
Abstract
Common variable immunodeficiency (CVID) is a heterogeneous group of diseases characterized by hypogammaglobulinemia, leading to recurrent infections. Defect in maturation of B cells into functional plasma cells is the most principal defect in CVID. B cell maturation antigen (BCMA) is an essential molecule for survival of long-lived plasma cells. The aim of this study is to evaluate BCMA expression on B cells as well as count peripheral blood plasmablast cells in CVID patients compared with healthy individuals. Blood samples were collected from 15 CVID patients and 15 age- and sex-matched normal controls. Genomic RNA was extracted from peripheral blood mononuclear cell samples using an RNX-Plus Kit. cDNA was synthesized from extracted RNA using a RevertAid First Strand cDNA Synthesis Kit. Synthesized cDNA was used as a template for reverse transcription polymerase chain reaction (RT-PCR) to measure BCMA gene expression by Maxima SYBR Green/ROX qPCR Master Mix Kit (Thermo Scientific). Flow cytometry was used to measure plasmablast counts in the peripheral blood. RT-PCR results showed that the expression of BCMA in CVID patients compared with control subjects was significantly decreased and this decrease was statistically significant (P < 0.046). Accordingly, the flow cytometric results demonstrated that the mean percentage of plasmablast cells and BCMA expression in patients was significantly (P < 0.002) decreased in comparison with the control group. Our data show that decreased BCMA expression as well as reduction of plasmablast cell frequency in CVID patients could be involved in development of CVID.
Introduction
C
B cell maturation antigen (BCMA) is a tumor necrosis family receptor superfamily member 17 (TNFRSF17) that is expressed only on B cells. This molecule is weakly expressed on resting B cells, but its expression is increased on plasma cells and germinal center B cells. BCMA is a vital molecule due to its essential role in the survival of plasma cells that produce long-term humoral immunity.17–20 It has been demonstrated that in BCMA/TNFRSF17-deficient mice, the production of long-lived plasma cells in the bone marrow is severely impaired. 21 Since BCMA is predominantly expressed on terminally differentiated B cells and has an important role in long-term survival of plasmablasts,21,22 defect in differentiation of B cells to plasmablasts and decreased plasmablast counts in CVID patients could be correlated with impairment in BCMA. The aim of this study is to evaluate BCMA expression as well as plasmablast counts in CVID patients compared with healthy individuals.
Materials and Methods
Patients
The study population included 15 patients with a diagnosis of having CVID who were referred to Alzahra Hospital of Isfahan University of Medical Sciences and 15 age- and sex-matched normal controls. Diagnosis of CVID was made by approved criteria, 23 including reduced levels of at least 2 serum immunoglobulins (IgG, IgA, and IgM) by 2 standard deviations from normal mean values for age, exclusion of other causes of hypogammaglobulinemia in individuals with age >4 years, evidence of specific antibody deficiency, and no evidence of profound T cell deficiency. Nobody was receiving the IVIG before sampling. The process of this study was approved by the ethics committee of Isfahan University of medical science, and informed consent was obtained from all participating adult subjects as well as from the parents of young patients.
Flow cytometry
A sample of 5 mL of blood was collected from patients and controls in ethylenediaminetetraacetic acid (EDTA) tubes. Blood samples from CVID patients were always obtained before IVIG replacement. Peripheral blood mononuclear cells (PBMCs) were isolated by Ficoll-Hypaque density gradient centrifugation. PBMCs were harvested and washed with phosphate-buffered saline plus 0 · 5% bovine serum albumin. PBMCs were stained for 20 min at 4°C with 5 μL of the following antibodies: anti-CD38–fluorescein isothiocyanate (FITC) (eBioscience), anti-CD19–phycoerythrin (PE) (eBioscience), anti-IgM−peridinin chlorophyll protein-eFluor710 (eBioscience), anti-CD-19 (FITC) (eBioscience), and anti-BCMA (PE) (Biolegend). Flow cytometric analysis was performed on an FACSCalibur instrument (BD Biosciences, San Jose, CA) and the data were analyzed using CellQuest-Pro software (BD Biosciences).
