
Abstract
Emergency department (ED) visits for asthma exacerbation have not become less frequent, essentially because the self-management of mild-to-moderate asthma exacerbations by children and their families remains sub-optimal. The objective of our study was to assess the proportion of visits to EDs for asthma exacerbation that were potentially avoidable and their risk factors [such as no Written Asthma Action Plan (WAAP)]. We conducted an 8-month multicenter study in 6 French pediatric EDs. Parents, nurses, and physicians filled out a questionnaire, recording information on the history of asthma and education (peak flow, WAAP), the self-management of the present exacerbation, the reasons for coming to the ED, the severity of the exacerbation, and the clinical outcome. An ED visit was deemed as potentially avoidable when a child who had not received adequate prehospital treatment left the ED after a maximum of 3 nebulizations with a bronchodilator with no relapse within 48 h. We included 107 children [mean (standard deviation) age 9.8 (2.4) years, 40% were girls]. At arrival, 76 children [71%, 95% confidence interval (CI): 62–80] had not received adequate treatment for the current exacerbation. Forty-one children (38%, 95% CI: 29–48) had an avoidable ED visit. Feelings of fear/anxiety were the only independent risk factor for avoidable visits, whereas the existence of a WAAP at home did not independently influence avoidable visits. Inadequate prehospital treatment and avoidable visits are frequent in children with known asthma visiting EDs for an asthma exacerbation. Strategies to reduce avoidable visits should seek to improve the WAAP, to develop and validate new electronic tools for self-managed interventions, and to provide reassurance.
Introduction
D
In a large number of cases, emergency department (ED) visits are not related to severe exacerbations requiring inpatient treatment but are the result of inadequate prehospital management of mild-to-moderate exacerbations.7,8 Causes for poor exacerbation management are multiple, ranging from inadequate therapeutic education to lack of medication available at home. As a result, 3 quarters of children with asthma visiting the ED do not need to be hospitalized9,10; however, they still seek medical care.
The Written Asthma Action Plan (WAAP) is a tool developed and used in therapeutic education to help patients formalize exacerbation management with respect to the recognition of early signs, knowledge of the names and doses of emergency medications, and identification of signs of severity requiring urgent medical attention.1,2 However, the distribution of WAAP among asthmatic patients is low, and even though it is more frequent in children than in adults visiting EDs (34% versus 26%), 11 it remains insufficient in hospitalized children (51% of the cases). 12 Moreover, it has recently been demonstrated that using a WAAP form to provide asthma management instructions confers no added benefits compared with subspecialty-based medical care and education for asthma. 13 Therefore, the issue of the high number of children visiting EDs for nonsevere exacerbation cannot be addressed without a precise assessment of the actions undertaken before the ED arrival and the reasons that prompted these actions (WAAP, education by the subspecialist, phone advice, etc.).
To date, the expectations of patients who visit EDs for asthma exacerbation have been poorly studied; however, they may reveal useful information to prevent unnecessary ED visits. We performed a prospective multicenter study in asthmatic children visiting EDs for asthma exacerbation. Our main objective was to evaluate the proportion of potentially avoidable visits and their possible risk factors, such as WAAP. As an additional objective, we assessed the ability of families to evaluate the severity of exacerbations.
Materials and Methods
Children 6–18 years of age with known asthma and their families were eligible for this study when they were admitted to the ED for asthma exacerbation in 1 of the 6 participating hospitals located in the Ile-de-France region. The child's inclusion could not have been preceded by an ED visit for asthma within 8 days.
Asthma exacerbation was confirmed by the ED physician, and a 39-item questionnaire (30-item questionnaire if no WAAP was available at home) was filled out by the family. Nurses and physicians filled out 16 additional items on the day of the visit, and 4 last items 3–7 days after the visit in children with early discharge. Families who were unable to complete a questionnaire written in French were not included in the study. An associated disease requiring oral steroid treatment was an exclusion criterion.
The questionnaire recorded anthropomorphic data, health insurance status, family educational level [International Standard Classification of Education (ISCED) 2011, www.uis.unesco.org], the type of doctor in charge of the child's asthma care, the existence of a WAAP and its characteristics, asthma control in the previous month, the history and the severity of the present exacerbation, the usual treatment and the supplemental treatment received at home and in the ED, the family's reasons for coming to the ED, and the final outcome of the visit.
