
Abstract
The prevalence of pediatric food allergies has increased in children by 50% from 1997 to 2011, affecting 1 in 13 children in the United States. Food allergies can have short- and long-term emotional and physical consequences, which may result in challenges for both children and caregivers. Currently, to our knowledge, there are no low-cost, easily available, evidence-based psychosocial resources for children with food allergies and their families. The Cellie Coping Kit for Food Allergies was created to address this need. This study examined the acceptability and feasibility of the Cellie Coping Kit as an intervention and explored the learning outcomes associated with the kit. Twenty-five children (between ages 7 and 13 with 1 or more food allergies) and their caregivers were recruited from an outpatient clinic while participating in an oral food challenge. Children and caregivers were introduced to the Cellie Coping Kit following their food challenge. Four weeks later, follow-up assessments were completed to evaluate participants' impressions of the intervention. The results suggest that children and caregivers found the Cellie Coping Kit acceptable and feasible. Most (80%–100%) participants thought the intervention materials were trustworthy, found the kit easy to use, liked the appearance of the kit, and would recommend the intervention to others. Approximately 65% of children and 60% of caregivers reported learning from the Cellie Coping Kit. The Cellie Coping Kit for Children with Food Allergies was generally well received by children with food allergies and their families. The Cellie Coping Kit can be used to help facilitate dialog between children and caregivers about food allergy-related issues. While results are promising, additional research (especially in younger children and those newly diagnosed) is needed to determine if the intervention is achieving targeted goals (ie, coping behaviors and improved adherence to medical recommendations).
Introduction
P
Pediatric food allergies are also challenging for the family. Caregivers are faced with numerous allergy-related tasks every day, such as reading and rereading food labels to avoid allergens, 15 monitoring the food their child ingests,16,17 advocating for their child (eg, educating school staff and other parents),16,17 ensuring that their child receives nutrition without consuming their allergen, 16 and communicating with restaurants to review allergen-free food options. 16 Mothers of food allergic children also report fears following their child's diagnosis of a food allergy with concerns about life-threatening reactions continuing over time. 18 Caregivers of food allergic children report a lower quality of life than caregivers of children without food allergies. 15
While psychosocial resources are limited for children with food allergies and their families, some children and their caregivers have access to educational resources. For example, parents may use online resources that provide allergen-free recipes, information specific to a new diagnosis of food allergies, advocacy information, and ways to connect to other families (eg, www.kidswithfoodallergies.org; www.foodallergy.org; www.myallergykingdom.com). Educational materials include games such as www.foodallergykidsspot.com and books (eg, Alfie the Allergic Alligator goes to School, 19 The Bugabees: Friends with Food Allergies, 20 Living confidently with Food Allergy—A guide for parents and families 21 ). New applications for smartphones or tablets have been developed, but most are currently considered of poor quality due to the type of information that they provide and/or problematic functionality. 22 Some children with food allergies and their parents may have access to support groups (either through social media or in-person weekly sessions). 23 While many of these resources may be helpful to families, to our knowledge, there are no easily accessible, evidence-based psychosocial resources that target the large range of physical and psychosocial stressors associated with pediatric food allergies.
The increased prevalence of pediatric food allergies, combined with the limited number of evidence-based psychosocial resources available to children and families, suggests a need for novel interventions. Low-cost interventions designed for family self-implementation may be able to help minimize the impact of food allergies. We created the Cellie Coping Kit for Children with Food Allergies as a tool to help address this need. Initially, the Cellie Coping Kit intervention was created for children with cancer. 24 The intervention kit consists of a toy (eg, Cellie) to promote engagement of the coping kit, food allergy coping cards (containing developmentally appropriate evidence-based techniques to help children with food allergies), and a caregiver's book (mirroring the tips on the coping cards). To ensure the Cellie Coping Kit for Children with Food Allergies is an evidence-based tool, we first conducted a thorough literature review to select what aspects of pediatric food allergy are most difficult for families and what research-based coping strategies are most effective in helping manage these types of stressors. We then infused this information into the Cellie Kit prototype before expert review of intervention content. The intervention content includes sections on communication, medical care, oral food challenges/testing, anaphylaxis, school and friends, emotional reactions, and additional resources for caregivers. See the Materials and Methods section for a more detailed description of how the Cellie intervention was developed. The primary aims of the current study were to examine acceptability and feasibility of the Cellie Coping Kit as an intervention for children with food allergies. Additionally, the study explored learning outcomes associated with the Cellie Coping Kit intervention.