Real-time quantitative reverse transcriptase–polymerase chain reaction
Total RNA was extracted from PBMC samples using the RNX-Plus reagent (Sinaclon, Iran). The purity of RNA samples was determined using a Nanodrop (WPA, Biowave 2). Then, cDNA was synthesized from extracted RNA using the RevertAid First Strand cDNA Synthesis Kit (Thermo, Fermentas) as instructed by the manufacturer. Synthesized cDNA was used as a template for real-time polymerase chain reaction (RT-PCR) to measure BCMA gene expression using the Maxima SYBR Green/ROX qPCR Master Mix Kit (Thermo Scientific). Amplification conditions were 94°C for 3 min, followed by 40 cycles at 94°C for 30 s, 58°C for 30 s, and 72°C for 45 s. A housekeeping gene (Beta–Actin) expression level was used to optimize BCMA gene expression. Primers were designed using the Gene Runner software (Hastings Software, Inc.; version 3.05). The following primers are provided in Table 1. RT-PCR was carried out in duplicate wells using ABI (Applied Biosystems) StepOne™ instrument and Ct values for target and housekeeping genes were calculated, the results were analyzed with the 2−ΔΔct formula.
BCMA, B cell maturation antigen.
Statistical analyses
To compare results between patients and normal groups, we applied an independent sample t-test. All experiments are presented as mean ± standard error of the mean (SEM) and P < 0.05 was considered as statistical significance. All the analyses were performed using SPSS 16.0.
Results
Characteristics of patients
The study population comprised 15 patients with CVID (8 males and 7 females; mean age 21.06 ± 10.03 years). The mean age at diagnosis was 12.93 ± 7.99 years and the mean age at onset of symptoms was 7.2 ± 6.68 years. The diagnostic delay in the patients was 5.2 ± 5.14 years. Nine patients (60%) were born from a consanguineous marriage. The mean serum IgG, IgM, and IgA levels at the time of diagnosis were 383.5, 23.14, and 19.93 mg/dL, respectively. Demographic and immunological data are provided in Table 2. The most common clinical manifestations among patients with CVID were sinusitis (8 patients), pneumonia (6 patients), and otitis media (6 patients). Other complications were bronchiectasis (4 patients), autoimmunity (4 patients), and allergy (6 patients).
B cells and plasmablast frequency
Mean percentage of B cells and plasmablast cells was calculated in peripheral blood of 15 patients with CVID and 15 controls using flow cytometer (Fig. 1). The flow cytometric results indicated that the mean percentage of B cells in the control group in comparison with patients was not significantly different (P = 0.153) (Table 3). Eight patients had reduced number of B cells, while 5 were in normal range. Two patients had an elevated B cell count (Table 2). As shown in Table 3 and Fig. 2, a significant difference (P = 0.01) was observed between the frequency of plasmablast cells in the control group and patient group. Noteworthy, the frequency of plasmablasts was reduced in all the studied patients (Table 2).
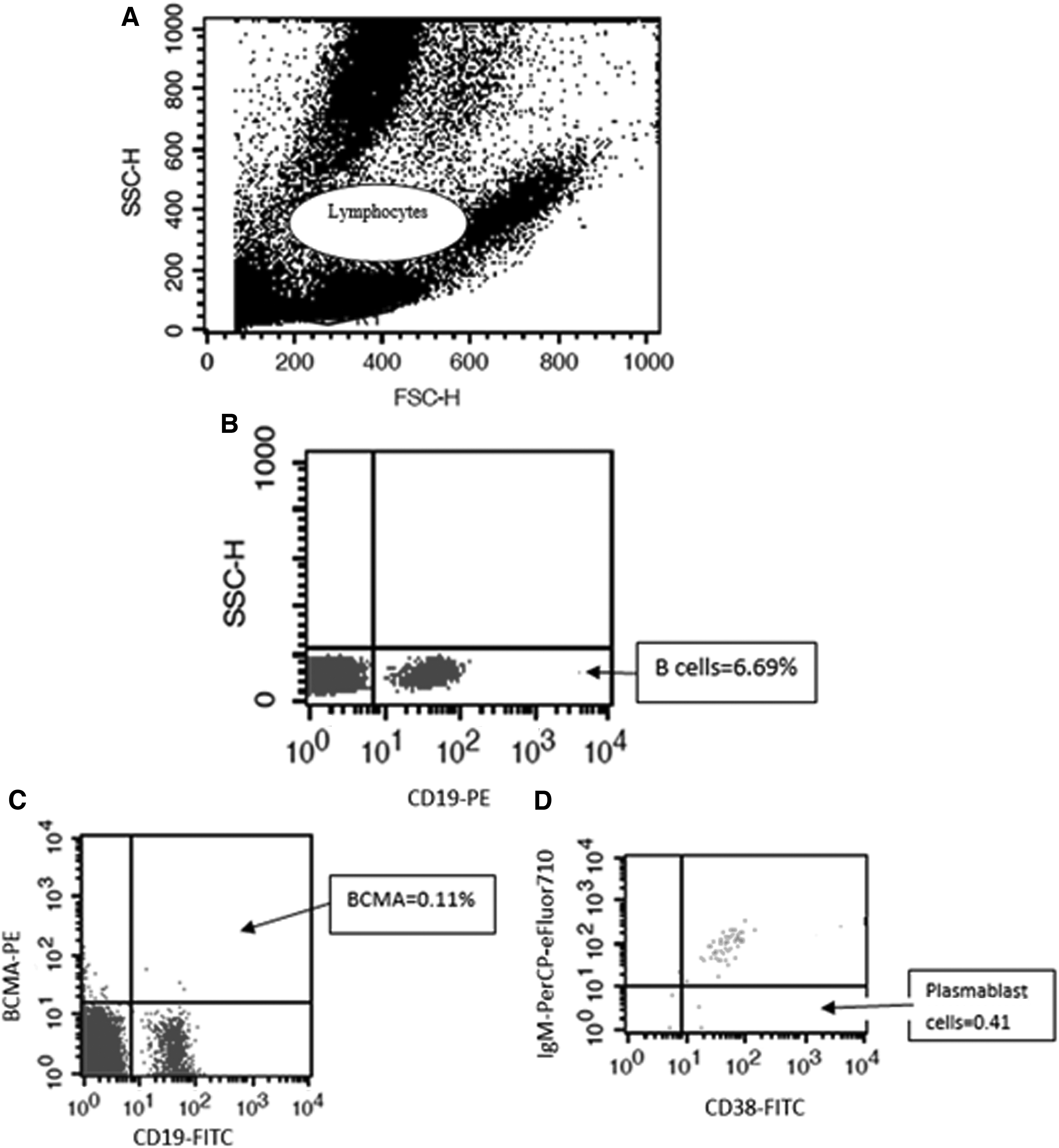
Flow cytometric analysis of B cells (CD19+), plasmablasts (CD19+CD38++IgM−), and BCMA expression in patient samples.
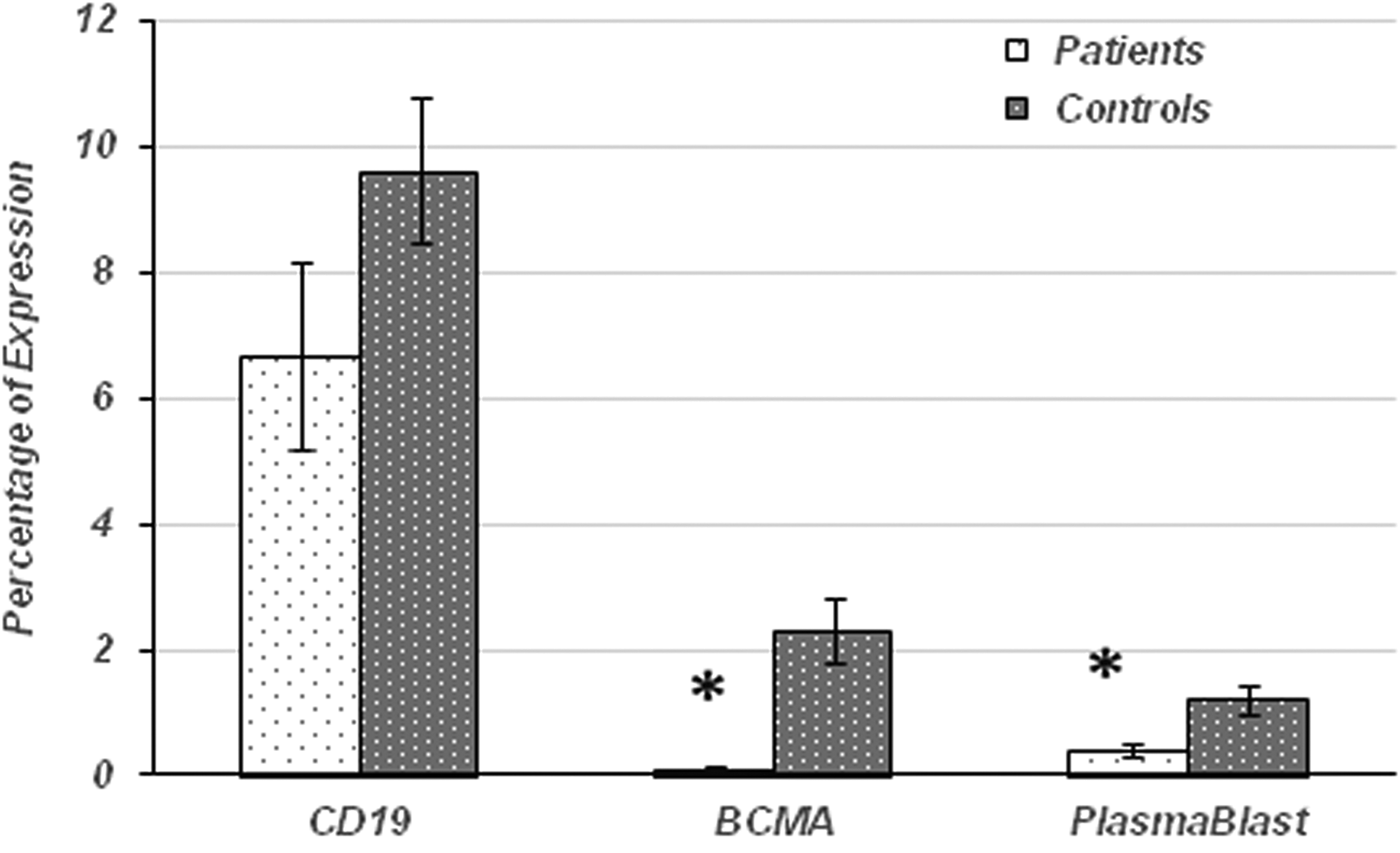
The percentage of B cells, plasmablasts, and BCMA expression in patients with CVID compared with controls. The mean percentage of B cells in CVID patients (n = 15) was not significantly different compared with healthy controls (n = 15), but the mean percentage of plasmablast cells and BCMA in CVID patients (n = 15) was significantly reduced compared with healthy controls (n = 15). Results are represented as mean ± SEM of the flow cytometric analysis of all patients and controls (*P < 0.05). CVID, common variable immunodeficiency; SEM, standard error of the mean.