In practice, the nurses completed a few items of the questionnaire (age, gender, and weight, respiratory rate, pulse oximeter, and peak flow value), then gave the questionnaire to the parents, and remained available to answer any question from them. The physicians quoted the severity of the exacerbation by using the same items as those used by the parents. The items, recordable at home, were drawn from the Global Initiative for Asthma (GINA) Guidelines 2 : breathlessness; comfortable posture; ability to talk; alertness; accessory muscle and suprasternal retractions; and wheezing. Symptoms scored from 1 to 3 points (0 if missing), with the total score ranging from 0 to 18 (with higher numbers indicating more severe symptoms). Symptom control during the month that preceded the current exacerbation was evaluated as recommended by the GINA Guidelines, asking 4 questions (answered per week or per month as appropriate): “How frequent are the respiratory symptoms during the day?”; “How frequent is the use of reliever medication, excluding doses taken before exercise?”; “How frequent are the respiratory symptoms at night?”; and “How frequently has physical activity been restrained because of asthma?”
The questionnaire provided usual reasons for coming to the ED that were answered by “yes” or “no” by the family, but space was available for the family to write down any other specific reasons. The adequacy of the WAAP was qualitatively evaluated according to GINA Guidelines. 2 Patients were asked whether the WAAP included or not: the dose of bronchodilator per inhalation; the frequency of bronchodilator dosing; the use of a peak flow meter; information on when and how to commence prescribed oral corticosteroids (OCS); and when to seek medical advice, including the need for an ED visit.
For children who did not need hospitalization, a phone call was made 3–7 days after the visit to check for relapse within 48 h of the ED visit.
Because patients are taught through therapeutic education to seek medical advice if symptoms persist despite repeated administration of a bronchodilator (with or without OCS), and because adequate treatment [including high dose of bronchodilator (4–10 puffs every 20 min for 1 h) and OCS 2 ] of mild-to-moderate exacerbations can be achieved at home or by a local physician, we defined potentially avoidable ED visits (hereafter referred to as an “avoidable ED visit”) as visits by children who met the following 3 conditions: (1) no adequate prehospital treatment; (2) no more than 3 bronchodilator nebulizations (with or without OCS) before discharge; and (3) no relapse within 48 h. Inadequate treatment at home was defined as one or both of the following conditions: (1) absence of repeated dose of short-acting beta agonist in the first hour of the onset of the symptoms and/or no short-acting beta agonist during the 3 h preceding the ED visit; (2) no improvement or worsening after 12 h of symptoms duration, despite short-acting beta agonist use without OCS administration. 2
We hypothesized that WAAP would reduce avoidable ED visits. Children using symptom-based WAAP have a lower risk of exacerbations requiring acute care [Relative Risk: 0.73, 95% confidence interval (CI): 0.55–0.99]. 14 Based on literature and clinical experience in the Paris area,15,16 we hypothesized that 50% of children would have a WAAP, as we included children already diagnosed with asthma. The enrollment of 98 children was necessary to demonstrate a 25% reduction of avoidable ED visits (risk α 5% and power 80%) based on a 50% prevalence of avoidable visits. We, thus, planned to include at least 100 children.
Parents and children older than 8 years of age gave informed consent, and the study was approved by the Institutional Review Board of the French learned society for respiratory medicine (Société de Pneumologie de Langue Française) (CEPRO 2013-002).
Results were expressed as mean ± standard deviation or median (25th–75th percentile), as appropriate. Percentages were expressed with a 95% CI. Between-group (avoidable/nonavoidable or OCS/no OCS) comparisons were performed by using the Mann–Whitney test, Student's t-test, or the chi-squared test, as appropriate. Similar variables (such as severity score) were compared by using paired tests. A multivariable logistic regression with all significant risk factors in univariate analyses (independent variables) and avoidable visits as dependent variable was performed. A P value <0.05 was deemed significant. Statistical analyses were performed by using Statview 5.0 software (SAS Institute, Inc., Cary, NC).
Results
One hundred seven children were prospectively included during an 8-month study (from February to September 2013) in the 6 participating hospitals. The characteristics of the children and of their exacerbations are given in Table 1. The flow chart of their outcome is shown in Fig. 1.
