
Abstract
Although second-hand smoke (SHS) exposure is associated with asthma, its effect on eczema is unclear. Especially, the effect of maternal passive smoking on childhood eczema has rarely been studied. Polymorphisms in tumor necrosis factor-α (TNF-α), toll-like receptor 4 (TLR4), and glutathione S-transferase P1 (GSTP1) genes interact with air pollutants and modify allergic disease development. This study aimed to investigate the effect of gene–environment interactions between SHS exposure and TNF-α/TLR4/GSTP1 polymorphisms on childhood eczema. From 2005 to 2006, 3,639 children aged 7 or 8 years were enrolled and followed up 2 years later. Details of SHS exposure and eczema were collected by questionnaires. TNF-α (rs1800629), TLR4 (rs1927911), and GSTP1 (rs1695) genotypes were determined. Maternal passive smoking during pregnancy was associated with increased prevalence of eczema diagnosis ever (adjusted odds ratio [aOR] 1.50, 95% confidence intervals [CI] 1.25–1.79), and eczema symptoms in the past 12 months (aOR 1.23, 95% CI 1.01–1.50). Persistent SHS exposure (from the prenatal period to the present) was associated with increased prevalence of eczema diagnosis ever (aOR 1.40, 95% CI 1.19–1.66). Maternal passive smoking during pregnancy and persistent SHS exposure were associated with increased risk of new eczema diagnosis in children with TNF-α AA or AG (aOR 2.83, 95% CI 1.11–7.23 for maternal passive smoking during pregnancy; aOR 3.65, 95% CI 1.29–10.29 for persistent SHS exposure), TLR4 CC (aOR 3.02, 95% CI 1.38–6.63 for maternal passive smoking during pregnancy; aOR 2.31, 95% CI 1.01–5.28 for persistent SHS exposure), and GSTP1 AG or GG (aOR 2.58, 95% CI 1.23–5.42 for maternal passive smoking during pregnancy; aOR 3.04, 95% CI 1.32–7.01 for persistent SHS exposure) genotypes. Interactions between SHS and TNF-α/TLR4/GSTP1 polymorphisms may affect childhood eczema development. Reducing SHS exposure from the prenatal period may prevent childhood eczema in susceptible populations.
Introduction
E
Several studies have evaluated the association of SHS exposure and eczema for a specific time, such as the fetal period, early childhood, or adolescence. Therefore, the association between persistent SHS exposure and development of eczema remains unclear. It is also unclear whether the effect of SHS exposure persists in school children. About half of children with early-onset eczema have complete resolution by 7 years of age. 19 If eczema persists, it is associated with morbidity, such as school absenteeism and emotional stress in school children. 20 Therefore, it is necessary to evaluate the effect of persistent SHS exposure on eczema, which extends beyond early childhood.
Genetic factors as well as environmental factors have important roles in the development of eczema. Therefore, genetic factors need to be considered when evaluating the effect of SHS exposure on the development of eczema. However, there has been only 1 study that examined the interaction between gene and SHS exposure on eczema in children, showing that prenatal smoke exposure increased the risk of eczema in children with GSTM1 null and glutathione S-transferase P1(GSTP1) Ile/Ile genotypes. 21
Toll-like receptors (TLRs), the first-line effector molecules in the innate immune system, may play an important role in initiating immune responses induced by air pollution.22,23 The potent proinflammatory cytokine tumor necrosis factor-α (TNF-α) may modify the effect of smoke exposure on allergic diseases in children.24–26 GSTP1 is involved in detoxification of smoke-induced oxidative stress. 21 Therefore, genetic polymorphisms of TNF-α, TLR4, and GSTP1 may result in different responses to SHS, and SHS exposure may interact with these polymorphisms to influence the development of eczema. In particular, TNF-α (rs1800629), TLR4 (rs1927911), and GSTP1 (rs1695) polymorphisms were associated with allergic diseases in our previous studies.18,27,28
We investigated whether maternal passive smoking during pregnancy and the offspring's persistent SHS exposure increased the risk of eczema and whether genetic polymorphisms in TNF-α (rs1800629), TLR4 (rs1927911), and GSTP1 (rs1695) genes modified the effect of SHS on eczema in school children.