CVID, common variable immunodeficiency.
BCMA expression
RT-PCR results showed a significant decrease (P = 0.046) in the level of BCMA mRNA in CVID patients compared with control subjects (Fig. 3). Accordingly, flow cytometric analysis showed that BCMA expression were significantly decreased (P = 0.002) on CD19+B cells of patients with CVID compared with controls (Fig. 2 and Table 3). The BCMA level was decreased in all the studied CVID patients (Table 2).

Expression of BCMA mRNA in patients with CVID compared with controls. Transcript level of BCMA in CVID patients (n = 15) was significantly reduced in comparison with healthy controls (n = 15). Results are represented as mean ± SEM of 3 identical repeats of each experiment. Results are normalized versus ACTB as reference gene (*P < 0.05).
Correlation and diagnostic value
Correlation analysis revealed a significant positive correlation between BCMA expression and plasmablast frequency (R = 0.60 and P = 0.001) as well as between BCMA expression and CD19+ cell frequency (R = 0.56 and P = 0.003).
To evaluate the potential of BCMA expression level as a diagnostic biomarker for CVID, we compared the expression level of BCMA from corresponding groups by receiver operating characteristic (ROC) analysis. ROC analysis determined the optimal cutoff value of ≥0.5 for BCMA protein expression to discriminate between CVID and non-CVID individuals with sensitivity and specificity of 100% and an area under the ROC curve (AUC) of 1. The optimal cutoff value for BCMA transcript level was ≥0.29 with sensitivity of 86% and specificity of 40% (Fig. 4).
