
Abstract
Atopic dermatitis (AD) is the most prevalent dermatological disease in the pediatric population. It is a chronic, pruritic, and inflammatory skin disorder, with a complex etiology involving genetic predisposition, skin barrier defects, and immune dysfunction. AD can be a challenge for patients, physicians, and caregivers and has a clear impact in patients’ quality of life (QoL). Educational programs for patients with AD and their caregivers are effective in improving adherence, QoL, and clinical outcomes. Different models of educational programs exist and their structures depend on cultural, social, and economic factors. To improve existing programs, the educational team should go beyond the disease and have a broader view of the many aspects involved in the pathological process. These include psychological, environmental, social, financial, and cultural aspects. Patients and their caregivers should have a more realistic expectation about the treatment. Innovative methods and approaches like design thinking can create new and effective solutions for patients with AD and their caregivers.
Introduction
A
AD is defined as a chronic, pruritic, and inflammatory skin disorder, with a complex etiology involving genetic predisposition and skin barrier defects such as filaggrin mutations, immune dysfunction, and environmental and/or psychological triggers. 3
The disease can be a challenge for patients, physicians, and caregivers4,5 and has a clear impact in patients’ quality of life (QoL).6,7 The presence of recalcitrant pruritus greatly affects the child's quality of sleep. 8 AD can also have its effects on caregivers, as shown by higher incidence of anxiety and depression. 9
Why Do We Need Educational Programs for AD?
Despite great advancements in our understanding of the immunologic mechanisms and skin barrier defects in AD, the management of this chronic condition often remains a challenging and frustrating problem for patients, caregivers, and healthcare providers.
Not surprisingly, we continue to solely rely on the paternalistic and informative model of the doctor/patient relationship. In this model, the doctor has all the answers and will provide all the support and technical information and expect that the patient will follow through his or her expert advice. 10 Unfortunately, this approach seems to be failing, especially in the management of chronic diseases. Above other factors, time constraints prevent the doctor alone from providing all the appropriate care needed by patients and caregivers.
In a recent survey conducted on the Internet by the Brazilian Atopic Dermatitis Association, nearly 80% of patients suffering with AD showed dissatisfaction with their treatment. A common perception was that doctors do not know how to manage the disease. Patients complain that doctors do not show a clear knowledge of the disease and fail to provide any emotional support. Consequently, patients and caregivers report seeing many doctors to treat their condition. 11
Educational programs were created to fulfill the need for more comprehensive and effective care in AD. In these programs, a multidisciplinary team, composed by doctors and other healthcare professionals, provides necessary information and tools for both patients and their caregivers. Parental education programs in AD have been described as very effective as a strategy for improving AD treatment in some countries.3,12–16 Multidisciplinary interventions aiming at AD patients and their caregivers generate enhanced disease control, as a consequence of stronger adherence, reduced corticophobia, decreased inflammation, and improvement of QoL and outcomes.2,17,18
What is the Evidence of the Effectiveness of Education in AD?
The relevance of education strategies for AD patients and caregivers has become an essential step in the international treatment guidelines worldwide.
One of the pioneer studies focusing on parental education and AD was reported by Broberg et al. in 1990. 19 The study evaluated the role of eczema school for 2 groups of 50 families of children with AD: one group received routine information given by the physician during the medical visit, and the other received further information on eczema treatment and practical training in controlling atopic eczema from a registered nurse. The therapeutic effect was better in the group that had received extra guidance. Other studies followed the educational track for caregivers of children with AD, always demonstrating the beneficial effects of such approach in the follow-up of the disease. 20
Wenninger et al. in 2000 described in detail the Berlin education program, which included medical, nutritional, and psychological issues. 21 This program consisted of six 2-hour group weekly sessions, limited to a maximum of 8 couples. There was also an interdisciplinary team that included pediatricians, psychologists, and dieticians. Interestingly, the participants had homework assignments, which included a symptom and nutritional diary, monitoring reactions to scratching, and bringing questions to the sessions. Children with AD included in this program were 5 months to 9 years old, with a mean age of 3.1 years. SCORAD (Scoring Atopic Dermatitis index) was the severity score utilized in the study, and the average decrease was 20.5 points. The QoL index assessed in the project was HRQoL (Health-Related Quality of Life). Two years later, the same German group led by Staab (2002) published a follow-up study, reporting the experience of 204 families with children with moderate to severe AD who enrolled in the program. 22 The results showed a significant change in treatment behavior, especially regarding the application of emollients and topical therapy, and reduction of treatment costs.