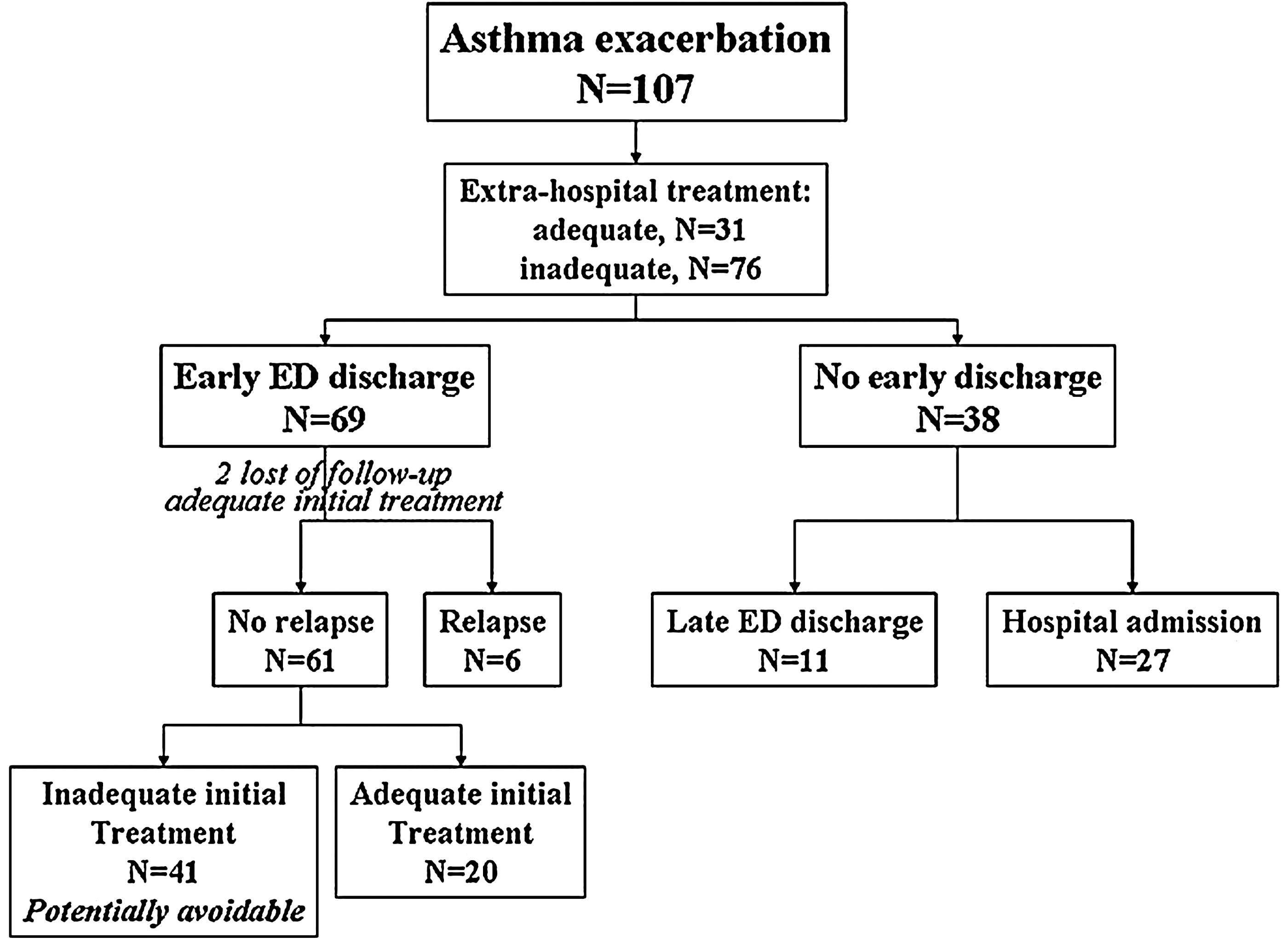
Flow chart from arrival at ED to final outcome. ED, emergency department.
Specialists are: pediatricians, pulmonologists, pediatric pulmonologists, and allergists. Results are means (standard deviation) or medians [interquartile range] or numbers. The first column is for descriptive purpose; the P values are related to the comparisons between “avoidable visits” and “non-avoidable visits” populations. The significance of P values in italics is expected/biased as by the definition of medically avoidable ED visits. Family educational level: Educational attainments were low when level 3 or less and medium-high when between levels 4 and 8 (ISCED 2011).
The significance of P value in bold is a p-value <0.05 that is not expected from the study design.
ED, emergency department; GP, general practitioner; OCS, oral corticosteroids; SABA, short-acting beta agonist; WAAP, Written Asthma Action Plan.
At arrival, 76 out of 107 children (71%, 95% CI: 62–80) had not received adequate treatment (Fig. 1). Among the 42 children (39%) with incorrect bronchodilator treatment, 16 (15%) had not received any reliever before arriving at the ED, and 26 children (24%) had received an insufficient dose of bronchodilator. Seventy-five children (70%) had not taken OCS before the ED visit, though 58 (54%) of them had an indication for it (severe or persistent mild-to-moderate exacerbation). Forty-one (38%, 95% CI: 29–48) children had made an ED visit that was classified as avoidable. The reasons for visiting the ED were numerous, and only 10 (9%) parents quoted just 1 reason for coming. The number of times each reason was quoted is summarized in Table 2. In addition to these reasons, 4 children had asthma symptoms during school hours and their parents were advised by the school staff to head to the ED.
