
Abstract
Second-hand smoke (SHS) exposure has been associated with significant health consequences in children. The objective of our study was to assess patterns of smoking, perspectives on smoking, and housing characteristics of families of infants with bronchopulmonary dysplasia (BPD) in the outpatient setting. From 2012 to 2014, caregivers of subjects who were recruited from a BPD outpatient clinic completed self-reported questionnaires regarding exposure to tobacco smoke in the home, patterns of smoking, household rules regarding smoking, and residence type. Caregivers of 222 subjects with BPD completed the questionnaire. Of these, 42 (18.9%) reported that a smoker lived in the home. Households that contained smokers were more likely to have lower median household income, be covered by public insurance, and have less education. Among households that included smokers, 7% reported that smoking was allowed inside the home, while 93% reported that smoking occurred only outdoors. Caregivers of nonsmoking households and smoking households reported that 57.5% and 59.5%, respectively, lived in attached housing or multiunit buildings. Households with smokers who lived in multiunit housing and were familiar with their properties' smoking rules (n = 23) were more likely to live in properties where smoking was permitted (78%), compared to nonsmoking families who were familiar with their property's smoking rules (43%; n = 77; P = 0.012). Nonsmoking families who live in multiunit housing that allows smoking on the property may be inadvertently exposed to SHS. The majority of smoking families report smoking outdoors, which still may be a measurable exposure that can have detrimental health consequences on BPD infants, an already medically fragile population.
Introduction
S
BPD is a form of chronic lung disease that primarily affects extremely low-birth-weight infants. Infants with BPD are more prone to respiratory infections, development of asthma-like symptoms, and hospitalizations due to respiratory illnesses, than infants without BPD.5–9 In addition to SHS, third-hand smoke (THS), which is residual tobacco smoke contamination that remains after the cigarette is extinguished, may be associated with health risks in children. 10 Due to increased morbidities associated with BPD in preterm infants, it is important to minimize modifiable postnatal risk factors such as SHS and THS to optimize lung function in later life.
Previous studies have shown disparate results with regard to associated respiratory morbidities in the preterm population and SHS. While Halterman et al. 4 found that very low-birth-weight infants exposed to tobacco smoke were more likely than unexposed infants to require acute care for respiratory problems, other studies11,12 did not see an association. Collaco et al. 12 measured hair nicotine levels as a marker of chronic tobacco smoke exposure in infants with a history of BPD who presented to an outpatient clinic. They found a significant association between higher hair nicotine levels and increased hospitalization rates and activity limitation in infants with BPD who required respiratory support at their initial outpatient visit.
Given the potential detrimental effects of SHS and THS on infants with BPD, we sought to ascertain smoking patterns, attitudes, and regulations in the BPD population. We hypothesized that most caregivers of children with BPD who did not report a smoker in the home would be more likely to have rules against in-home smoking than those with a smoker in the home. However, we further hypothesized that most caregivers of children with BPD who reported a smoker in the home would also have rules against in-home smoking. We assessed second-hand smoking rules in the BPD population using 222 patients who were recruited from our outpatient BPD clinic.
Materials and Methods
Study population
All subjects were recruited from the Johns Hopkins Bronchopulmonary Dysplasia Clinic between January 2012 and January 2014. Patients were referred to the clinic by area neonatal intensive care units (NICUs) or pediatricians on the basis of prematurity and BPD as per National Institute of Child Health and Human Development criteria. 9 Of 227 patients recruited with a diagnosis of BPD and born at ≤36 weeks of gestation, 222 completed the questionnaire. This study was approved by the Johns Hopkins Institutional Review Board (protocol #NA_051884). Participating parents and caregivers provided informed consent for study participation.
Questionnaire data
The questionnaire was adapted from the 2011 Social Climate Survey of Tobacco Control (www.socialclimate.org) and contained information about self-reported exposure to tobacco smoke in the home, patterns of smoking, household rules regarding smoking, and where patients live (see Supplementary Data; Supplementary Data is available online at www.liebertpub.com/ped). Clinical data, including birth weight, the presence or absence of gastrostomy tubes, Nissen fundoplication, home supplemental oxygen, and home mechanical ventilation were obtained through chart review. Race and primary caregiver education level were self-reported. Median household income was derived from the 2010 US Census data based on residential zip code. Health insurance information was obtained from billing records.
