
Abstract
Maximizing clinical efficiency through the reduction in inpatient length of stay (LOS) using standardized protocols has been a major objective among hospital administrators, most notably in the context of recent healthcare reimbursement changes at statewide levels. The objective of our project was to determine whether a synchronous change in an inpatient asthma protocol that relied on a respiratory therapist (RT)-driven bronchodilator weaning algorithm and bronchodilator therapy given through a metered dose inhaler (MDI) plus valved holding chamber (VHC) could impact clinical and financial outcomes. A pre-post study assessed patients aged 2–21 years of age admitted with a primary diagnosis of status asthmaticus. The effect of the protocol was measured from October 2014 to July 2015. Outcome variables included patient demographics, hospital LOS, all-patient refined diagnosis-related groups (APR-DRGs), and inpatient charges. Outcomes were compared between the preimplementation and postimplementation time periods. Statistical significance was measured using Wilcoxon signed-rank test and bootstrap logistic regression models. Protocol patients (n = 110) had a similar demographic and clinical profile compared with the matched population from the previous nonprotocol fiscal year (n = 150). Use of the protocol resulted in a significantly reduced LOS that maintained significance after adjusting for APR-DRGs weight (P < 0.05). The protocol did not alter the total hospital billing charges. A nonstatistically significant reduction in 30-day readmission rates was observed among those administered the protocol. An RT-led weaning protocol using a quantitative scoring system and MDI+VHC for bronchodilator administration resulted in a significantly reduced LOS.
Introduction
T
We at Johns Hopkins Children's Center (JHCC) recently undertook the task of revising the inpatient asthma care guidelines for patients in non-intensive care units (ICUs) in a manner that was consistent with both national guidelines and select national pediatric hospital protocols.10–12 The revision was undertaken after a routine institutional review of the protocol by various JHCC stakeholders requested updates to adhere to contemporary evidence-based guidelines. Beyond the major clinical focus of our endeavor, it was also administratively significant given recent statewide healthcare policy changes enacted in Maryland. The state's health services cost review commission recently enacted a global budget revenue model that provides a fixed amount of annual revenue to hospitals for services that they provide to in-state residents, thus providing an incentive for hospitals to be more efficient (eg, reducing LOS). 13
The previous asthma protocol employed at JHCC in non-ICU settings had key features that were identified as being potentially modifiable components to enhance process efficiency: (1) house staff used a nonscoring-based combination of qualitative and quantitative criteria to assess clinical response to bronchodilators, (2) respiratory therapists (RTs) would be responsible for administering solely nebulized albuterol therapy as directed by the physicians, (3) bronchodilator weaning could only be implemented upon direct patient assessment by house staff.
We incorporated the insight from a multidisciplinary collaborative of inpatient asthma stakeholders to develop a protocol that emphasized a quantitative scoring system, serving as the foundation for an RT-driven bronchodilator weaning algorithm, which, in turn, delineates the administration of albuterol preferably through a metered dose inhaler (MDI) plus valved holding chamber (VHC). The intervention was implemented during a study time period when no other asthma or related inpatient discharge initiative was occurring. This article describes the impact of this multipronged intervention on the primary outcome of average LOS and secondary outcomes of inpatient billing charges and readmission rates.
Methods and Materials
Setting
JHCC is Maryland's largest children's hospital with 205 beds and ∼9000 admissions per year. Asthma exacerbation or status asthmaticus constitutes the primary diagnosis in 4% of cases requiring inpatient admission. Our staff includes an estimated 620 nurses, 80 RTs, 35 pediatric pharmacists, 82 pediatric house staff, and 143 attending physicians.