Materials and Methods
Participants
Children were eligible to participate if they were between the ages of 7 and 13, had 1 or more IgE-mediated food allergies that required food avoidance and an anaphylaxis plan, had sufficient English language skills, and the cognitive ability to participate in the intervention and complete assessments. A total of 33 children and their caregivers (parents/legal guardians) were offered an opportunity to participate in the study: 25 children (14 males, 11 females) and 1 caregiver per child (22 females) were enrolled (78% participation rate). Follow-up assessments were completed by 20 children and 21 caregivers (80% follow-up rate). The Hospital's Institutional Review Board approved all study procedures.
Procedure
Participants were recruited during a food challenge (referred by an outpatient clinic). Research assistants approached families who met eligibility criteria and explained the study. After written consent and assent were obtained, children and parents were introduced to the Cellie Coping Kit for Food Allergies intervention. Research assistants asked families to identify allergy-related challenges, and then reviewed the intervention materials specific to the child's needs. For example, if a child reported that he or she felt isolated at school, the child and parent were directed to the section of the kit that provided coping tips about school and friends (eg, ask your parents to bring the class a snack that is allergen free; take part in other fun things at the class party besides eating). See below for a more detailed description of the intervention. Follow-up assessments were completed 4 weeks later through the phone. During the follow-up assessments, children and parents independently completed a semistructured interview and satisfaction questionnaire 24 reporting on use of the Cellie Coping Kit during the past 4 weeks.
Description of the Cellie Coping Kit intervention
The Cellie Coping Kit is an evidence-based intervention designed to be implemented by children and caregivers. The kit content was developed by reviewing past research, obtaining informal input from families of children with food allergies, and integrating recommendations from food allergy experts (eg, physicians, nurses, nurse practitioners, psychologists, social workers). In creating this intervention, the content was targeted for school-aged children. School-aged children demonstrate improved reasoning and conceptual thinking skills, 25 allowing a greater capacity to reflect on the consequences of food allergy. Growing vocabulary, syntax, and verbal fluency enable school-aged children to more effectively utilize language to communicate their thoughts, feelings, and experiences to their social supports. 26 The skills required to implement the Cellie intervention are those reasoning and language skills that have been developed by middle childhood. Thus, by middle childhood, most children should be able to identify challenges of food allergies and work with their parents to learn how to deal with these challenges.
The Cellie Coping Kit includes a stuffed toy (Cellie), coping cards, a caregiver's guide, and a drawstring bag for easy transportation (eg, to school, friend's house). The stuffed toy (Cellie) is integrated into many of the coping strategies (eg, practice using your trainer epinephrine autoinjector on Cellie). Each of the 42 coping cards has a picture of Cellie on the front, followed by a stressor and several coping tips on the back (eg, strategies for eating outside of the home). See Figure 1 for sample coping card. The caregivers' guide corresponds to the coping cards and has tips and additional resources for caring for a child with food allergies (eg, grocery shopping). See Figure 2 for sample caregivers' guide content.