The first column is for descriptive purpose; the P values are related to the comparisons between “avoidable visits” and “non-avoidable visits” populations.
The significance of P value in bold is a p-value <0.05.
MD, medical doctor.
Written Asthma Action Plan
The prevalence of the WAAP was 50/107, 47% (95% CI: 37–56) and was not associated with a reduction in avoidable visits, even when considering the most appropriate WAAP. The WAAP was mostly given by specialist practitioners (36/50, 72%). For instance, all children who were followed by a pediatric pulmonologist had a WAAP (n = 10). The WAAP was associated with a reduction of anxiety/fear recorded as one of the reasons for visiting the ED: 15/50 (30%, 95% CI: 17–43) in families with a WAAP versus 32/57 (56%, 95% CI: 43–69) in families without a WAAP; P = 0.007.
Risk factors for avoidable visits
A logistic regression, using the 2 relevant significant risk factors found in univariate analyses [care by a specialist doctor (eg, pediatrician, pulmonologist, allergist) and ED visit associated with fear/anxiety, Tables 1 and 2] as independent variables and avoidable visit as dependent variable, demonstrated that the risk of avoidable visits was reduced when the ED visit was not related to fear/anxiety [odds ratio (OR): 0.43, 95% CI: 0.19–0.97, P = 0.042].
Prehospital administration of OCS
Since prehospital administration of OCS was a frequent determinant of avoidable ED visits, we analyzed the characteristics of asthma exacerbations with respect to OCS administration. The results are given in Table 3. Interestingly, in children who received OCS at home, the decrease in severity of the clinical score between home and ED was greater than that of children who did not receive OCS at home (score decrease: 1.6 ± 2.0 versus 0.0 ± 1.9; P < 0.001).
The significance of P values in bold is p-values <0.05.
Exacerbation severity
An additional objective of our study was to assess the ability of families to evaluate the severity of asthma symptoms during exacerbation. As parents scored the maximal intensity of symptoms before visiting the ED, their score was only moderately correlated with the physician's score, established, using the same criteria, at ED arrival (r = 0.50, P < 0.001). This is probably partly due to differences in the progression of exacerbations. In all the study children, the score decreased from parents' to physician's evaluation (P = 0.024). When splitting the sample according to the progression of the exacerbation assessed by the parents (see “early progression” in Table 1), there was a significant difference in changes in score severity (maximal intensity scored by parents before ED visit minus severity at ED arrival scored by physicians) between children considered as improved and those considered as worsened [−1.1 ± 2.1 (n = 29) versus +0.1 ± 2.1 (n = 28); P = 0.041]. The latter result supports the ability of parents to correctly evaluate the severity of asthma exacerbation in their children.
Discussion
In our observational, prospective multicenter study, we found that, in France, the prevalence of avoidable ED visits for asthma exacerbation in children was high (38%, 95% CI: 29–48), despite half of the participating families possessing a WAAP (47%, 95% CI: 37–56). The WAAP was not associated with a significant reduction of avoidable ED visits, and 71% (95% CI: 62–80) of the children had not received adequate treatment before arriving at the ED. The only nontherapeutic modifiable risk factor for avoidable visits was anxiety/fear felt by parents at home. Parents could reasonably be involved in the management of their child's asthma exacerbation, as they proved to be capable of evaluating the severity and the course of the exacerbation by identifying simple symptoms.
The main objective of our study was to evaluate the proportion of avoidable ED visits, which calls for a definition of such visits. We focused on ED visits characterized by inadequate prehospital treatment and early discharge, because this inadequacy of treatment has to be addressed before other self-management aspects can be modified.
