
Abstract
The diagnosis of food allergy is challenging due to different immunologic mechanisms and diversity of symptoms. An open or double-blinded oral food challenge (OFC) was performed on 391 children (aged 0.2–16.9 years) with suspected cow's milk (n = 266) or wheat allergy (n = 125) to characterize immediate, delayed, and transient symptoms, and to evaluate the role of earlier food-related symptoms and immunoglobulin E (IgE)-mediated sensitization for the OFC outcome. The OFC resulted in an immediate positive reaction in 38% (n = 148) and a delayed positive reaction in 21% (n = 81) of the 391 children. Transient reactions, the majority of which were localized skin reactions, were seen in almost third (n = 50) of the patients with a negative OFC result (n = 162/391). Immediate localized skin reactions were more common during the milk challenge (p = 0.010), whereas immediate lower respiratory tract symptoms (p = 0.001) were more common during the wheat challenge. Although 14% (n = 21) of those with an immediate reaction received i.m. adrenalin as a treatment of the reaction, there were no life-threatening events. Multivariate analyses revealed that independent risk factors for the immediate OFC outcome were earlier moderate-to-severe immediate food-related reactions, marked IgE-mediated sensitization to the suspected food, and in case of wheat, age <12 months. The accuracy of OFCs can be enhanced without increasing the risk of serious allergic reactions by taking into account earlier food-related symptoms and the level of IgE-mediated sensitization, by refining our knowledge of transient non-specific reactions, and by applying standardized OFC protocols with over-one-day challenges.
Introduction
F
Suspicion of food allergy is commonly raised by the parents but much less frequently confirmed by a thoroughly controlled OFC.10,11 The reported frequency of symptoms during food challenges varies noticeably between studies, due to differences in patient age, sensitivity pattern, specific allergens used, and OFC protocols.5,12,13 There is still a great need for systematically collected prospective data on allergen- and organ-specific symptoms. 14 Clinical symptoms should be objective and/or: (1) severe, (2) reproducible, or (3) persisting. 15
In the patients' view, the key questions are: (1) Should a specific allergen be avoided or not? (2) If avoidance is necessary, how strict should the diet be? (3) What is the individual risk for immediate serious reactions? (4) What are the mild and transient symptoms indicating tolerance rather than allergy? Reduction of overdiagnosis is particularly important since unwarranted elimination of foodstuffs is not without risks, and strict diets might increase the probability of developing acute allergic reactions later in life. 16
By performing OFCs in 391 children with a suspicion of cow's milk or wheat allergy, we aimed at characterizing organ- and food-specific immediate, delayed, and transient reactions, and at evaluating the role of parentally reported earlier food-related reactions and the level of IgE-mediated sensitization with regard to the OFC outcome.
Materials and Methods
Study population
The study subjects included 391 consecutive children (aged 0.2–16.9 years, median 1.2 years) with a suspicion of cow's milk (n = 266) or wheat (n = 125) allergy who underwent an OFC in the pediatric unit of the tertiary hospital between September 2006 and April 2007. Earlier food-related symptoms were charted by a parental interview, and a physical examination was performed on the children. Any suspected symptoms and signs before, during, and after the OFC were recorded by using a structured form. Immediate reactions appearing during the OFC were classified as local/general (skin symptoms in particular), or subjective/objective, and grouped according to the severest symptom. 9 IgE-mediated sensitization to the suspected food was evaluated by SPTs and/or sIgE obtained in 12 months before the OFC.