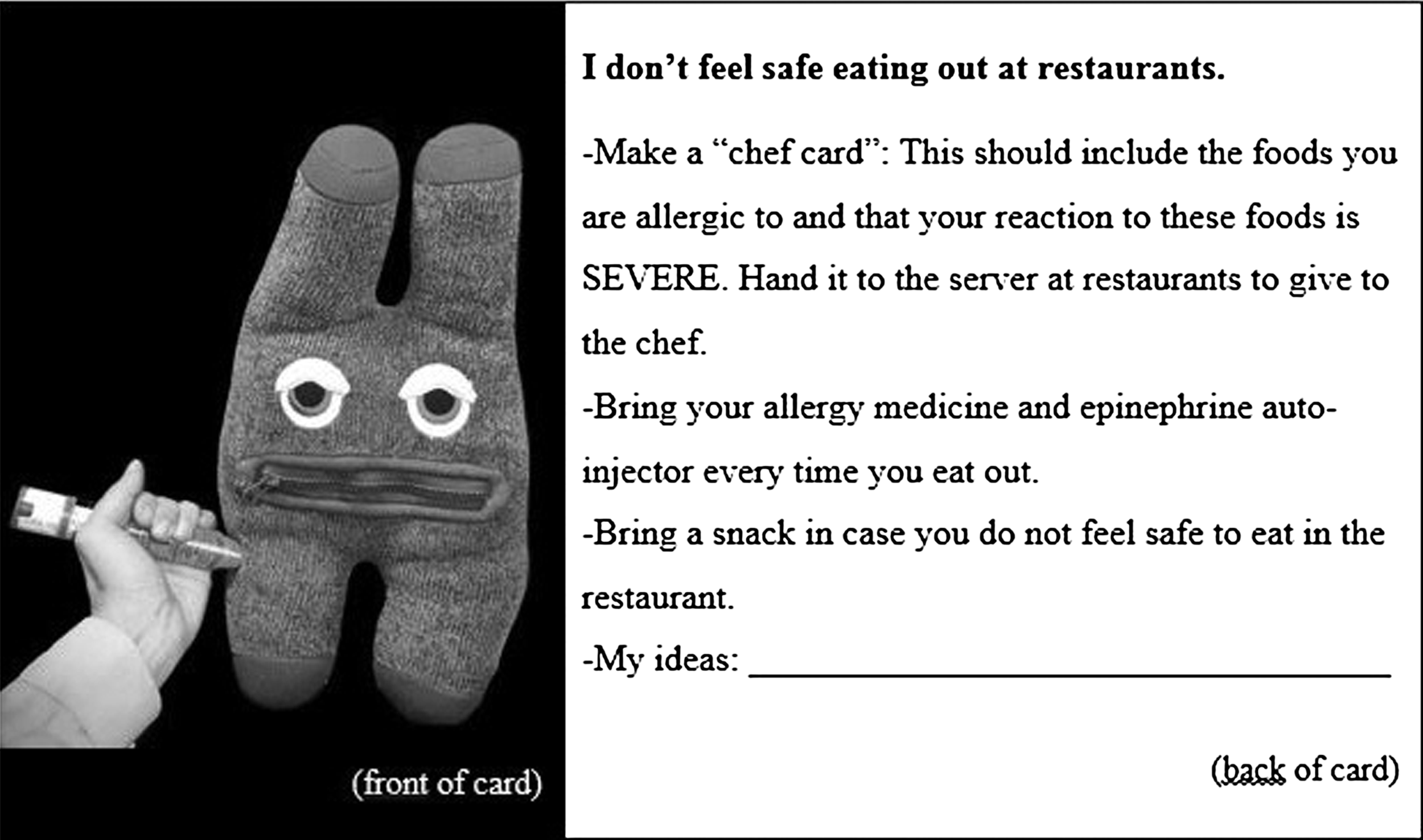
Sample Cellie Coping Kit coping card.

Sample content from the Cellie Coping Kit Caregiver Guide.
Measures
Acceptability and feasibility
A semistructured interview and a satisfaction questionnaire adapted from a previous study were administered to assess participants' impressions of the intervention. The semistructured interview 24 includes 13 open-ended questions that address kit usage, barriers, ways the kit was helpful, learning, and general feedback. The satisfaction questionnaire 24 contains 11 yes or no questions about the kit's usefulness, teaching capability, and trustworthiness, followed by 3 questions regarding the kit's design.
Statistical analysis
Data from semistructured interviews were summarized by categorizing how children and caregivers used the kit, barriers that prevented use of the intervention, and types of learning from the kit. Data from the satisfaction questionnaire were summarized using frequencies.