Children hospitalized for asthma exacerbation in France have previously been described as frequently undertreated and insufficiently educated about asthma. 17 A survey conducted in the Paris area showed that the majority of children admitted to the ED do not have a severe exacerbation, as demonstrated by the low hospitalization rate (25.4%), 9 similar to that described in our study (25.2%) and in a North American study. 10 These results suggest that a probable non-negligible proportion of children briefly treated in the ED could have been successfully treated at home or by a local physician. To our best knowledge, the percentage of avoidable ED visits for asthma exacerbations has not been determined in school-age children and adolescents already diagnosed as asthmatic. It has been found in 199 children that a medical phone contact during an asthma exacerbation increased the use of short-acting bronchodilators [adjusted OR: 3.6, 95% CI: 1.3–9.4] and of OCS (adjusted OR: 3.3, 95% CI: 1.3–8.4) preceding the ED visit, but the potential effect of the medical advice on the patients' outcome was not mentioned in the study. 8
The high prevalence of avoidable ED visits may have several explanations. First, health coverage in France is good and the accessibility to ED is easy in the urban area of the study. However, the majority of the children (n = 75, 70%) were recruited between 8 AM and 8 PM, a period during which local practitioners are available, and almost all the patients (n = 97, 91%) had total healthcare coverage. In 197 North American asthmatic children and their families who had easy healthcare access and a similar prevalence of the WAAP (43%) as our study children, the decision to go to the ED rather than to look for a local doctor (without further precisions as to the reasons behind that decision) was recorded in 30% of the cases. 18
Second, as previously shown, 17 patients are insufficiently educated about asthma and management of exacerbation. However, in our study, the presence of a WAAP was not associated with a reduction of avoidable visits, but there was a lower proportion of avoidable ED visits in children treated by an asthma specialist. It is probable that verbal instructions, such as an explanation on the noninferiority of a valve holding chamber versus nebulizers to deliver bronchodilators 19 or of the correct OCS indications (Table 3), play an important role in the self-management of asthma exacerbation, as previously suggested.13,20 Indeed, it is a routine practice in France to deliver bronchodilators via nebulizers in EDs, even though it is known that aerosols of bronchodilators used in conjunction to a valve holding chamber are as efficient for acute asthma treatment. Without specific explanations, most of the children and their parents may feel that nebulization is the most efficient treatment, which prompts them to visit the ED. 21
WAAPs were supplied by both general and specialized practitioners, and some of them did not include all necessary information for exacerbation treatment. However, even children with the most appropriate WAAP did not exhibit a reduced proportion of avoidable visits. This result is in line with those of Tan et al., 22 who demonstrated that the WAAP did not modify the likelihood of caregivers to either stop medications without consulting their physician or seek acute care consultation, nor did it improve caregivers' confidence in the self-management of their children's asthma. It has been stated that the WAAP should clearly indicate the course of action to follow, the expected response, and the expected timeline of the response. 23 Such objectives are challenging because of the restricted size of the WAAP (usually 1 page).
Feelings of fear or anxiety were one of the recorded reasons for visiting the ED and were associated with avoidable visits, suggesting that psychological factors may prompt acute care visits, despite the severity of the exacerbation. This association does not imply a causal relationship, but anxiety and fear felt by children and their families may promote ED visits since psychological factors have been associated with worse outcomes and a greater need for medical intervention. 24 Psychological triggers alone have been found to explain up to 34% of the variance in control of asthma symptoms. 25 Furthermore, it has been shown that severe life events, both on their own and in conjunction with high chronic stress, significantly increase the risk of new asthma attacks in children. 26 Thus, a high chronic stress level may contribute to the propensity for visiting the ED.
It is probable that in the near future action plans will exist in electronic form, but the issue of their appropriateness would have to be sorted out before broad dissemination. Smartphone and tablet self-management applications for asthma are emerging tools for the delivery of self-managed interventions, but their effectiveness remains to be demonstrated. 27 The challenge for an electronic Asthma Action Plan would be to reassure users, taking into account the exacerbation severity, and to deliver appropriate instructions as to what must be done right away and in the following hours and days.
Our study has some limitations, such as its descriptive nature. Risk factors for avoidable visits have not been previously described, and this study may, thus, seem preliminary. Our results are partly based on answers to a questionnaire filled out by the families during their stay in the ED (recall bias). Our sample size calculation was based on the WAAP prevalence; consequently, we may have overlooked less prevalent risk factors. Moreover, whether the risk factors evidenced are specific or not to the French health system remains an open question.
In conclusion, our observational multicenter study shows that avoidable ED visits for asthma exacerbation in children remain frequent (38% of visits are avoidable), and it suggests that the WAAP in its present form cannot reduce this frequency. Since the only identified risk factor of avoidable visits is fear/anxiety, the WAAP should aim at mitigating these feelings by providing readily available and adequate therapeutic advice. In the near future, applications for Smartphone or tablet giving such advice based on the severity of the exacerbation assessed by the parents could best suit this purpose.
Footnotes
Acknowledgment
The investigators received a grant from the Association CARDIF–L'Assistance Respiratoire (Director Dr. Fayssal El Husseini). No. CARDIF-12-017.
Author Disclosure Statement
No competing financial interests exist.