Oral food challenges
For at least 1 week before the OFC, the suspected food product was eliminated from the diet of each child. During this period, parents kept a daily symptom diary. A successful elimination was followed by an open OFC that was performed in children with positive SPT results or a suspected immediate-type reaction; OFCs were performed as DBPCFC in children with negative SPT results or with a history of or suspected delayed-type reactions. 9 For the DBPCFCs, all the food products were prepared on site by the hospital kitchen staff who were not involved in the food challenge process. 17 In DBPCFCs, the suspected food product and placebo were given in a random order 2 weeks apart, including 1 wash-out week in between the challenges. 17
In both the open OFCs and DBPCFCs, food was administered in gradually increasing amounts until unequivocal objective adverse reactions occurred. To consider a challenge result positive, the occurring adverse reaction should be worsening, repeated, or persistent by increasing doses of suspected food, in both the open OFCs and DBPCFCs. 9 In case of milk, the first dose was 1 drop applied onto mucosa of the inner side of the lower lip. Thereafter, 2, 10, 50, and 100 mL formula or with children above 1 year of age, raw milk was given at 30 min intervals. 18 The first dose of wheat was 1 drop of wheat in NaCl solution applied onto the mucosa of the inner side of the lower lip. Thereafter, 1, 5, and 10 g of wheat were given at 1-h intervals. 17 Positive reactions that occurred within 2 h after the last dose were classified as immediate reactions. If there were no reactions in the outpatient clinic, the OFC was continued at home with at least 400 mL of milk (or equivalent dairy products), or 20 g of wheat, each day for 7 days. As during the elimination period, also during the home challenge the parents kept a daily symptom diary.
The exact time, nature, and the eliciting dose of each observed adverse reaction were recorded. It was predetermined that in case of doubtful reactions, the challenge was to be continued until there were obvious objective signs of positive reactions. Transient symptoms appearing during the challenge were also recorded.
SPT and serum sIgE
Data on SPTs to suspected foods were available for 322 (82%) of the 391 children. SPTs were carried out on the volar aspect of the forearm with a positive control (histamine hydrochloride 10 mg/mL; ALK-Abello), a negative control (buffer solution; ALK-Abello), cow's milk formula, wheat flour dissolved in NaCl solution (1:10), and gliadin (1 mg/mL). The SPTs were read after 15 min. The wheal's longest and shortest perpendicular axis was measured, and the results were expressed as the mean wheal diameter in millimeters. Reactions with a mean wheal diameter of 3 mm or larger were considered positive.
Data on sIgE to suspected foods were available for 98 (25%) of the 391 children. Serum samples were analyzed with ImmunoCAP® (Phadia AB, Uppsala, Sweden) for sIgE to milk or wheat. Samples with an sIgE antibody concentration above or below the measuring range (0.1–100 kUA/L) were diluted and reanalyzed to obtain the exact concentration. Values of 0.35 kUA/L or greater were regarded as positive.
Statistics
To evaluate the statistical differences between the groups, χ2-test or Fisher's exact test (if the expected frequency for any cell was <5) was used for dichotomous variables, and Mann–Whitney U test or Kruskal–Wallis test was used to analyze continuous or ordinal variables. Correlations between continuous and ordinal variables were determined by Spearman's rank correlation test. Predictive values (PVs), sensitivity, specificity, and likelihood ratios for positive test results (LR+) were calculated by using routine equations. An LR+ of ≥5 is considered to have at least a moderate increase in the likelihood of the disease, and an LR+ of ≤0.2 is considered to have at least a moderate decrease in the likelihood of the disease. The receiver operating characteristic (ROC) curves were applied to determine an optimal SPT wheal size and an optimal sIgE concentration to differentiate children with immediate positive reactions from those with the negative OFC. Two-tailed tests were used in all analyses. p Values less than 0.05 were considered statistically significant. SPSS 22.0 (SPSS, Inc., Chicago, IL) statistical software was used for statistical analysis.
Ethical considerations
The study was approved by the research ethics committee of the regional university hospital, and it was carried out in accordance with the principles embodied in the Declaration of Helsinki of 1965 (as revised in Brazil 2013). Parents of the study children gave informed consent, and patient anonymity was preserved by using methods approved by the ethics committee.
Results
Table 1 presents the results of the 391 OFCs performed. The OFC resulted in an immediate positive reaction in 38% of the children, and a delayed positive reaction in 21% of the children. Transient reactions—the majority of which were localized skin reactions—were seen in almost third (31%) of the patients, with a negative OFC result (Table 1). Immediate localized skin reactions were more prevalent in milk challenges, whereas lower respiratory tract symptoms were more frequent in wheat challenges (Table 1). Immediate reactions were observed already after the first dose in 12% (n = 31/266) of the milk challenges, and in 5% (n = 6/125) of the wheat challenges (p = 0.031). The median dose that elicited an immediate reaction was 6 mL for milk and 6 mg for wheat. For milk challenges with immediate reactions, there was a negative correlation between the symptom-eliciting dose and the SPT wheal size (r = −0.501, p < 0.001). Such a correlation was not seen for wheat challenges (r = −0.067, p = 0.719). All delayed objective symptoms appeared within the first 4 days from the beginning of the challenge, and none had a first objective symptom later. Open OFCs were regarded more often positive (in 63%) than DBPCFCs (in 43%) (p = 0.001).