Results
Twenty-five child participants (14 males) ranged from age 7 to 13 years (M = 9.6; SD = 2.2). In this cohort, children were most commonly allergic to peanuts, tree nuts, eggs, sesame, and shellfish. Seventy-six percent of children reported 2 or more allergens. All caregivers identified as parents and most were mothers (88%). See Table 1 for demographic characteristics.
Results suggest that children and caregivers found the intervention acceptable: most (80%–100%) participants reported that the invention materials were trustworthy, found the kit easy to use, liked the appearance of the kit, and would recommend the Cellie Coping Kit to others (Table 2). In addition, parents and children found the kit engaging. For example, 1 child (male, age 12) commented, “I used it [the kit] with my mom and by myself. [We] went over how to deal with [food allergies] and what [cards] to use.” Children also found the Cellie Coping Kit comforting. For example, 1 child (male, age 12) commented, “[I] played with [Cellie] when I was nervous.” A few children (ages 7–8) reported that the coping cards contained too many words and that the directions were confusing. A parent of a 12-year-old male who reported not using the kit stated, “It was not a good day for my child; the food challenge was tough.”
In cases where a child or parent skipped a question, valid percentages are reported.
Results also suggest that children and parents found the intervention feasible (Table 2). Families reported using the kit for comfort, fun, to facilitate discussion, and for coping tips. For example, the parent of a 7-year-old male commented, “[He] used Cellie to make him feel better.” A parent of a 10-year-old female shared, “We discussed scenarios on the cards and how she can handle them when a parent is not there.” When asked about what parts of the intervention were used, many parents and children reported finding the chef card helpful. Intervention barriers included busy schedules, age (some parents thought the material was aimed toward younger children), and time of delivery (after or during a food challenge in which some children were experiencing distress).
Regarding learning outcomes, 65% (n = 13) of children and 57% (n = 12) of parents reported learning from the Cellie Coping Kit: new coping tips (eg, ways to cope with anxiety/nerves), new ways to discuss food allergies, and gaining a new perspective on food allergies. For example, 1 child (male, age 12) stated, “[I] used the cards about shyness and being ashamed.” A parent of a 7-year-old female commented, “[We] had a dialogue about feeling fear in certain settings that my child has never talked about before.” A child (male, age 11) reported that he learned, “You don't have to be scared because you can encourage yourself.” Another child (male, age 8) explained that he learned, “It is okay to get frustrated about allergies.”
Regarding acceptability, 80% (n = 16) of children and 91% (n = 19) of parents stated that they would recommend the Cellie Coping Kit to other families. When we asked participants what we should tell others about the kit, a parent of a 10-year-old female stated, “[The Cellie Kit] has lifesaving tips.” Another parent (of a 7-year-old female) said, “If you are feeling frustrated about how to handle your kid's allergies, use this kit. It reduces anxiety for both parent and child.” A male, age 11, stated, “[The Cellie Kit] is helpful and picks up your spirit.”
Discussion
Children with food allergies are faced with numerous diverse challenges every day.5,6,8,10,11 Psychosocial resources to help children and their families manage food allergies are limited. 5 The development and initial evaluation of the evidence-based Cellie Coping Kit for Children with Food Allergies take a step forward toward filling these gaps. Results of this pilot study are promising: the majority of participants found the intervention to be trustworthy and provide helpful tips. Many children reported learning new strategies or information that helped them manage their food allergies and/or emotional response to food allergies. In addition, most families reported that the Cellie Coping Kit intervention was feasible to implement without additional support from the medical team or a mental health provider.
The Cellie Coping Kit provided an avenue for families to improve communication about the challenges of food allergies. This is consistent with findings from both the cancer and sickle cell disease versions of the coping kit.24,27 Open communication about various illness-related topics (eg, treatment, feelings, acceptance, and experience) can help families function cohesively and minimize perceived disease burden. 28 For pediatric populations who must deal with chronic medical conditions, resources like the Cellie Coping Kit may make it easier for families to identify, articulate, and discuss challenges.