Materials and Methods
Subjects and study design
From 2005 to 2006, a total of 3,639 first- or second-grade elementary school children were recruited from 29 elementary schools in 10 Korean cities. Participants were followed up 2 years later, and the follow-up rate was 70.4%. Prevalence of eczema and history of SHS exposure were assessed using the modified International Study of Asthma and Allergies in Childhood questionnaire.29,30 This study was approved by the Institutional Review Board of the Asan Medical Center, University of Ulsan College of Medicine. Written consent was obtained from all parents and guardians following a detailed explanation of the study.
Assessment of SHS exposure
We categorized SHS exposure into 2 subtypes (maternal passive smoking during pregnancy and offspring's persistent SHS exposure) to evaluate whether there were different effects of SHS exposure on eczema with regard to the exposure period.
Maternal passive smoking during pregnancy was defined as smoking by any other household member at any time during the pregnancy when the mother was not smoking and assessed with the following question: “Did other household members smoke during pregnancy?” The offspring's postnatal SHS exposure was defined as smoking by household members (parents and other members, if present) and assessed with the following question: “Did any household member smoke from after the child's birth until the present time?” Persistent SHS exposure was defined as exposure from the prenatal period to the time of the second survey, and children were considered to have persistent SHS exposure if they answered “yes” to the 2 questions. Exposure to each type of SHS was dichotomized (yes/no).
Assessment of eczema
Eczema was assessed with the following questions: “Has your child been diagnosed with eczema by a physician at any time during his/her lifetime?” (Eczema diagnosis ever) and “Has your child had an itchy rash at any time in the past 12 months?” (Eczema symptoms in the past 12 months).
Skin prick test
Skin prick tests were performed using 16 common Korean inhalants and food allergens (Allergopharma, Reinbek, Germany); Dermatophagoides pteronyssinus, Dermatophagoides farinae, cat dander, dog dander, cockroach, Alternaria alternate, Aspergillus fumigatus, grass, tree mix (I), tree mix (II), mugwort, ragweed, egg, milk, peanut, and soybean. Histamine (10 mg/mL) was used as a positive control, and normal saline as the negative control. Each allergen solution was pricked into the skin on the volar surface of the child's forearm. The procedure was repeated for each allergen and for the controls using a new lancet for each allergen. Wheal size was recorded after 15 min, taking the largest diameter and the diameter at 90° to its midpoint. Mean wheal diameter was calculated as the average of the 2 diameters. Allergen mean wheal diameter 3 mm or greater and equal or greater than the histamine wheal diameter was considered a positive skin prick test result. Atopy was defined as the presence of 1 or more positive reactions from the skin prick test. 17
Genotyping
The single-nucleotide polymorphism in TNF-α promoter (rs1800629) was genotyped using the single base extension method, as described previously. 27 Genotyping of the TLR4 (rs1927911) and GSTP1 (rs1695) polymorphisms was performed using a TaqMan assay (ABI, Foster City, CA).28,31 The 5 μL polymerase chain reaction (PCR) mixtures contained 10 ng of genomic DNA, 2.5 μL of TaqMan Universal PCR Master Mix, and 0.13 μL of 40 × Assay Mix. The thermal cycling conditions were as follows: 50°C for 2 min (to activate uracil N-glycosylase and prevent carryover contamination), followed by 95°C for 10 min (to activate the DNA polymerase), and then, 45 cycles of 95°C for 15 s and 60°C for 1 min. All PCRs were performed using 384-well plates and a 384-well Veriti Thermal Cycler (ABI), and the endpoint fluorescent readings were performed using an ABI PRISM 7900 HT Sequence Detection System (ABI). Duplicate samples and negative controls were included to ensure accuracy of genotyping.