Milk challenged versus wheat challenged.
Localized erythema and/or urticaria.
Oral pruritus, itchy throat, or abdominal pain, with or without localized skin involvement.
Generalized erythema and/or urticaria.
Vomiting and/or diarrhea with or without skin involvement.
With skin and/or GI involvement.
Eczema.
Vomiting, diarrhea, and/or abdominal pain.
Nausea and/or abdominal pain.
GI, gastrointestinal.
In case of an immediate positive OFC reaction, the main line of treatment included oral antihistamines (85%; n = 126/148), whereas oral prednisolone was administered rarely (5%; n = 8/148). The need for intramuscular adrenalin was higher during wheat challenges (24%; n = 10/42) as opposed to milk challenges (10%; n = 11/106) (p = 0.035). No life-threatening events were seen.
The baseline data of children with an immediate positive OFC reaction differed significantly from those with a negative OFC result with regard to age, the type of a parentally reported earlier food-related reaction, and positive SPT or sIgE results (Table 2). In contrast, those with a delayed OFC reaction differed from those with a negative OFC result only with regard to earlier delayed skin reactions, which were more frequent in children with a negative OFC result (p = 0.027). The children who underwent a milk challenge were younger (median 1.0 years of age) than those who underwent a wheat challenge (median 1.4 years) (p < 0.001). In addition, earlier food-related reactions were more often reported as immediate in those with a suspicion of milk allergy (41%; n = 108/266) than in those with a suspicion of wheat allergy (28%; n = 35/125) (p = 0.016). There were no differences in SPT or sIgE positivity between the children with a suspicion of milk allergy and those with a suspicion of wheat allergy.
The values are presented as median (range) or n (%).
Classified according to the severest symptom. Mild: erythema, abdominal pain; Moderate: urticaria-angioedema, vomiting, diarrhea; Severe: anaphylaxis, need for adrenalin.
Eczema.
Vomiting, diarrhea, and/or abdominal pain.
A wheal with a diameter of ≥3 mm against the tested allergen, or sIgE of ≥0.35 kU/L.
LR+, positive likelihood ratio; PV, predictive value; sIgE, allergen-specific immunoglobulin E; SPT, skin prick test.
Although children with an immediate positive OFC reaction differed from those with a negative OFC result in several baseline characteristics, in most cases, LR+ values showed either no or not more than a small increase (LR+ <5) in the likelihood of an immediate reaction in the OFC (Table 2). Only earlier anaphylaxis or a need for adrenalin during an earlier food-related reaction had a significant increase in the likelihood of an immediate reaction in the OFC (LR +13.5) with a PV of 92%. However, the sensitivity of such an earlier reaction on the immediate outcome was only 8% (Table 2). Moreover, among those 13 subjects with earlier severe food-related reactions, there were only 2 children who received i.m. adrenalin as a treatment for the immediate reaction during the OFC: 1 patient because of angioedema, facial urticaria, and vomiting after the third dose of milk, and another patient because of generalized urticaria and vomiting after the second dose of wheat. The milk-challenged patient did not get any symptoms before the dose after which he needed adrenalin, but the wheat-challenged patient was recorded to have an urticarial lesion in the inner side of the lower lip after the first dose of wheat; however, as there was no worsening of the symptoms, the OFC was continued and stopped only after the second dose.
On the other hand, combining earlier severe reactions with less severe but objective immediate skin (ie, urticaria-angioedema) or GI (ie, vomiting, diarrhea) symptoms yielded an LR+ of 4.6 with a PV of 72% and sensitization of 56%. Earlier delayed GI symptoms rarely associated with an immediate OFC reaction (Table 2). None of the baseline characteristics were associated with an increase or a decrease in the likelihood of a delayed OFC reaction (Table 2).
