
Abstract
Hypersensitivity pneumonitis (HP) is an inflammatory lung disease triggered by environmental antigens. The antigens can come from bacterial, fungal, animal, or chemical sources. This case report discusses an 11-year-old male patient with a chief complaint of persistent cough for more than one month that was suspected to be pneumonia. The patient was ultimately diagnosed and treated for HP caused by exposure to pigeon allergens.
Introduction
H
Case Description
We present a case of an 11-year-old boy admitted to our Paediatric and Allergology Department with a persistent, paroxysmal cough unsuccessfully treated with a macrolide antibiotic (clarithromycin) on an outpatient basis for 10 days. The boy had no previous history of chronic disease. A negative family history of atopic diseases was elicited.
On admission, the boy was in very good general condition. Physical examination revealed congested pharyngeal mucous membranes, loud vesicular sounds above the lung fields, numerous bilateral fine crackles, and single wheezes; no other abnormalities were detected.
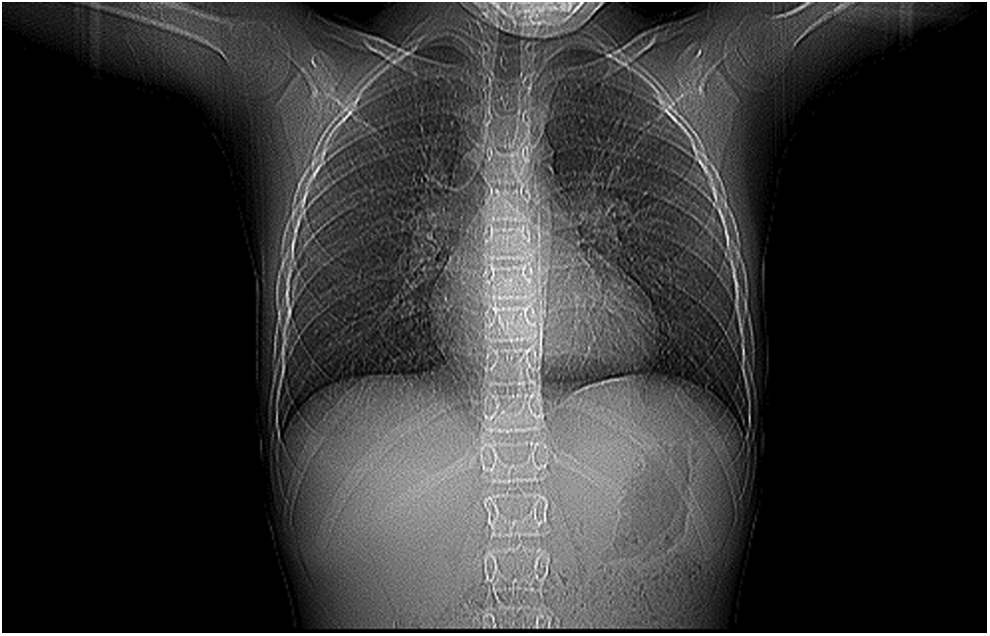
Results of investigations indicated elevated total IgE concentration at 309.9 IU/mL (normal limit <200), presence of IgE specific for cat fur allergens (Class 4), grass pollens: common meadow grass (Poa pratensis) and cock's foot (Dactylis glomerata) (Class 2), mugwort (Artemisia vulgaris) pollen (Class 1), and dog fur (Class 1). The presence of atypical bacteria antibodies was determined: Mycoplasma pneumoniae, Chlamydia pneumoniae, and Bordetella pertussis in IgA and IgM classes—within normal limits. A chest X-ray revealed bad aeration and numerous merging densities of the lungs upon inflammatory parenchymal–interstitial lesions with atypical changes in the hilar. Based on the history taking, physical examination, and results of investigations, the patient was diagnosed with bilateral interstitial pneumonia, polysensitization, and allergic rhinitis. Antibiotic therapy (clindamycin and ceftazidime), budesonide, and fenoterol with ipratropium nebulization, hydrating intravenous infusions, and kinesiotherapy were applied, resulting in a gradual improvement in the patient's health and resolution of signs. The boy was discharged home in a good general condition after an 8-day hospitalization, with recommendation to continue antibiotic therapy (cefuroxime for 5 days) and take antihistamines, antileukotrienes, and inhaled glucocorticosteroids.
Fourteen days after the end of hospitalization, the boy presented to the department with persistent coughing and shortness of breath on exertion. On admission, the boy was in very good general condition. Physical examination revealed loud vesicular sounds over the lung fields and numerous crepitations heard bilaterally at the lung bases; no other abnormalities were detected.