In pediatric patients with a chronic disease, a comprehensive understanding of their condition is an important step toward self-management, which is necessary to maximize efficient treatment and clinical outcomes. 29 The majority of children (60%) reported learning from the Cellie Coping Kit, including new information about food allergies and coping tips. Parents also noted that the kit included information to help manage allergic reactions, including lifesaving information. Food allergies are the number one cause of emergency room visits for anaphylaxis 1 ; use of the Cellie Coping Kit may help provide information in a developmentally appropriate way about how to avoid anaphylaxis and how to manage it when it does occur.
Results from this pilot study suggested that the Cellie Coping Kit was likely most beneficial to young children (eg, 12 and younger). Families commented that it would be most helpful to receive the Cellie Coping Kit either when the child was young (eg, 3 or 4 years old) or at the time of a new food allergy diagnosis. While most parents had already been managing food allergies for some time, 57% reported learning new tips from the kit. These findings are consistent with those of the cancer version of the kit: families reported that this type of resource is most helpful early on when first learning how to manage children's medical conditions. 22 Nearly two-thirds of participating parents reported a graduate or professional degree; thus, it is likely (given their education level) that parents in the current study were able to seek out information as needed to help manage their child's food allergy challenges. While families suggested the most benefit for children who were younger, children under 8 years likely need additional assistance from caregivers or medical teams to promote full understanding of the coping tips.
Barriers implementing the Cellie Coping Kit intervention included integrating it into a busy schedule and difficulty transporting the kit between houses when the child has more than 1 residence. In both cases, medical teams can help families overcome these barriers by integrating the Cellie Coping Kit into standard care during office visits. For example, the medical team can encourage bringing the Cellie Kit to appointments, use the kit to assess current challenges in the family, and help families identify strategies during appointments. In families where children have multiple residences, children may benefit from having a kit at each household.
Several limitations exist in this initial pilot study. The small and relatively homogeneous sample may limit generalizability of results. While results are promising of this intervention, future research should aim to include a more diverse sample such as including patients from different geographic regions, families with greater variation in caregiver education, and a wider range of socioeconomic statuses. This increased diversity will better address generalizability regarding acceptability and feasibility of the Cellie intervention with this population. The semistructured interviews and satisfaction questionnaires used in this study were originally developed to evaluate the Cellie Coping Kit for children with cancer; psychometric properties are not available for these measures, so results should be interpreted with this in mind. Additionally, follow-up assessment at 4 weeks postbaseline did not provide information on longer term usage of the coping kit. Finally, this pilot study was not designed to assess intended intervention outcomes (eg, coping behavior and improved adherence to medical recommendations). Future research in larger samples should examine targeted outcomes over a longer follow-up period.
Conclusions
We were able to create a low-cost, evidence-based coping tool that was well received by children and families of children with food allergies. It should be noted that the Cellie Coping Kit is not intended to be a substitute for behavioral health services or medical team support. Rather, the kit can be used along with other support systems (eg, psychologists, medical professionals, teachers) and facilitate an open dialog between caregiver and child. More research is necessary to examine how families from diverse socioeconomic and ethnic backgrounds implement the Cellie Coping Kit intervention and to assess the impact of the intervention on targeted outcomes, but these pilot results are promising and suggest that this type of coping intervention may benefit children with food allergies.
Footnotes
Acknowledgments
The authors would like to thank The Children's Hospital of Philadelphia Food Allergy Research Fund and The Florence Forgotson Charitable Foundation for supporting this project. In addition, the authors would like to thank Anne Vinsel, MS, MFA, Katie Romanski, RN, BSN, and Yuran Kim Chi, RN, BSN for their contributions to this project.
Author Disclosure Statement
Meghan Marsac, PhD, is a coinventor of the Cellie Coping Kit. The Children's Hospital of Philadelphia and coinventors may benefit financially from the kit. Revenue will be steered back into research in accordance with the Children's Hospital of Philadelphia's nonprofit status. The research presented in the article has been approved by the Hospital's Conflict of Interest committee. All other authors report no disclosures.