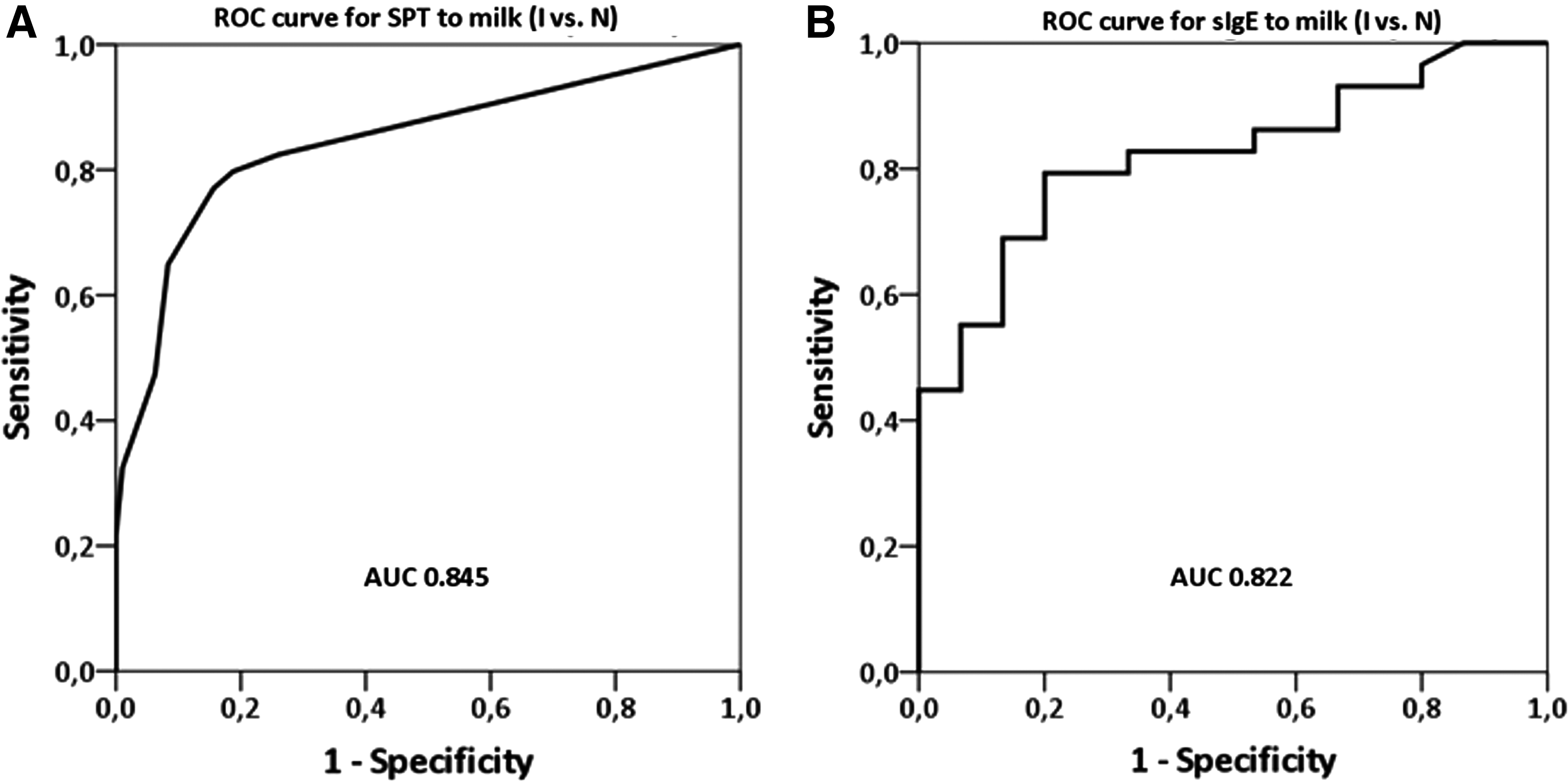
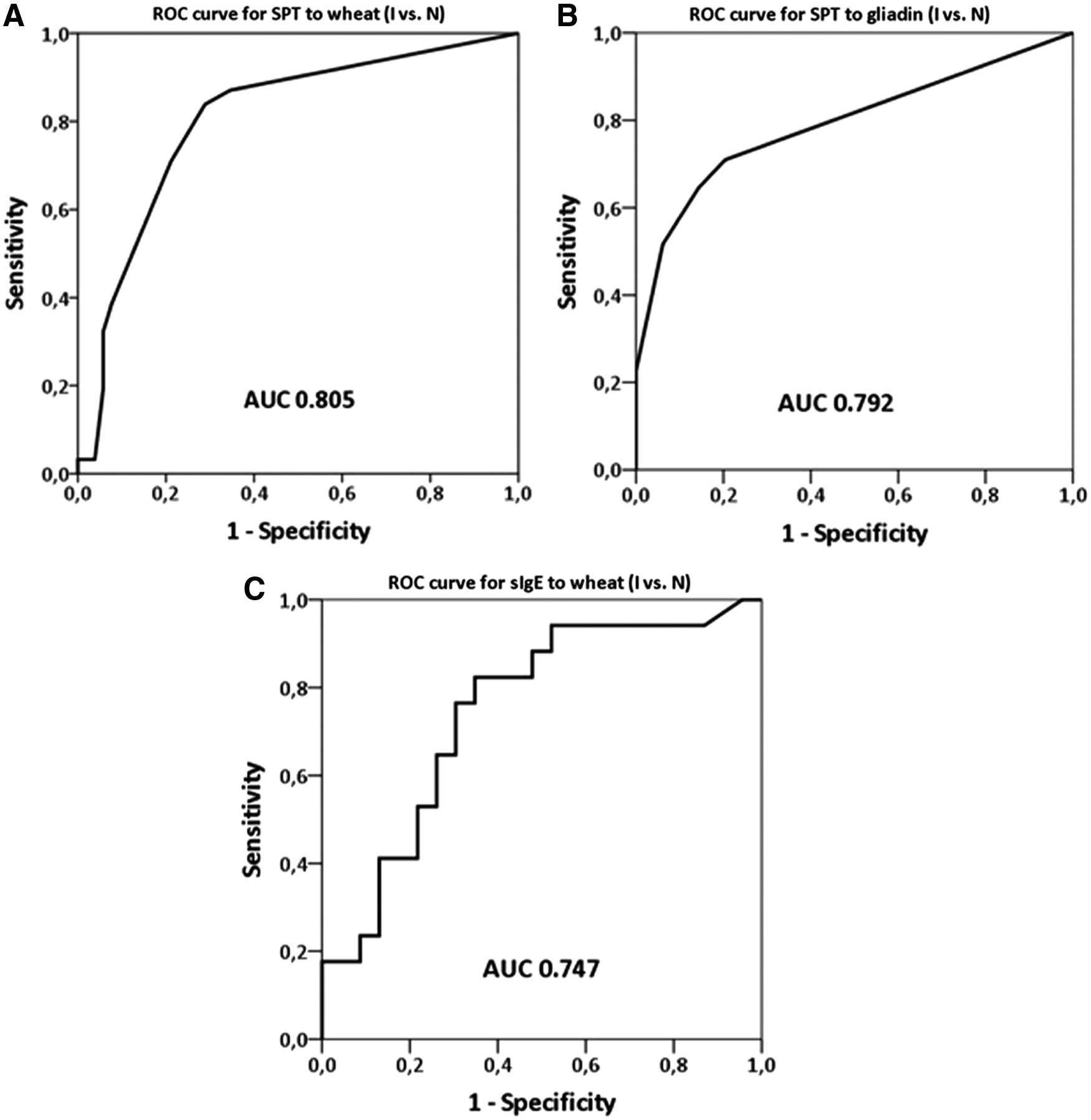
ROC analyses were performed to find optimal cut-offs for SPT and sIgE results (Figs. 1 and 2) with regard to the OFC outcome. ROC curves revealed that an SPT wheal of ≥6 mm and an sIgE level of ≥5 kU/L to milk, as well as an SPT wheal of ≥6 mm to wheat, or ≥5 mm to gliadin, yielded LR+ values of ≥5, increasing at least moderately the risk for the immediate OFC reaction compared with the negative OFC result. With regard to sIgE to wheat, no such cut-off level was found: LR+ remained low, maximum 2.5, for the sIgE level of ≥7.0 kUA/L, with a sensitivity of 65% and a specificity of 74%.