In 2003, Cork et al., from the United Kingdom, published a study that aimed to determine the effect of education and demonstration of topical therapies by specialist dermatological nurses on therapy utilization and severity of atopic eczema. This study involved 51 children with AD, who were followed for 1 year. The authors utilized the Six Sign Atopic Dermatitis Severity Score (SASSAD) and parental assessment of itch, sleep disturbance, and irritability. Fifty-one children and their families were exposed to repeated education and demonstration of topical therapies by a nurse, which resulted in 89% reduction in the severity of eczema, with an 800% increase in the use of emollients. 12
In Japan, Futamura et al. performed a randomized controlled trial (RCT) study in 2013 that analyzed the effects of a short-term Parental Educational Program (PEP) on childhood AD. 23 They evaluated the long-term effects of a 2-day PEP. Fifty-nine children with moderate to severe AD and their mothers were enrolled to join the program, which consisted of a booklet with information about the disease and conventional therapy, with or without a 2-day PEP, including a day in the hospital. SCORAD was the chosen instrument for AD evaluation. The authors detected that PEP had a positive long-term effect on eczema severity and reduction in parental anxiety in relation to corticosteroid usage.
From a global perspective, there are 2 relevant studies that compile projects about patients with AD and education (Table 1): one was published by Ersser et al. in 2014, and comprehends a Cochrane review,14,24 and the other represents a position article by Barbarot et al., from 2013. 25
AD, atopic dermatitis; CDLQI, Childrens' Dermatology Quality of Life Index; IDQOL, Infants' Dermatology Quality of Life; QoL, quality of life; RCT, randomized controlled trials; SCORAD, Scoring Atopic Dermatitis index.
In 2016, an excellent review from Ahrens and Staab 26 listed the main goals of patients and parent education in AD: improvement of self-management skills and self-responsibility; promotion of a better outcome of AD; promotion of a better QoL for patients and caregivers, and reduction of treatment costs and secondary prevention of comorbidities, including respiratory and mental health disorders.
Currently, various severity scales and measures are being used in AD studies. The definition of relevant clinical outcome measures for AD is crucial for conducting future therapeutic strategies. 3 Therefore, the creation of a task force to study outcome measures for AD was mandatory. The HOME (Harmonizing Outcome Measures for Eczema) initiative is a first attempt to standardize outcome measures for future studies and has defined 4 outcome domains: clinical signs, symptoms, QoL, and long-term control of flares.18,26–28
Going Beyond Education
Education can be defined as the act or process of imparting or acquiring a particular knowledge or skills. 29 Educational programs can impart relevant information for patients and caregivers and, consequently, improve the understanding about the disease. However, explaining how the disease works and what medications to use may not be sufficient. Education should have a more comprehensive role in chronic disease management.
Robert Wood Johnson Foundation, the largest private U.S. grant maker focused on health, estimates that only 20% of a person's health is related to healthcare. The rest stems from behavioral, environmental, and social factors (Fig. 1). 30
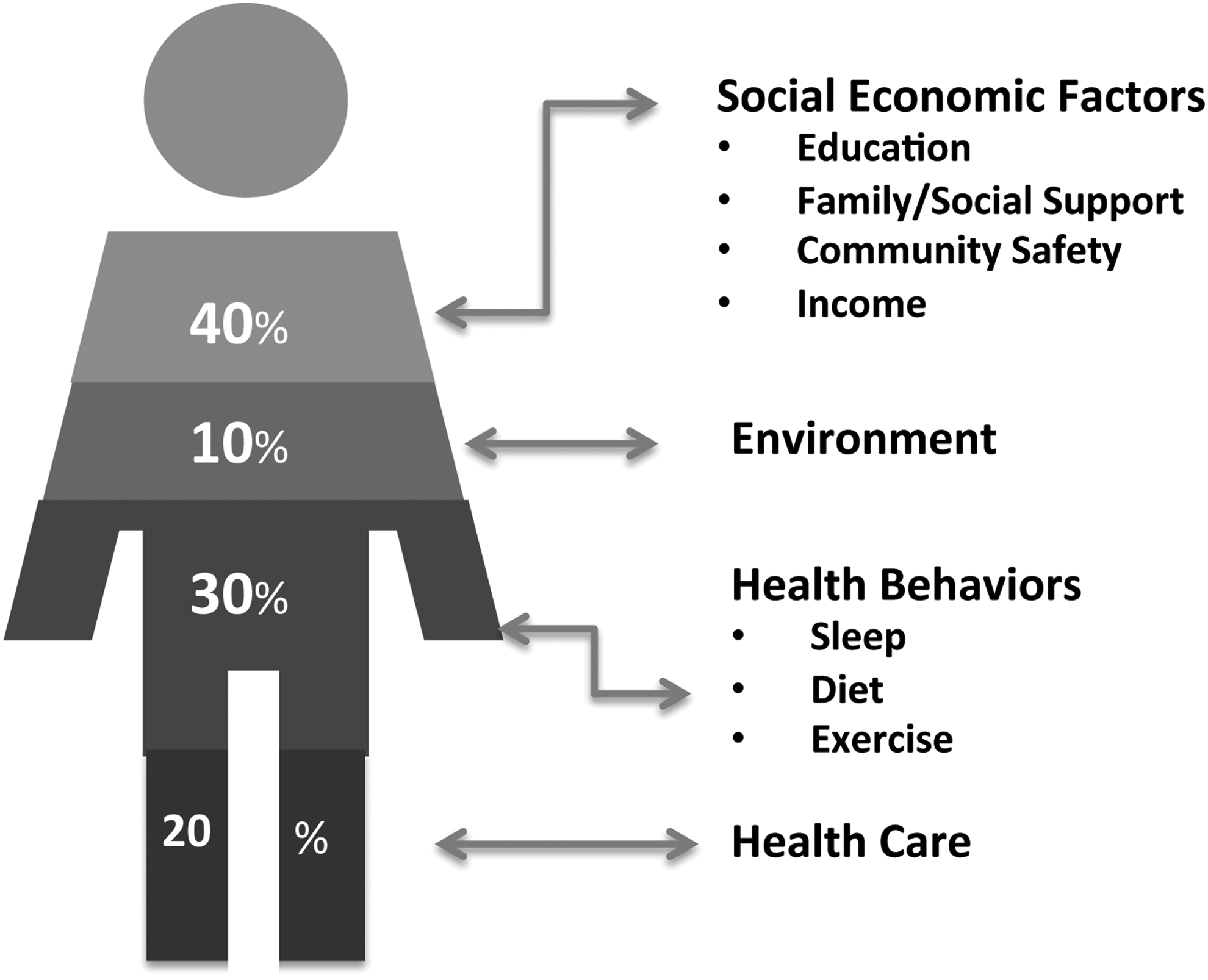
Factors that go into a person's health.