Statistical analyses
Differences between smoking and nonsmoking households were assessed using either χ2 or t tests. All statistical analyses were conducted in Stata IC 11.0 (College Station, TX), and P values <0.05 were considered statistically significant.
Results
Demographics
A total of 222 caregivers completed the questionnaire and of these 42 (18.9%) indicated that there was a smoker living in the home (Table 1). 61.3% of the subjects were male and 65.3% were nonwhite. The mean gestational age of all subjects was 27.1 weeks. 41.9% of subjects were on home supplemental oxygen, and 34.7% of subjects had a gastrostomy tube at the time of initial BPD clinic visit.
NICU, neonatal intensive care unit; SD, standard deviation.
The median estimated household income of the study population was $66,300, and 61.7% of subjects had public insurance. Families with a smoker living in the home had a lower median household income (P = 0.040), were more likely to be covered by public insurance (P = 0.030), and have significantly less education compared with caregivers living in a nonsmoking household (P = 0.001). There was no difference in gender, race, gestation, or birth weight between children living in a household with a smoker.
When comparing clinical characteristics, there were no differences in age of discharge from the NICU, home ventilator use, gastrostomy tube placement, or inhaled corticosteroid use before 2 years of age. However, children of nonsmoking households were more likely to be discharged to home on supplemental oxygen (P = 0.050) and to have a Nissen fundoplication (P = 0.040) compared to children living in households with a smoker.
Patterns of smoking
Of the 42 households with smokers, the primary caregiver was the only smoker in 26% of the households. In 33% of households, someone other than the primary caregiver was the smoker and in 40% of households, the primary caregiver and another occupant(s) in the household were smokers. Among households in which a smoker lived, 7% reported that smoking occurred indoors and 93% reported that smoking only occurred outdoors. Of those who smoked outdoors, 41% reported smoking taking place in a garage, 41% reported smoking taking place near the home (ie, porch, deck), and 18% reported smoking taking place away from the home. Of the 42 households that reported the presence of a smoker, 7% reported exposure to smoke in a car.
Rules on smoking
Caregivers were also queried regarding rules about smoking in cars and in their homes. Thirty-six households with a smoker reported on rules about smoking in the home. Of the households who had smokers, 8% allowed smoking inside the home, but only when the child was not present and 92% of caregivers allowed smoking only outside the home. Seventy-four percent of smoking households reported that smoking is never allowed in their cars, 14% reported that smoking in the car is allowed when children are not present, 5% reported that smoking in the car is allowed at any time, and 7% reported that they do not own a car. All nonsmoking households stated that smoking is prohibited in their homes and cars.
Housing characteristics
Housing characteristics of smoking and nonsmoking families were assessed. Of the 42 households that reported the presence of a smoker, 17 (40%) reported living in a home detached from any other home, 17 (40%) reported living in a home attached to other homes (eg, duplexes, row houses, and townhouses), and 8 (19%) reported living in a multiunit building (apartments or condominiums) (Fig. 1). Of the 180 households with no smokers in the home, 78 (43%) reported living in a home detached from any other home, 64 (36%) reported living in a home attached to other homes, and 38 (21%) reported living in a multiunit building. There was no difference in housing type by household smoking status (P = 0.835). There was a tendency for smoking households that live in multiunit housing to be more familiar with their property's smoking rules compared to nonsmoking households that live in multiunit housing (92% versus 75%, P = 0.071) (Fig. 2). Smoking households that were familiar with their property's smoking rules (n = 23) were more likely to live in properties where smoking was permitted, compared to nonsmoking families who were familiar with their property's smoking rules (n = 77). Specifically, of the 23 smoking households that were familiar with their property's smoking rules, 18 (78%) reported that smoking was permitted anywhere on the property, 1 (4%) reported that smoking was permitted only in individual units, and 4 (17%) reported that smoking was not permitted at all. Of the 77 nonsmoking households that live in multiunit housing and were familiar with their property's smoking rules, 33 (43%) reported that smoking was permitted anywhere on the property, 7 (9%) reported that smoking was permitted only in individual units, and 37 (48%) reported that smoking was not permitted at all (P = 0.012 for all 100 households that were familiar with their property's smoking rules).