Statistical analyses
Statistical analyses used SAS version 9.2 software (SAS Institute, Inc., Cary, NC). To determine the association between SHS exposure and eczema, adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were calculated using logistic regression models. In multivariate analyses, sex, body mass index, maternal education level, and parental history of allergic disease were adjusted. For all analyses, P < 0.05 was considered statistically significant. Multiple testing problems were adjusted by false discovery rates (FDR). FDR was calculated by p,adjust function in R software with “Hochberg” option.
Results
Characteristics of the study population
The mean age of participating children was 7.7 ± 0.5 years and 52.5% were male. Schools were randomly selected from 3 districts of Korea (city: 25.9%; industrial: 43.2%; farming and fishing villages: 30.9%). Prevalence of maternal and paternal histories of allergic disease was 17.1% and 17.3%, respectively (Table 1).
Prevalence of SHS exposure and eczema
SHS exposure rates for maternal passive smoking during pregnancy were 20.9% and those for persistent SHS exposure were 14.6%. The prevalence rates of eczema were as follows: eczema diagnosis ever, 31.7%; eczema symptoms in the past 12 months, 22.3%; and new eczema diagnosis, 6.4% (Table 2).
Persistent SHS exposure was defined as SHS exposure from the prenatal period to the time of the second survey.
New eczema diagnosis was defined as eczema diagnosis at the second but not the first survey.
SHS, second-hand smoke.
Effects of maternal passive smoking during pregnancy and persistent SHS exposure on the risk of eczema
Maternal passive smoking during pregnancy was associated with increased prevalence of eczema diagnosis ever (aOR, 1.50; 95% CI, 1.25–1.79); and eczema symptoms in the past 12 months (aOR, 1.23; 95% CI, 1.01–1.50). Persistent SHS exposure was associated with increased prevalence of eczema diagnosis ever (aOR, 1.40; 95% CI, 1.19–1.66). New eczema diagnosis was not associated with either maternal passive smoking during pregnancy or persistent SHS exposure (Table 3).
Adjusted for sex, body mass index, maternal education level, and parental history of allergic disease.
New eczema diagnosis was defined as eczema diagnosis at the second survey, but not at the first.
Persistent SHS exposure was defined as SHS exposure from the prenatal period to the time of the second survey.
aOR, adjusted odds ratio; CI, confidence interval; SHS, second-hand smoke.
We further evaluated whether the effect of SHS exposure on eczema could be different by allergen sensitization. The association of maternal passive smoking during pregnancy with childhood eczema symptoms in the past 12 months differed by the presence or absence of allergic sensitization (p for interaction, 0.074). For children without allergic sensitization, the association of maternal passive smoking during pregnancy with childhood eczema symptoms in the past 12 months was not statistically significant (aOR, 1.14; 95% CI, 0.80–1.63). For children with allergic sensitization, the association of maternal passive smoking during pregnancy and childhood eczema symptoms in the past 12 months was statistically significant (aOR, 2.07; 95% CI, 1.22–3.49). Similarly, the effects of persistent SHS exposure on the risk of eczema symptoms in the past 12 months differed by the presence of allergic sensitization (aOR, 0.93; 95% CI, 0.62–1.40 for children without allergic sensitization and aOR, 1.89; 95% CI, 1.06–3.38 for children with allergic sensitization, p for interaction, 0.068) (Table 4).
Adjusted for sex, body mass index, maternal education level, and parental history of allergic disease.
New eczema diagnosis was defined as eczema diagnosis at the second survey, but not at the first.
Persistent SHS exposure was defined as SHS exposure from the prenatal period to the time of the second survey.
aOR, adjusted odds ratio; CI, confidence interval; SHS, second-hand smoke.