Planning the intervention
The asthma protocol was intended to standardize inpatient asthma care in non-ICU settings at JHCC using input from a multidisciplinary asthma steering committee. Members of the group included leadership or designated asthma specialists/educators in the Departments of Pediatric Nursing, Respiratory Therapy, Pharmacy, General Pediatrics, and Pediatric Pulmonology. Input from the Department of Pediatrics included faculty affiliated with residency education and house staff leadership. The protocol was aligned with best practice guidelines from the National Heart, Lung, and Blood Institute. 8 Components of the final protocol were also compared with inpatient asthma protocols from comparable pediatric academic medical centers.1,11,12
Patients transferred from the ICU to a floor bed were permitted to be placed on the protocol, but were not incorporated into the analyses. Our study did not include patients transferred from the ICU since the protocol was not administered in the setting and thus provider-specific management led to variability in costs and LOS. Patients were managed by either the General Pediatrics or Pediatric Pulmonary inpatient care teams. Decision support tools were built into the electronic health records (EHRs) and included an order set with links to descriptions of the protocol components. Scheduled electronic mail messages that described the ordering of the pathway on the EHR system were sent to the house staff assigned to each month's general pediatric and pulmonary inpatient services. Previously available order sets that pertained to bronchodilator therapy were maintained to provide status quo options for patients not meeting the protocol's inclusion criteria.
A quantitative pediatric asthma score (PAS) was used in replacement of combined qualitative and quantitative clinical criteria used as a guide for bronchodilator weaning (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/ped). The PAS was adapted from previous validated scoring mechanisms. 1 The score relied on measurement of 5 clinical criteria: respiratory rate, auscultation, accessory muscle use, oxygen saturations, and functional level of dyspnea (Supplementary Table S2). Each measure was subdivided into 3 severity categories with each worth 1 additive point, whereby a maximum of 3 points was assigned for the highest grade of clinical severity. Scoring of dyspnea during sleep was dependent on the caregiver's report of the patient's ability to converse, eat, or play immediately before sleep. If caregivers were not at the bedside or if uncertainty of the reported level of dyspnea existed, the child was awoken for dyspnea assessment. The frequency of bronchodilator administration was adapted from an algorithm that assessed the absolute value of the PAS and time spent in select bronchodilator phases (Supplementary Table S3). 10
The PAS was measured by the RT and confirmed by the patient's registered nurse (RN) at the time of planned bronchodilator treatments, after administration of intensification regimens or during any period in which concern for the clinical status worsens. All RNs and RT-derived PASs were entered in the EHR within decision support flow sheet categories. Discrepant scoring was resolved by assessment of house staff who could rely on their own clinical assessment or self-determined PAS value.
Albuterol through MDI+VHC was the default choice for β2-agonist administration. RTs were the only healthcare staff who administered bronchodilators. The dosage of albuterol was modified based on the phase of bronchodilator delivery (eg, increased actuations at Q2 compared with Q4 hour dosing) (Supplementary Table S4). Albuterol nebulization was permitted on an as-needed order for patients who were unable to comply with VHC-based delivery. Intensification mandated the use of dual albuterol and atrovent nebulization therapies for 3 consecutive doses, along with further medical management directed by house staff. Levalbuterol was not part of the protocol and was considered a variance if used. Hospital discharge required fulfillment of several criteria, with the most notable being clinical stability, as documented by low PASs during at least 2 consecutive albuterol treatments provided every 4 h and an adequate home management plan.
All identified stakeholders were educated between 15 and 30 days before the hospital-wide initiation of the protocol. Education was provided using lecture series, small group discussions, handouts, case examples, and e-mail reminders. Daytime and evening lectures were provided to RTs and RNs to maximize awareness of its components among shift workers. Stakeholders were given laminated cards that provided a summary of the PASs and bronchodilator weaning algorithm. After implementation, stakeholders were requested to provide any reasons for divergence from the protocol. Feedback was also requested on a weekly basis from stakeholder leadership 3 months postinitiation to address issues of durability and sustainability.