Educational programs for AD are complex entities and require time and financial support to work. With a few exceptions, current programs reach a limited number of patients, and long lasting programs are rare. To improve existing educational programs, healthcare providers who make up the educational team should go beyond the disease and beyond clinical walls and have a broader view of the many aspects involved in the pathological process, including social, emotional, financial, and cultural aspects. Community outreach activities for patients and caregivers such as local support groups, as well as disease awareness walks and activities, organized by AD nonprofit organizations are a few examples of straightforward approaches that could be promoted to improve current educational programs. Art therapy can bring beneficial effects in the treatment of asthma and could also be used for patients with AD. 31
Innovation processes like design thinking is another approach with a lot of potential for creating new solutions in the educational area for patients with AD and their caregivers. Design thinking is a creative innovation process originally used by designers to enhance the look and functionality of products. More recently, this process has also been used to deal with complex social and health problems. Design thinking is a human-centered approach that, when applied to healthcare, involves listening closely to patients’ needs and problems. 32 Design thinking allows creative and effective solutions to appear from patients themselves rather than being imposed by the healthcare professional. It also involves working in collaboration with a multidisciplinary team that includes patients and their families, doctors, psychologists, nurses, social workers, and others.
Recommendations for AD Educational Programs
Empathy: Healthcare providers have to be aware of common—but not usually acknowledged—problems faced by patients with AD and their caregivers. These may include frustration, isolation, shame, anger, and depression.
Integrative thinking: Besides analytical/scientific thinking, healthcare providers have to integrate patients’ cultural values, experiences, and limitations into their clinical decisions.
Creativity and experimentation: Adding artistic activities like drawing, origami, poetry, and music into AD educational programs can be powerful tools.
Collaboration: The educational team should include physicians, patients, parents/caregivers, psychologists, nurses, social workers, nutritionists, artists, volunteers, and anyone willing to improve patients’ growth and self-development.
Optimism: There is always a potential solution better than the existing alternative (Adapted from T Brown).32,33
Contrary to the belief that medication alone can treat and solve all problems, design thinking shows that to be effective, the management of AD must constitute a much broader approach, encompassing emotional, social, cultural, and financial factors.
Patients should also have a more realistic expectation about the treatment and should not expect a swift and miraculous cure. An active partnership between healthcare professionals and patients should be established for the development of an effective therapy in AD.
Conclusions
Educational programs for patients with AD and their caregivers are effective in improving adherence, QoL, and clinical outcomes. Different models of educational programs exist and their structures depend on cultural, social, and economic conditions. Healthcare providers who work with AD patients and their caregivers must go beyond the disease and have a more comprehensive view of the many aspects involved in the pathological process. These include psychological, environmental, social, financial, and cultural aspects. To be more effective, an active participation of patients and caregivers will be needed in the process of constructing new and improved models of educational programs. Innovative methods and approaches like design thinking, which uses empathy, collaboration, and experimentation, can create new and effective solutions for patients with AD and their caregivers.
Footnotes
Author Disclosure Statement
No competing financial interests exist.