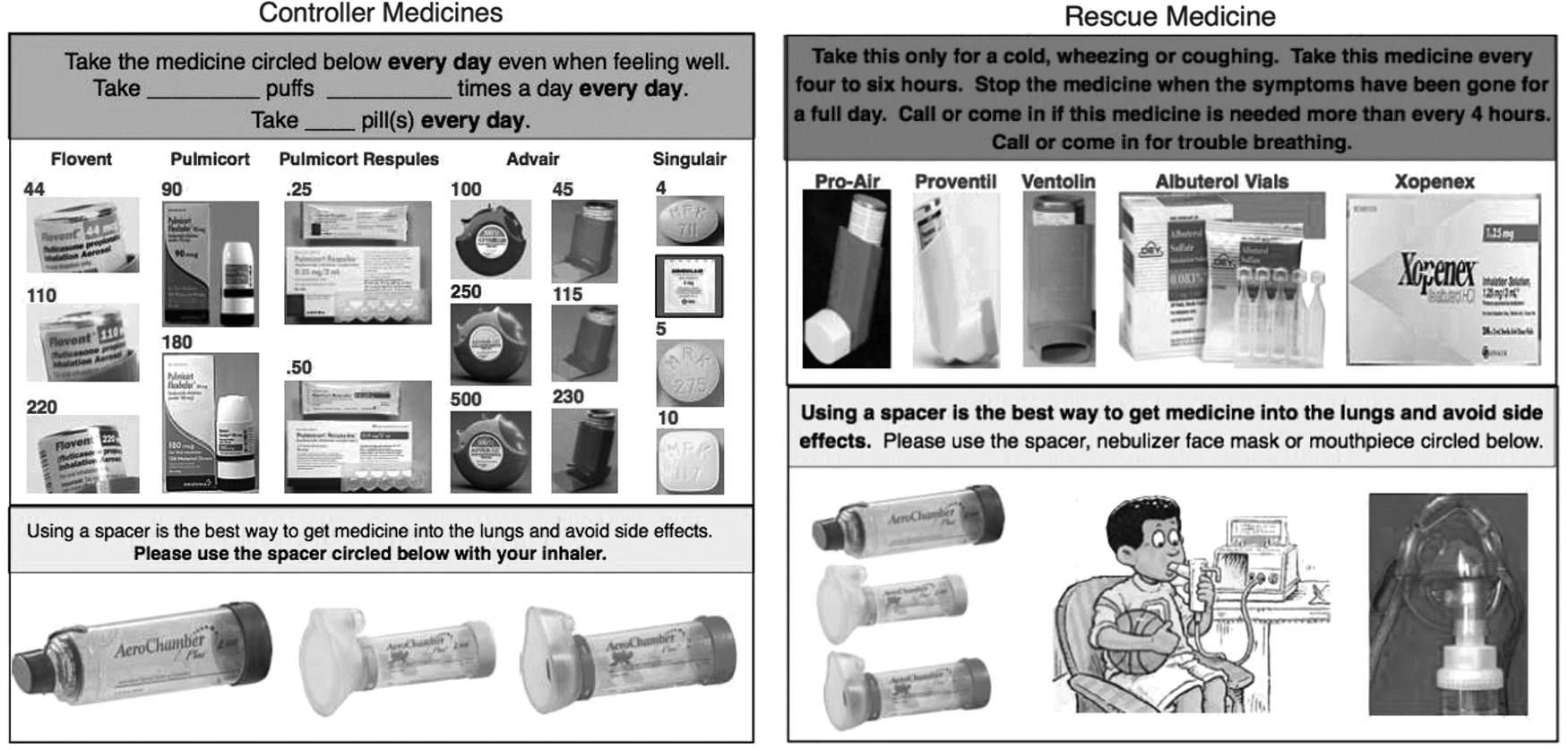
Picture-based medication plan.
Data collection
While waiting for the doctor, the RA surveyed the consenting parent. Parents reported basic demographics (ie, child age, gender, and ethnicity). They also completed the 12-item Pediatric Asthma Control & Communication Instrument (PACCI) to determine children's current level of asthma control. 17 The PACCI assesses frequency of daytime symptoms, short-acting beta2-agonist use, attacks, activity limitation, and nocturnal symptoms. The PACCI can be scored using: (1) a continuous score ranging from 0 (best control) to 19 (worst control); or (2) categories (well controlled versus not well controlled) based on national asthma guidelines. 19 Parental health literacy was measured using the Rapid Estimate of Adult Literacy in Medicine—Short Form (REALM-SF): parents read aloud 7 medical words: behavior, exercise, menopause, rectal, antibiotics, anemia, and jaundice. Reading grade level is determined based on the number of correctly pronounced words: 0–6 = less than 9th grade; 7 = 9th grade or higher. 20 Finally, parents rated the potential usefulness of the PBMP by indicating their agreement (5-point scale) with 9 statements (eg, “I would feel more confident in my ability to treat my child's asthma if I could review pictures of the asthma medicines with my child's doctor”; “I would like my child's doctor to explain how to use asthma medications using pictures”). They provided these ratings at 2 time points: before being shown a PBMP, but after being given a brief description of one by the RA and after the clinical encounter with their doctor.