Study population
Inclusion criteria included children aged 2 to 21 years with a primary diagnosis of status asthmaticus or acute asthma exacerbation. Exclusion criteria included the following diagnosed comorbidities: (1) chronic lung disease (eg, bronchopulmonary dysplasia, cystic fibrosis, and ventilator-dependent respiratory failure); (2) lower airway pathology (eg, bronchiolitis and airway malacia); (3) upper airway pathology (eg, croup, vocal cord disorders, airway malacia, and presence of tracheostomy); (4) heart disease (eg, congenital or acquired heart defect and cardiac arrhythmias); and (5) acute chest syndrome. Children with an empiric or proven diagnosis of bacterial pneumonia were recommended to be monitored for nonbronchodilator responsive respiratory symptoms. Diagnoses were based on the International Classification of Diseases, Ninth Revision codes.
Study design and duration
This quality improvement study was evaluated using a pre-post study design with an historical control group. The preimplementation period was from October 2013 to July 2014 and the postimplementation time period was from October 2014 to July 2015. Similar time periods were used for comparison to accommodate for seasonal variations in disease presentation. The study was notably truncated from the planned 1-year to 9-month interval secondary to observed acute decline in protocol usage, which mandated the need for review and re-education among the stakeholders. Study approval was obtained per the Johns Hopkins Schools of Medicine Institutional Review Board.
Data collection
All outcome measures were derived from administrative databases within JHCC Department of Finance. 14 Johns Hopkins Medicine (JHM) Casemix DataMart was accessed for patient demographics, admission, discharge, billing details, and readmission data. Demographic data included age, gender, and race. LOS was measured by the time of admission to discharge order entry in the EHR (Allscripts Sunrise Clinical Manager, Chicago, IL). Financial metrics included all-patient refined diagnosis-related groups (APR-DRGs) that classifies patients based on severity of illness, risk of mortality, and resource utilization. APR-DRGs are numbered sequentially from 1 to 4, which indicate, respectively, minor, moderate, major, or extreme severity of illness or risk of mortality. Billing data included items ascribed to room and board, drugs, radiology, supply, therapy, and other ancillary charges. Physician service charges were not included in the utilization charges review. Thirty-day hospital readmissions were reviewed among the 5 inpatient JHM-affiliated institutions serving children within the state of Maryland.
Determination of patients in whom the pathway had been used required a 2-step process. Patients with a primary diagnostic ICD-9 code of asthma (ICD9 493.xx) were obtained from Casemix DataMart. Patient names were then cross-tabulated with inpatient orders to review order entry for the protocol. EHRs were further reviewed to determine whether appropriate inclusion and exclusion criteria had been applied to all screened patients acquired through Casemix DataMart. Protocol concerns were addressed in real time by members of the asthma steering committee, including the lack of enrollment of potential enrollees meeting inclusion criteria.
Data analysis
We compared patient characteristics between preimplementation and postimplementation using chi-square testing for categorical variables. The primary outcomes were hospital LOS and billing charges. Distributions of the untransformed LOS and charge data were non-normally distributed. Due to the observed skewed distribution, variables presented in control charts were presented with the central line as the median value; control limits among the protocol cohort were represented as the first and third interquartile range to more accurately reflect statistical dispersion. Due to the uneven group sizes and small sample size, a traditional bootstrapping with replacement technique was used to measure the mean difference in primary outcomes between the preimplementation and postimplementation time periods. The underlying assumption of bootstrapping was that our original data set serves as the parent population and is representative of the larger population to which our study wishes to draw inferences. 15 The 1,000 bootstrap data sets were analyzed using logistic regression with the final model using a fixed number of covariates. A level of 0.05 was used to test for significance. Analyses were conducted using Stata 12 (StataCorp LP, College Station, TX).
Results
We enrolled 110 participants in the new protocol as direct admissions from the pediatric emergency department, as compared with 150 in the previous fiscal year (FY) time period (Supplementary Fig. S1). The preimplementation and postimplementation cohorts were not statistically different based on select demographic indicators (Table 1). There was no significant difference in administrative classification based on APR-DRGs disease severity classification between the 2 cohorts. All enrollees had been appropriately enrolled with no identifiable presence of exclusion variables. A total of 22 patients were admitted with a primary diagnosis of asthma and had not been ordered the protocol, of which 7 met inclusion criteria. Two of these 7 patients who met inclusion criteria but were not ordered for the protocol were admitted with requirements of albuterol therapy every 3 h and discharge occurred in ≤1 day. The remaining 5 potential enrollees were admitted to the pulmonary service who determined that their baseline classification of severe asthma required closer house staff oversight or preferred need for nebulized therapy. The majority of potential enrollees were admitted in the first 3 months postprotocol initiation. Weaning had occurred as delineated in the protocol's decision support with the exception of 5 patients. Three of these patients were reported to be weaned too rapidly and the remaining 2 were deemed to be weaned too slowly, based on physician clinical assessment. Weaning issues were documented and reviewed with the pertinent stakeholders and all patients were maintained on the protocol.