Chest high-resolution computed tomography was performed (Figs. 1 and 2). Investigation indicated ill-defined interlobular nodules in both the lungs, merging into diffuse density areas of the ground glass opacity type involving the whole lung parenchyma with partial saving of peripheral/subpleural portions. Carinal lymph nodes of up to 11 mm in size in the mediastinum and the thymus in the anterior mediastinum were revealed. These findings were suggestive of HP.
HRCT of the chest showing ground glass opacities in the middle and lower lung zones. This type of HRCT pattern is most frequently found in the patients with subacute HP. HP, hypersensitivity pneumonitis; HRCT, high-resolution computerized tomogram.

HRCT of the chest showing ill-defined centrilobular nodules of up to 11 mm in size in the mediastinum and the thymus in the anterior mediastinum.
On repeat history taking, it was discovered that the child had experienced gradually decreasing endurance over the past 1.5 years. In addition, several dozen years ago, the boy's grandfather had bred 400 pigeons in the attic of the house where the boy lived.
To extend the diagnostic procedure, the boy was referred to the Department of Pneumonology and Cystic Fibrosis of the Institute of Tuberculosis and Lung Disorders in Rabka. Investigations performed there revealed an elevated level of specific IgG class antibodies for pigeon and parakeet antigens, and oxygen desaturation (from 97% to 89%) in a 6-min walk test (6MWT). Bronchoscopy did not show lesions in the bronchial tree. Bronchoalveolar lavage (BAL) indicated reduced level of macrophages (57%) and increased percentages of neutrophils (31%) and eosinophils (6%) with 6% of lymphocytes. Pulmonary function testing was attempted during his early evaluation, but was unsuccessful because of his inability to perform acceptable spirometric maneuvers. Based on the investigation results, the final diagnosis of EAA was made. The patient was commenced on systemic corticosteroids (methylprednisolone 2 mg/kg·day up to a maximum of 60 mg/day), with very quick improvement in exercise capacity and reduction in the number of auscultatory changes. After 10 days of corticosteroid therapy, there was no desaturation in 6MWT (97% at the beginning and 96% at the end). Steroids were continued at high dose during 1 month, and then tapered slowly over the subsequent 5 months.
In addition, the boy's parents carried out an extensive renovation of the attic of the house where pigeons had been bred, with the boy living in a different place during the renovation.
This resulted in a continuing gradual improvement, leading to normalization of exercise capacity and of auscultatory changes. The level of specific IgG class antibodies for pigeon and parakeet antigens gradually decreased (Table 1). No radiology control after treatment was performed yet.
The boy was cared for by the Allergology Outpatients Clinic and periodical investigations were performed in the Department of Pneumonology and Cystic Fibrosis. On subsequent visits, the boy's condition systematically improved and auscultatory changes resolved. The boy learned to perform lung function tests, which were conducted on each visit (at monthly intervals, Table 2 and Fig. 3) that also indicated the boy's improved clinical condition.
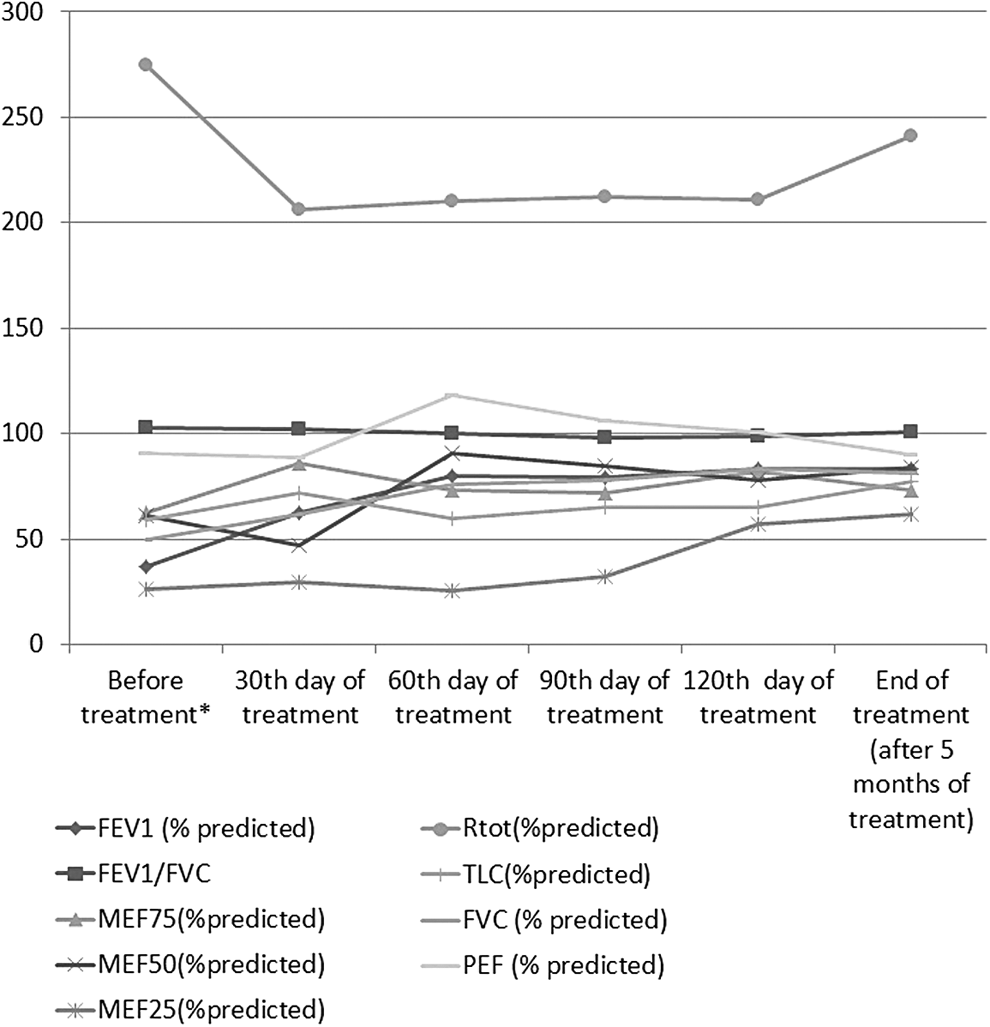
Changes in spirometric values after treatment with systemic corticosteroids (*).