Statistical analysis
First, groups were split based on parental health literacy levels according to a conventional cut point21,22: ≥9th grade literacy level (n = 64) versus <9th grade literacy level (n = 15). Two sample t-tests and chi-square tests were conducted comparing these groups on demographics and asthma control (percentage with well-controlled asthma). Next, McNemar's tests were conducted comparing the proportion of parents who responded as “agree” or “strongly agree” to each evaluative statement after the clinical counter versus before; these were conducted separately for each health literacy group. Significance level was set at P < 0.05.
Results
The full sample (N = 79) was mostly nonwhite with well-controlled asthma, and almost 20% of parents had less than a 9th grade literacy level (Table 1). The literacy groups did not significantly differ in terms of child age, gender, or asthma control; however, the higher literacy group had a higher proportion of white children compared to the lower literacy group.
Two samples t-test.
Chi-square test.
Before interacting with their providers, most of the lower literacy parents endorsed the PBMP (Table 2). Generally, there was no significant change in the proportion that endorsed the PBMP after interacting with the provider, although lower literacy parents that endorsed “Having pictures of my child's asthma medicines would make me more confident talking to my child's doctor about my child's asthma” and “I would feel more confident in my ability to treat my child's asthma if I could review pictures of the asthma medicines with my child's doctor” increased by more than 20 percentage points.
McNemar's test of repeated proportions.
PBMP, picture-based medication plan.
Comparatively, fewer parents in the higher literacy group (n = 64) endorsed the PBMP before discussing it with their child's provider (Table 3). However, we observed a significant increased endorsement of PBMPs on 4 of the 9 evaluative statements after clinical encounters.
McNemar's test of repeated proportions.
In both literacy groups, post use of the PBMP, we observed a decrease in the level of endorsement for 2 statements: feeling “more educated about my child's asthma” and “more comfortable treating my child's asthma” (P > 0.05 for both changes). In the low-literacy group only, there were 2 additional statements that decreased in level of endorsement: (1) the PBMP “would make it easier to show my child's doctor the medications my child takes for asthma” (87% versus 80%); (2) “I would feel more comfortable describing how often my child used their asthma medications” (64% versus 57%) (P > 0.05 for both changes).
Discussion and Conclusion
In this sample of parents of children with asthma seeking care from an urban outpatient clinic, we found that parents with lower literacy reported positive attitudes toward the PBMP at the outset, which did not significantly change after actual use of PBMPs with providers. This may be because parents with lower health literacy are aware of their need for pictorial instructions and, thus, endorsed the PBMPs before being given one tailored to their child's treatment. This pre-encounter self-awareness may also explain why we did not observe significant changes in endorsement of the PBMP after clinical encounters.
Parents with higher literacy showed a significant increase in their endorsement of PBMPs after actually using it with their child's physician. It may be that these more literate parents were appreciative of the pictorial instructions once a personalized PBMP was presented to them.
Notably, there was some decreased endorsement of the PBMP in both literacy groups (eg, “I would feel more comfortable treating my child's asthma if I could review the asthma medicines with my child's doctor). It may be that certain parental expectations exceeded the scope of the PBMP (eg, asthma education regarding pathophysiology and medication side effects; improving adherence recall; and inhaler technique). Moreover, modifications to the PBMP based on these decreased endorsements may improve its acceptability (eg, adding depictions of how to use medication devices). Some next steps in this line of research include: (1) repeating the study in a larger sample to explore potential differences between patients of specific literacy levels to determine if present results are replicable; and (2) measuring self-management behaviors (eg, medication adherence) in relation to changes in attitudes toward the PBMP.
Conclusion
Among an urban racially diverse sample seeking care from an urban outpatient asthma clinic, parents of low and high literacy levels endorse specific benefits of a picture-based medication plan (PBMP) for asthma care, especially after using them in clinical encounters. The fact that most of the lower literacy parents endorsed a PBMP suggests that this may be a means of improving parent understanding, confidence, and communication with physicians during clinical encounters.
Footnotes
Acknowledgment
This study was conducted at the Johns Hopkins University. Funding for this research was provided to Dr. Okelo through NHLBI HL089410.
Author Disclosure Statement
No competing financial interests exist.