Among the 15 children who were not ordered the protocol based on fulfillment of exclusion criteria, all but 4 had a diagnosis of chronic lung disease and were admitted to the pulmonary service. The basis for the chronic lung disease included history of bronchopulmonary dysplasia, interstitial lung disease, or ventilator dependence. The remaining 4 patients who had also met exclusion criteria were diagnosed with congenital heart disease or comorbid vocal cord dysfunction.
Patients receiving albuterol through MDI+VHC or nebulization therapy did not experience any adverse effects. Albuterol nebulization was most often prescribed by the house staff as an as-needed order during time points of sleep when the patient did not appear to be compliant with the required MDI+VHC technique, although all patients were administered albuterol through an MDI+VHC during the majority of their inpatient stay. There was no RT reported usage of nebulized therapy of patients on the protocol while awake. There were no reported cardiovascular complications associated with the protocol's albuterol MDI dosing. Three patients with discrepant PASs between the RTs and RNs were resolved with house staff-determined scoring. There were no significant differences in the 30-day inpatient readmission rates between the groups (Table 1). Two children initially admitted on the protocol required intensification. One patient responded well to intensification therapy and subsequently continued the weaning of bronchodilators based on the protocol. The other child was admitted to the ICU within 12 h of admission requiring more comprehensive medical management; they were transferred back to a non-ICU floor for nonprotocol-based bronchodilator weaning. There were no reported parental concerns regarding any of the protocol components. There was no mortality reported during the study interval among all individuals admitted with a primary diagnosis of asthma, regardless of protocol administration.
The LOS was statistically reduced in the postimplementation cohort than in the preimplementation cohort (Table 2). The difference in LOS remained significant after APR-DRG-adjusted weight in the model (Fig. 1). Despite the reduced LOS, there was no meaningful change in the average total inpatient billing charge. The difference in LOS among the preimplementation and postimplementation time periods (mean difference <1 day) did not alter the room and board service charges. The radiology and laboratory charges were the only 2 subcategories of charges with significant reductions; neither could be attributed to the effects of the intervention since the protocol did not address the usage of these components. Changes in the radiology and laboratory charges were assigned to emergency room, not inpatient floor-related initiatives. Despite the higher charges associated with albuterol through MDI+VHC, compared with charges by nebulized therapy, the medication charges were not statistically dissimilar among the groups (Table 2, Fig. 2).