FEV1, volume that has been exhaled at the end of the first second of forced expiration; FVC, forced vital capacity; MEF, maximal expiratory flow; PEF, peak expiratory flow; Rtot, total resistance of the airways; TLC, total lung capacity.
Discussion
Pigeon breeder's lung is one of the most common forms of HP and is responsible for about 80% of all cases worldwide. In other areas, other causes (such as exposures leading to “farmer's lung”) may be as or more prominent. HP is a disease caused by immune reaction to environmental antigens. It is also believed that heredity may play an important role, with families positive for HLA-DR7, HLA-B8, and HLA-DQw3 showing a stronger predisposition. 3 The physical examination typically reveals crackles over lower lung fields. Precipitating antibodies against specific antigens are present in some patients, but their detection is not a prerequisite for diagnosis. Patchy and nodular opacities are found on plain chest X-ray, and high-resolution computed tomography shows centrilobular nodules, diffuse ground glass opacities, and fibrosis. Pulmonary function tests reveal restriction, reduced lung diffusion capacity, and exertional hypoxemia. HP is uncommon in childhood, and very few data regarding frequency, treatment, and outcome exist for children.4 In Denmark, the incidence and point prevalence of HP were 2/year and 4/1,000,000 children. 4
We present a child with HP who was initially misdiagnosed as having allergic disease. The correct diagnosis was made based on history taking (exposure to allergens of pigeons), physical examination, radiological investigations, and the presence of specific precipitins in serum. The diagnosis was delayed because of other symptoms because of unexpectedly long history of exposure dating back many years before symptoms appeared. Typical flu-like symptoms (fever, chills, dry cough, dyspnea, and bone and muscle pain) were not present. However, progressive dyspnea and exercise intolerance in his chronic stage were present. Also, the patient did not have the typical BAL lymphocytosis seen in this disease (usually more than 50% of lymphocytes). However, lower lymphocytosis in HP can be seen in chronic stages of the disease. After taking a thorough history, exposure to pigeon allergens was elicited. The clinical symptoms of the patient could be explained by a more intense and prolonged exposition to allergen. It should be noted that late diagnosis in up to a quarter of the children with HP has been reported. 5
Laboratory tests of our patient indicated the presence of specific precipitins in serum, blood precipitins were strongly positive for pigeon and parakeet. Furthermore, leukocytosis and increased concentrations of IgG and IgM class immunoglobulins were found.
Treatment included total and definitive allergen avoidance and systemic corticosteroid therapy.
In this case, the overall condition of the patient and results of lung function tests improved after applying the already mentioned treatment methods. Clinical improvement began with avoidance of exposure, as previously described. 6 Long-term prognosis in children with HP appears favorable although persistent peripheral airway involvement of unknown clinical significance was demonstrated. 7
In conclusion, children with chronic cough should be suspected with HP if they present progressive dyspnea and/or exercise intolerance.
Footnotes
Acknowledgments
We obtained written permission from the parents for the publication of this case history. This study is self-funded.
Author Disclosure Statement
No competing financial interests exist.