Residence type by smoking status.
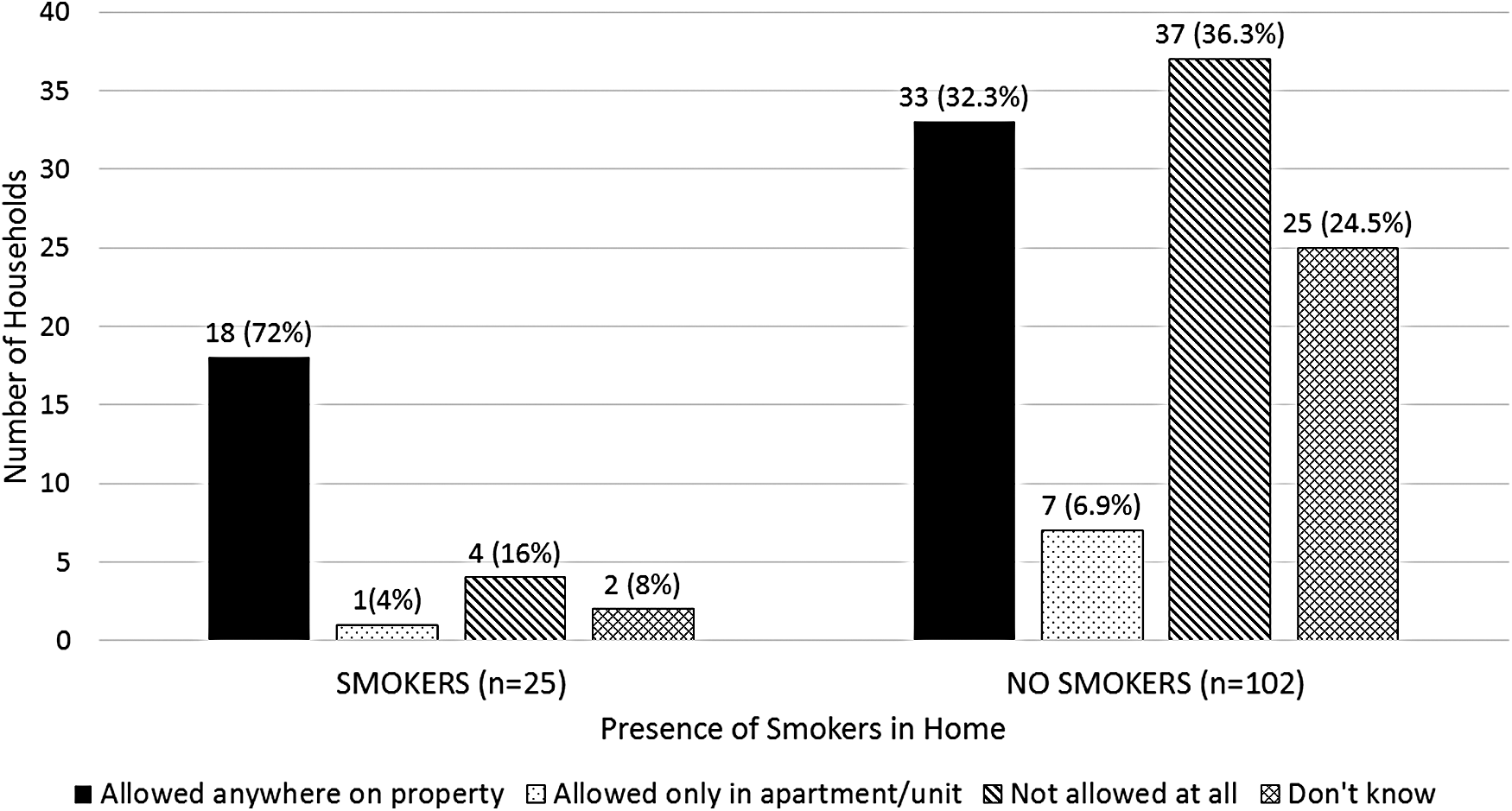
Rules on smoking in multiunit or attached housing.