Associations between SHS exposure and polymorphisms in TNF-α, TLR4, and GSTP1 genes on the risk of new eczema diagnosis
TNF-α (rs1800629), TLR4 (rs1927911), or GSTP1 (rs1695) polymorphisms did not have a significant impact on eczema diagnosis ever and eczema symptoms in the past 12 months (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/ped). After adjustment for estimated FDR, TNF-α (rs1800629), TLR4 (rs1927911), or GSTP1 (rs1695) polymorphisms did increase the risk for new eczema diagnosis in children exposed to maternal passive smoking during pregnancy (Figs. 1a–3a) and in children with persistent SHS exposure (Figs. 1b, 2b, and 3b). Under the consideration of multiple testing problems, the effect of TLR4 with maternal passive smoking during pregnancy is uniquely significant at the 0.05 significance level, but its interaction with persistent SHS exposure also reveals promising significance.
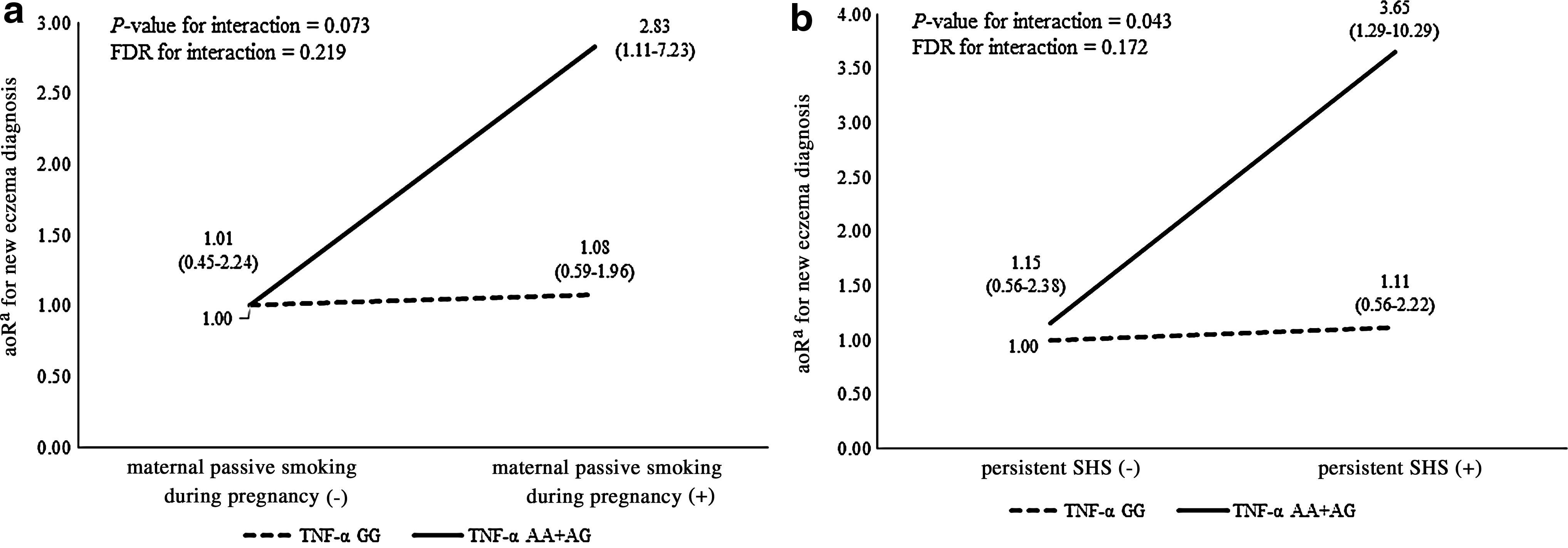
Influence of TNF-α (rs1800629) genotypes, with

Influence of TLR4 (rs1927911) genotypes, with
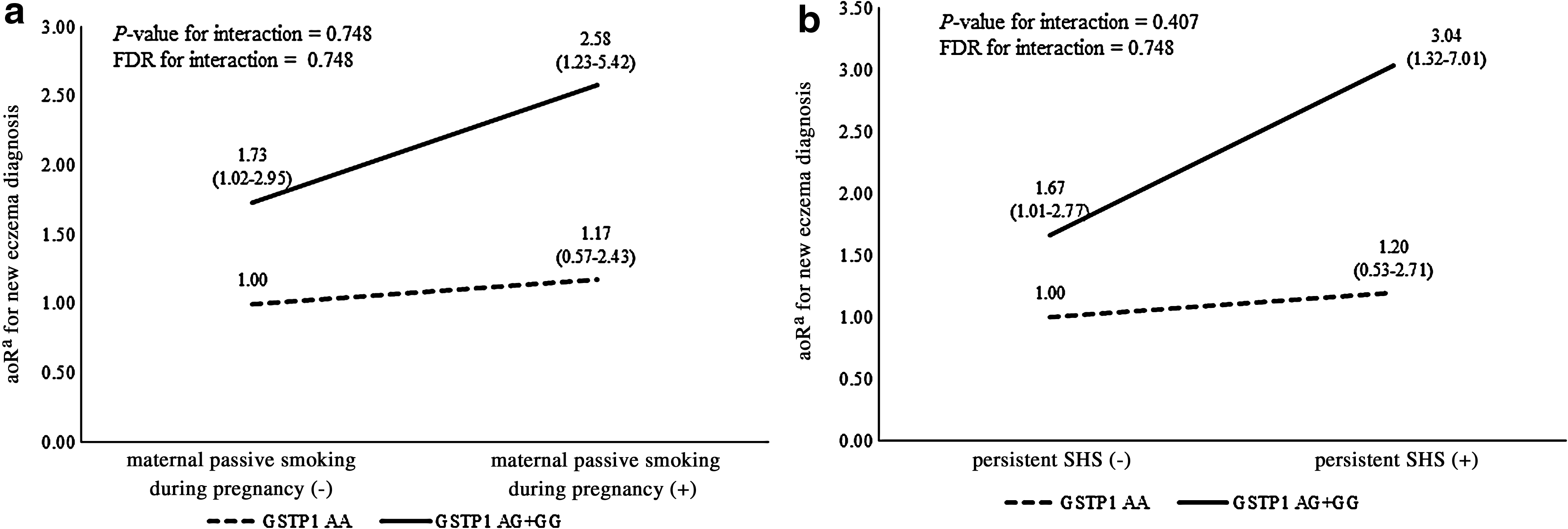
Influence of GSTP1 (rs1695) genotypes, with
Discussion
This study found that both maternal passive smoking during pregnancy and offspring's persistent SHS exposure were associated with the risk of eczema prevalence in Korean school children. We also found associations between SHS exposure and development of eczema in school children with the AA or AG genotypes of TNF-α (rs1800629), the CC genotype of TLR4 (rs1927911), and the AG or GG genotypes of GSTP1(rs1695). This study showed further results than previous study, 30 suggesting the importance of the interaction between genetic polymorphisms and SHS exposure, including maternal passive smoking during pregnancy on childhood eczema.
The prenatal period has been considered a critical determinant for development of eczema.8,10,32–34 However, the evidence supporting an association between prenatal SHS exposure and eczema in children appears inconsistent, and the relationship has not been investigated sufficiently.8–11 Moreover, the effect of maternal passive smoking during pregnancy on the offspring's eczema has rarely been studied. Only 2 studies have shown the association between maternal passive smoking during pregnancy and eczema in children.16,17 Our study suggested that maternal passive smoking during pregnancy also had important effects on the fetus, which persist until childhood. Not only maternal passive smoking during pregnancy but persistent SHS exposure from the prenatal to the current period also associated with eczema in school children. Although it is difficult to distinguish between the effect of prenatal SHS exposure from that of postnatal exposure or persisting exposure over both periods, previous studies have evaluated the effect of SHS exposure during specific periods. Further studies exploring the effect of persistent SHS exposure on eczema and in relation to the relevant SHS exposure period are required.