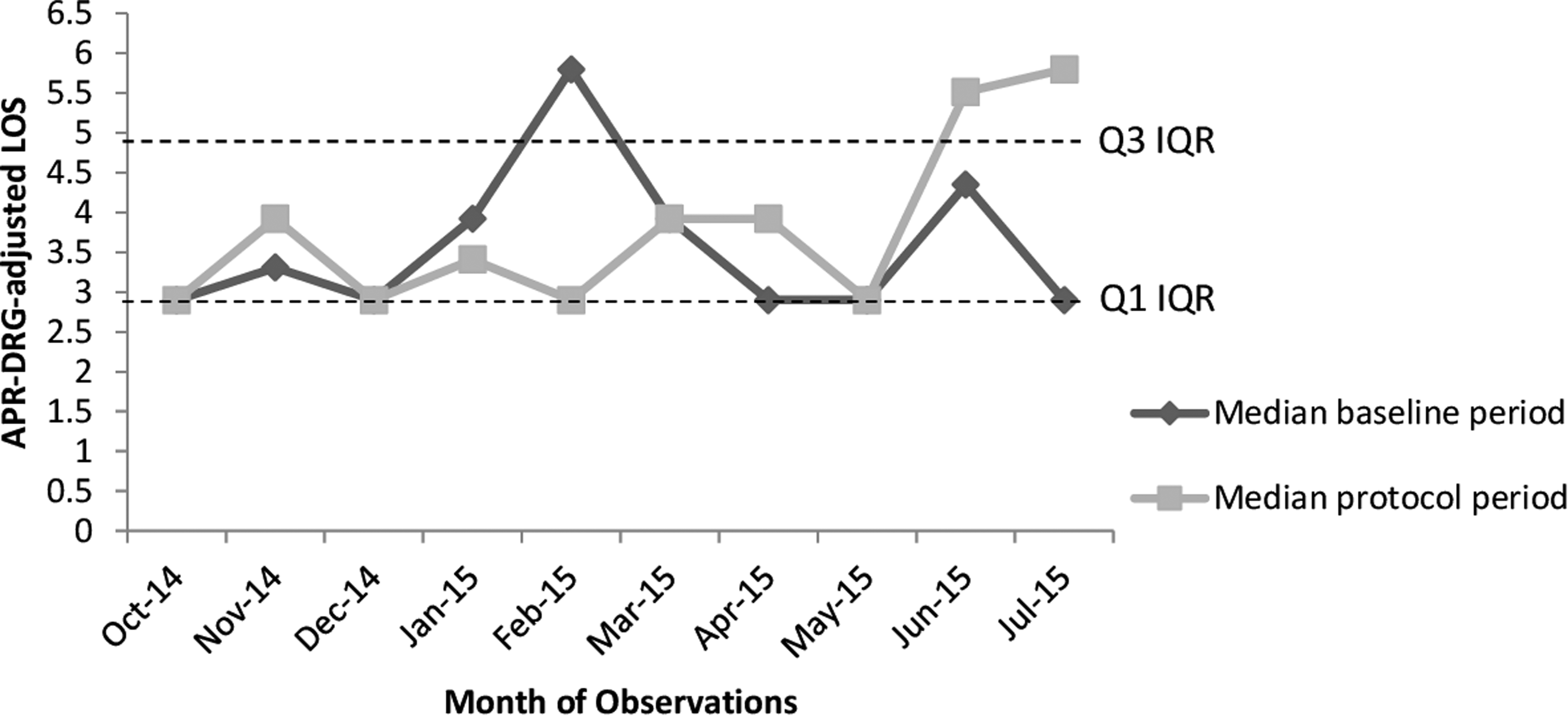
Protocol APR-DRG-adjusted LOS, relative to the preimplementation fiscal year. APR-DRGs, all-patient refined diagnosis-related groups; IQR, interquartile range; LOS, length of stay; Q1, first quartile; Q3, third quartile.