Discussion
In this study, we found that 18.9% of children with BPD seen in an outpatient clinic lived in a household with at least 1 smoker. The prevalence of SHS in our BPD outpatient population was less than that of the overall prevalence in the general pediatric population (40.6% in children age 3–11 years surveyed in 2011–2012). 13 However, SHS may still have important health consequences for this vulnerable population. In addition, demographic analysis of our BPD population showed that BPD infants exposed to SHS were also from a socioeconomically disadvantaged group, which may further increase their vulnerability to poor outcomes.
In our study, the majority of smoking households (92%) and all nonsmoking households prohibited smoking in their homes. These figures are higher compared to those reported in a Centers for Disease Control and Prevention (CDC) study, which found that 89.1% of nonsmoking households and 48.0% of smoking households have a smoke-free home rule. 14 Similarly, in our study, the majority of smoking households (74%) and all nonsmoking households reported that smoking is prohibited in their cars. Again, our figures are higher compared to those reported in a CDC study, which showed that 84.9% of nonsmoking households and 27.0% of smoking households have a smoke-free vehicle rule. 14 Findings from our study suggest that nonsmoking families of children with BPD may seek to limit SHS exposure by enforcing specific smoking rules in the household.
However, these families may still be exposed to SHS if they live in proximity to smoking households via attached housing. Wilson et al. showed that children who live in apartments had higher cotinine (a nicotine metabolite) levels compared to those who live in detached housing. 15 In our population, more than 50% of children with BPD live in attached or multiunit housing. Many nonsmoking households who live in multiunit housing are not familiar with their property's smoking rules. Therefore, these families may be inadvertently exposed to SHS if they happen to live on a property that allows smoking inside the building.
Studies have shown that the risk of SHS exposure in multiunit residential buildings is high, as smoke can enter the home from hallways, balconies, air conditioners, and gaps between floors and walls. Enclosed public areas—such as common areas—are public places within these buildings where SHS can occur. 16 In our study, we found that some nonsmoking families who knew their property's smoking rules still resided in housing that allowed smoking on the property (43%). This finding suggests that BPD infants who live in these households may be exposed to SHS.
Our study had limitations that should be considered when interpreting the results. First, our sample was recruited from a primarily urban population, which may not necessarily represent the BPD population in other areas of the country. Second, our patients were recruited from a tertiary care center, so compared to patients from a nontertiary care center, our patients may have more severe disease and/or more complex medical diagnoses. Third, our method of using questionnaires may underreport exposure to SHS, especially in those infants who are inadvertently exposed to SHS or in families who underreport due to social desirability. Caregiver questionnaires may fail to capture infants who are exposed to SHS compared to nicotine and cotinine levels. This discrepancy may be either intentional (ie, social desirability) or unintentional (ie, nonsmoking families are inadvertently exposed to SHS).
In a previous study, we found measurable levels of nicotine in the hair of children with BPD in both smoking and nonsmoking households by caregiver report. This would suggest that children in nonsmoking households may be exposed inadvertently by living in attached housing near a smoker or that smoking was reported incorrectly by the caregiver due to social desirability purposes. For children living in smoking households where smoking is reported to occur only outdoors, the location of smoking may have been reported incorrectly by the caregiver due to social desirability purposes or represent third-hand exposure, which has been reported to occur indoors in settings where smoking does not take place (eg, NICUs). 17
In conclusion, we found that although most caregivers enforce smoking bans within the home, children with BPD may still be exposed to nicotine due to proximity to smokers in multiunit or attached housing or THS exposure from those who smoke outdoors. These inadvertent SHS and THS exposures may contribute to adverse pulmonary outcomes in this population already at increased risk for respiratory morbidities.
A recent policy enacted by the federal government may help to diminish these SHS and THS exposures. On November 30, 2016, the United States Department of Housing and Urban Development issued a nationwide smoking ban in all public housing units, including outdoor areas within 25 feet from the building. 18 Policies such as this recent smoking ban may provide healthier home environments for children overall, but especially for children with BPD, who are at greater risk for respiratory exacerbations and acute care usage due to their underlying chronic lung disease.
Footnotes
Acknowledgments
The authors thank the families and patients of the Johns Hopkins Bronchopulmonary Dysplasia Clinic, who participated in this study. This work was funded by the American Academy of Pediatrics FAMRI (Flight Attendant Medical Research Institute) Richmond Center of Excellence, which did have not have input into the study design, analysis, decision to publish, or manuscript preparation.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.