ROC curves for
ROC curves for
When combining SPT and sIgE results, an SPT wheal of ≥6 mm and/or an sIgE level of ≥5 kU/L to milk gave an LR+ of 6.9, with a PV of 79% and a sensitivity of 64% for an immediate milk challenge outcome compared with the negative OFC result. When combining SPT results to wheat and gliadin, an SPT wheal of ≥6 mm to wheat and/or ≥5 mm to gliadin gave an LR+ of 5.4, with a PV of 61% and a sensitivity of 55% for an immediate wheat challenge outcome compared with the negative OFC result.
Age-adjusted multivariate logistic regression analyses were performed to find out independent risk factors for an immediate OFC reaction (Table 3). As a result, it was found that earlier moderate-to-severe immediate food-related reactions, and aforementioned levels of IgE-mediated sensitization were independent risk factors for the immediate positive reactions in milk challenges. Earlier moderate-to-severe immediate food-related reactions to foods, age less than 12 months, and aforementioned marked SPT reactivity to wheat or gliadin were found to play a role as independent risk factors for an immediate OFC reaction to wheat.
Results of age-adjusted multivariate logistic regression analyses. Analyses were performed as immediate versus delayed positive or negative oral food challenge results.
n = 226; Nagelkerke R2 0.475.
n = 104; Nagelkerke R2 0.299.
Urticaria-angioedema, vomiting and/or diarrhea, or anaphylaxis/need for adrenalin.
CI, confidence interval; OR, odds ratio.
Discussion
By performing OFCs in almost 400 children with a suspicion of cow's milk or wheat allergy, we were able to show that the OFC outcome can be predicted at least on a certain level by the history of food-related reactions, IgE-mediated sensitization, and the age of the patient. Transient reactions, that is, erythema not progressing to urticaria-angioedema, and subjective abdominal symptoms were surprisingly common, seen in almost third of the OFCs with a negative result. Although the frequency of transient reactions probably varies between populations, there is a considerable risk for food allergy overdiagnosis if the OFC is stopped and annotated as positive on mild symptoms.
During infancy, when new nutrients are introduced in the diet, insignificant sensitization to food antigens may cause transient non-specific symptoms. However, in ∼8% of children, 19 the development of tolerance fails, resulting in food allergy. On the other hand, there are several non-allergic conditions producing similar symptoms 2 but often suspected as allergic by parents. 10
SPTs and sIgE-measurements are commonly available methods for detecting IgE-mediated sensitization, but they are not sufficient for food allergy diagnostics per se, as the recommended levels for significant predictive results vary by age and are food specific. 2 According to the national guidelines of our country, the diagnosis of food allergy to cow's milk, wheat, or hen's egg should be established by OFC, irrespective of the allergen-specific IgE level or SPT results. However, in children with a reliable history of anaphylaxis to a food item, caution should be taken when performing OFCs, and under such circumstances, follow-up of sIgE in search of decreasing values could be a useful tool for assessment of optimal timing for the OFC. Spontaneous development of tolerance is seen in the majority of milk and wheat allergic children by school age,12,13,20 and, thus, earlier reactivity to foods is likely to alleviate by time. However, despite the development of clinical tolerance, IgE-mediated sensitization might be seen for years on. On an individual level, the present data showed how erratic the food allergy diagnosis is, if based merely on SPT or sIgE positivity. There are children with an SPT wheal of 10 mm in diameter, or an sIgE of >50 kUA/L to wheat but with a negative result in the wheat challenge. In addition, a negative test result does not guarantee clinical tolerance 2 that was, in particular, seen in the youngest children also in our OFC material. Therefore, OFCs as open or as DBPCFCs are regarded as a gold standard for food allergy diagnosis.
We used OFC protocols that are in line with the protocols widely applied in our country. Since the proportion of immediate reactions with the first dose and the incidence of serious reactions were not prominently high, our allergen doses appeared to be within acceptable limits. In fact, as the reactions with the first dose, that is, 1 drop of the allergen solution applied onto the mucosa of the inner side of the lower lip, were relatively rare, such a small amount of allergen solution was omitted from the further OFC protocols used in our hospital. In the present study, adrenalin was given in an early phase of a generalized allergic reaction to avoid further complications. Hence, not all reactions treated with adrenalin can be classified as anaphylaxis. However, by scoring the challenge outcome, 9 the use of adrenalin can often be avoided if early reactions are recognized and OCF is stopped before proceeding to a higher dose of food. There were significantly more positive results with open challenge compared with DBPCFC. In our opinion, this does not directly indicate the inferiority of the other but rather reflects the fact that DBPCFC were performed only in those with suspected delayed or equivocal symptoms and with more often IgE-negative status.