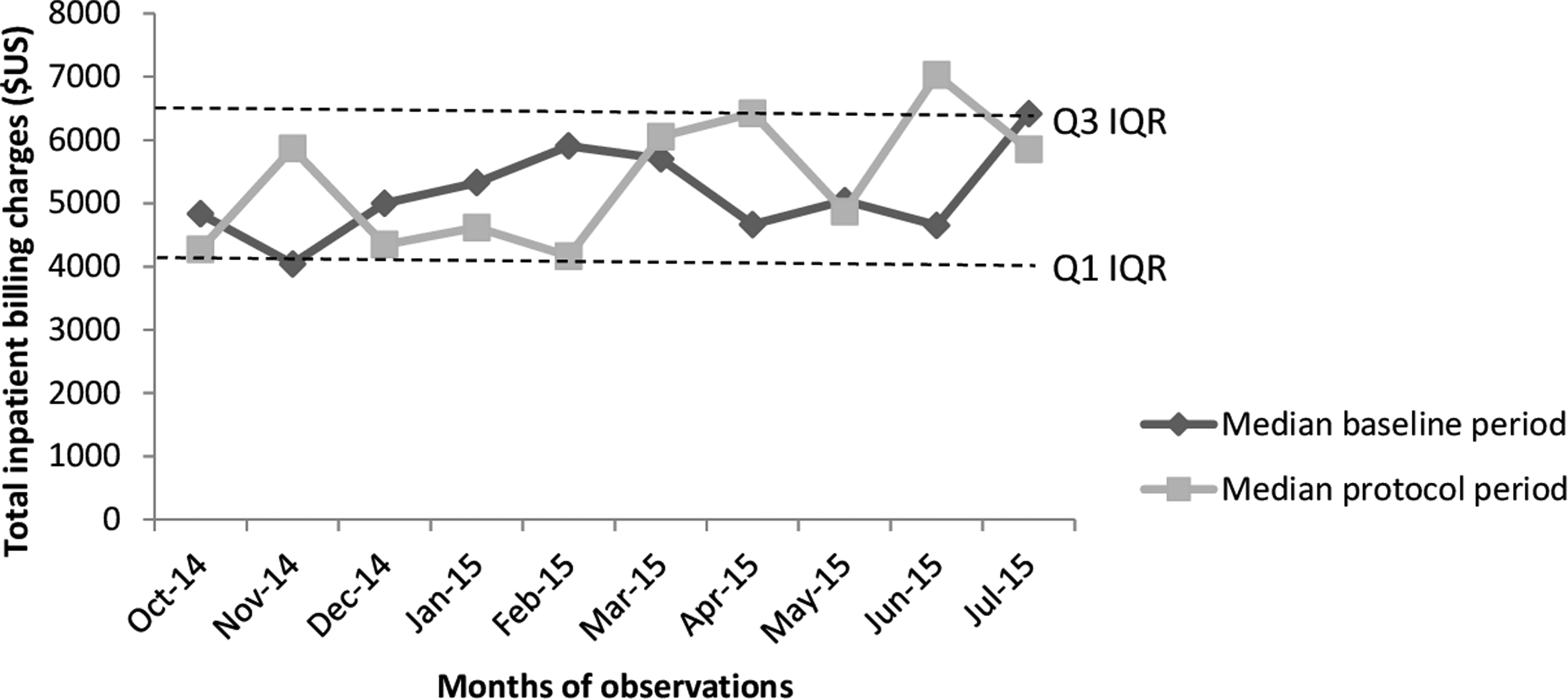
Protocol total inpatient billing charges ($U.S.), relative to the preimplementation fiscal year. Q1, first quartile; Q3, third quartile.
represents a statistically significant difference.
APR-DRGs, all-patient refined diagnosis related groups; LOS, length of stay.
Inpatient asthma admissions had notably declined in both preimplementation and postimplementation cohorts starting in May of each FY, which corresponded to a seasonal decline in disease exacerbation during the summer months (Supplementary Fig. 1). Despite the seasonally attributed decline in admissions, there was a remarkable decline in the protocol usage in July 2015, which mandated the need for a comprehensive stakeholder review and refinement of ongoing educational strategies. This study was terminated after 9 months of recorded observations, but the protocol continues to be used in JHCC under the supervision of the asthma steering committee leadership.
Discussion
This study demonstrates an inpatient asthma protocol that successfully adapted major components within national and pediatric center-specific asthma guidelines in a large academic medical center.10–12 The developed protocol leveraged the expertise of a multidisciplinary stakeholder team to replace an existing asthma pathway that had notable limitations. The new protocol mandated the synchronous enactment of several changes to inpatient asthma care—which included an RT-led bronchodilator weaning algorithm, asthma scoring system, and albuterol administration with preferred delivery through MDI+VHC. In the process of implementing this approach, we appreciated that the protocol components increased the autonomy and decision-making capacities of the RTs, while maintaining the educational and supervisory responsibilities attributed to the house staff. The multifocal aspects of it ultimately resulted in a significant decrease in the mean LOS, although the difference (measured in hours) was not large enough to affect the total charges associated with hospitalization.