SHS exposure increases the risk of allergic sensitization and eczema development by altering immune responses and increasing the allergenicity of allergens.35–38 There are studies suggesting that prenatal or postnatal SHS exposure increases the risk of atopic eczema.9,39 Our results are consistent with these findings in terms of allergen sensitization. The risk of eczema symptoms in the past 12 months in maternal passive smoking during pregnancy and with persistent SHS exposure was more significant in atopic children than in nonatopic children.
The AA or AG genotypes of TNF-α (rs1800629), the CC genotype of TLR4 (rs1927911), and the AG or GG genotypes of GSTP1 (rs1695) increased the risk of new eczema diagnosis during the follow-up period in children with maternal passive smoking during pregnancy and in persistent SHS exposure. Overall, these results suggest that the effects of maternal passive smoking during pregnancy on the risk of developing eczema continue until later childhood and may be modified by genetic factors. It is unclear why the interaction between SHS exposure and the polymorphisms of TNF-α, TLR4, and GSTP1 was significant only in new eczema diagnosis. There are possible mechanisms described in other studies. SHS exposure increases allergic sensitization over time, rendering children susceptible to the development of childhood-onset eczema. 40 SHS exposure also impairs the skin barrier function. An impaired skin barrier allows the ingress of allergens, bacteria, and viruses, thereby affecting new development of eczema. 41 Genetic polymorphisms may have an important role in children's susceptibility to SHS exposure, promoting new development of eczema. 42
Maternal smoking during pregnancy inhibited neonatal immune responses to TLR ligands and defective TLR4 signaling, resulting in skin barrier dysfunction and allergen sensitization.43,44 TNF-α also increases after cigarette smoke exposure. 24 The risk of allergen sensitization following air pollution is increased in children with polymorphisms of TNF-α. 45 SHS is a major source of free radicals and SHS-induced oxidative stress promotes Th2 differentiation. 46 In terms of oxidative stress, polymorphism of GSTP1 is associated with adverse effects of prenatal smoke exposure. 21
This study has several limitations. First, SHS and eczema data were derived from questionnaires; therefore, the possibility of recall bias cannot be excluded. As the information was gathered via parental questionnaires, some exposure misclassification is likely. In future studies, the use of more objective and precise measures of SHS exposure may help to clarify the association with eczema. Second, we only selected 1 polymorphism from each gene, although it should be noted that previous studies have demonstrated relationships between these polymorphisms and susceptibility to allergic diseases.27,28,31 In terms of its strengths, this nationwide study enrolled more than 3,000 children and the response rate to the questionnaire was greater than 95% and could be considered representative of an Asian country. In addition to examining the effects of maternal passive smoking during pregnancy and persistent SHS exposure on eczema, we also investigated gene–environment interactions related to TNF-α, TLR4, and GSTP1.
In conclusion, this study suggested that both maternal passive smoking during pregnancy and persistent SHS exposure are associated with eczema in school children. The effects of maternal passive smoking during pregnancy and persistent SHS exposure on the eczema symptoms were more significant in school children who were atopic than in those who were not. In particular, AA or AG genotypes of TNF-α (rs1800629), the CC genotype of TLR4 (rs1927911), and the AG or GG genotype of GSTP1 (rs1695) increased new eczema diagnosis in children exposed to maternal passive smoking during pregnancy and persistent SHS. Overall, the effects of maternal passive smoking during pregnancy and persistent SHS exposure on the risk of developing eczema continue until childhood and may be modified by genetic factors. Efforts should be made so that pregnant women are not exposed to SHS. Avoiding SHS exposure in pregnant women and children may reduce the occurrence of eczema in children, especially in those who are genetically susceptible.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.