Because of the possibility for falsely negative results, the initially negative challenges were continued for 7 consecutive days. Only persistent and worsening symptoms recorded in the diary were considered as a positive OFC result. According to our results, there is a considerable risk for falsely negative results by single-day challenges. Children who do not react during the first challenge day may be at risk of unanticipated allergic reactions at home, or the underlying reason for exacerbation of atopic dermatitis or gastric complaints will be undetected. The reason for this delayed reactivity probably reflects other mechanisms besides type I IgE-mediated reaction, particularly in food-induced GI allergies. 21 The ideal duration and cumulative doses of OFC remain to be defined but according to our data, the duration of OFC with a maximum of 5 days could be optimal.
The nature and severity of symptoms, the minimum eliciting dose, and the associations with sIgE levels or SPT positivity are allergen specific, as seen in many studies.19,22 In the present study, more wheat-related immediate lower respiratory tract symptoms were seen, whereas immediate localized skin reactions were more common during milk challenges. The reasons for these allergen-specific properties are yet to be discovered. In a recent report of organ-specific symptoms, the allergen-specific differences were distinct from our study. 14 In another study, in accordance with ours, there were more severe reactions during wheat challenges compared with milk. 5 We observed delayed atopic eczema as an independent symptom in only one fifth of the children compared with much higher rates in studies with only open OFCs. 23 These discrepancies are largely attributable to differences in the patient population, challenge protocols, and symptom classifications.
The likelihood of an immediate positive OFC result increased with the increasing SPT wheal size and sIgE levels to milk. However, only modest sensitivity and specificity of SPT and sIgE to wheat was observed. Interestingly, SPT for milk correlated with the allergen dose and objective symptoms. For wheat, such a relationship could not be observed, making wheat even a more unpredictable allergen. However, wheat-allergy diagnosis might be improved by including component testing into the diagnostics, as recently suggested. 17
Our study has several limitations that need to be addressed. Although data on symptoms before and during the OFC were collected prospectively, laboratory data on allergic sensitization were assessed retrospectively, resulting in some missing information. Not all challenges were performed as DBPCFCs, however those with earlier delayed reactions were, to minimize confounding factors. 6 Interpretation and classification of observed reactions during OFCs can be influenced by subjective factors. However, more than 95% of the challenges were supervised and symptoms of OFCs were recorded by the same study physician, being one of the authors.
The diagnosis of food allergy cannot be based merely on a parental report of symptoms, as there is a significant level of overdiagnosis of food allergy even by physicians. 11 The lack of standardized and controlled diagnostic workout will ultimately lead to unnecessary avoidance diets. On the other hand, without OFCs, the underlying nature of food-related reactions might not be recognized, increasing the risk of severe reactions with accidental exposures. Preferably, all OFCs should be performed as DBPCFC, but in practice that is not always possible. For that reason, children with earlier immediate moderate-to-severe objective symptoms, and usually evidence of IgE-mediated sensitization for the offensive food could be challenged openly, and those with delayed or unclear symptoms should be challenged by using the DBPCFC protocol (Fig. 3).

Algorithm for choosing oral food challenge method. IgE+, IgE mediated; IgE−, non-IgE mediated.
In conclusion, it is possible to enhance the accuracy of OFCs without increasing the risk of serious allergic reactions by (1) taking into account earlier parentally reported symptoms of food ingestion; (2) refining our knowledge of transient non-specific reactions; (3) considering the level of allergen-specific sensitization; and (4) in case of suspected delayed reactions, using DBPCFC protocols with over-one-day challenges.
Footnotes
Acknowledgments
The authors thank the registered nurse Tuija Rito for her skilful data management, the children themselves, and their parents. They also acknowledge support from Helsinki University Central Hospital Research Funds, Sigrid Jusélius Foundation, and Foundation for Pediatric Research.
Author Disclosure Statement
No competing financial interests exist.