The reduction of inpatient charges associated with inpatient asthma protocols has been demonstrated in previous studies.1,4,16,17 However, achieving a statistically significant change in charges, based on the reduction in hours of LOS, should be balanced against the value of having more available bedspace for other patient admissions. More efficient bedspace turnover could be valuable as the state of Maryland converts to an all-payer model, in which hospitals will be allotted a set numbers of funds to use in a global budget.18,19 Hospital administrators may find the protocol beneficial in its approach to reduce the LOS while enhancing clinical efficiency. 13 Moreover, the reduction in 30-day readmission rates, although not achieving statistical significance, may also be beneficial as payors are modifying their reimbursement mechanisms for these encounters.20,21
Our study has several limitations, of which the most notable was the acute decline in protocol usage at ∼9 months postimplementation. A barrier we identified was that greater physician involvement in bronchodilator weaning appeared to be desired as a learning tool by junior residents transitioning to leadership roles corresponding to the time point of reduced utilization. To address this issue, RTs have since started notifying house staff immediately after determining whether the PAS warrants changing of bronchodilator frequency. House staff are now provided the option of evaluating the patient before any weaning of therapy. Before this effort, house staff were notified after weaning had occurred or when intensification was deemed necessary. Further efforts have since included monthly educational seminars and electronic communications, reminding house staff of the protocol's components and inclusion criteria. We have also continued to maintain real-time communication through electronic mail with stakeholders regarding potential enrollees and deviation/discontinuation of the protocol. Moreover, targeted education has also been implemented at individual and group levels among all newly employed RTs using an RT care clinical coordinator—a key point given routine staff turnover. A general review of these efforts, based primarily on stakeholder feedback, has noted improved usage and acceptability of the protocol.
Another limitation had been the inability to determine the effect of the protocol on patients initially admitted to the ICU and transferred to a non-ICU bedspace for further medical management. We had applied the protocol to patients transferred from the ICU who had met inclusion criteria; however, they were not included in our analyses. Our protocol was intended for the non-ICU setting; the higher acuity and varying clinical presentations in the ICU mandated different management strategies, which resulted in large inter-individual variation in LOS and charges to preclude its incorporation into the analyses. The value of the protocol may be enhanced in the future when viewed under a broader perspective that takes into account these higher acuity patients through the potential incorporation of this or a complementary protocol across hospital settings.
Further limitations include cost analyses that solely reflect inpatient charges from the healthcare payer perspective. The reduced LOS may have a greater impact when measuring direct (eg, caregivers' out-of-pocket expenses) or indirect cost savings (eg, improved work productivity). A modification of the study design may as well have bolstered the assessed value of the protocol, whereby the historical comparative group was replaced by a control group that received our standard inpatient asthma care—thus, yielding a randomized control for more potent analyses. We also did not have a baseline level of intensification events to compare with our protocol time period. Historical usage of bronchodilators during time points of intensification may have provided another outcome that could be used to gauge the protocol's value. The protocol may as well motivate caregivers to treat asthma exacerbations using β2-agonist therapy through an MDI+VHC, as opposed to nebulized treatment—an effect that is consistent with current clinical guidelines and best practice, but may have potential downstream effects on future costs. Future work will address organizational and clinical factors that will enhance implementation of the protocol more broadly within the framework of diverse stakeholders in varying hospital care environments.
Conclusion
Inpatient asthma protocols have been extensively documented to be beneficial in several healthcare institutions. The synchronous implementation of a multipronged approach using a quantitative scoring system, RT-lead bronchodilator weaning, and increased actuations of albuterol through MDI+VHC was successful in reducing the mean LOS. Although no significant change in inpatient charges was observed, the shortened hospitalization has possible implications for administrators seeking safe and efficient strategies to enhance available bedspace.
Footnotes
Acknowledgments
We would like to thank Drs. Janet Serwint, Michael Barone, Stacey Cooper, Lauren Cohee, Jamie Flerlage, Branden Engorn, Caleb Ward, and Kristen Johnson for their assistance in the design and implementation of the protocol.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.