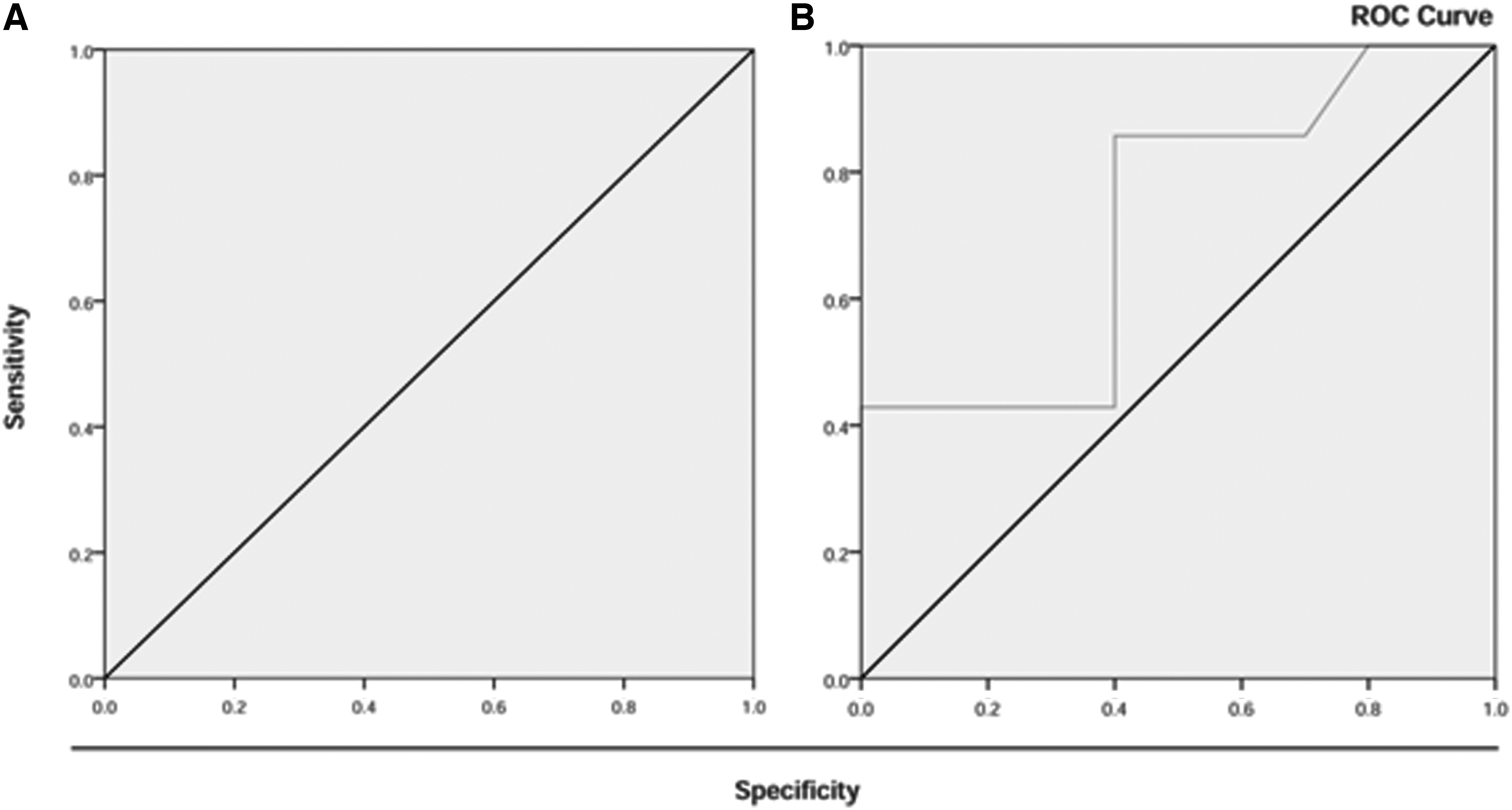
ROC curve of CVID patients versus normal controls analyzed for BCMA expression level in peripheral blood B cells.
Discussion
According to many previous studies, most CVID patients have absent or reduced plasma cells and, on the other hand, BCMA is essential for survival of long-lived plasma cells. Knockdown technology (small interfering RNA) showed that BCMA contributed to both proliferation and survival of B cells.22,24 The role of BCMA in B cells seems to have been disregarded and is much less understood in human diseases. Hence, evaluation of mutations in the BCMA gene and its expression on B cells, as well as counting peripheral blood plasmablast cells, in patients with CVID compared with a normal individual seems to be necessary.
In this study, our flow cytometric results indicated that the mean percentage of B cells in the patient group in comparison with control group was not significantly different, but the mean percentage of plasmablast cells was significantly decreased in CVID patients compared with controls. These findings match the findings of others that most CVID patients have normal numbers of peripheral B cells and the fundamental defect in CVID is lack of maturation of B cells into functional plasma cells and hence sharp reduction or absence of plasma cells.15,25–31
We also showed that the expression of BCMA on B cells was significantly decreased in patients with CVID compared with controls. This is consistent with low frequency of plasmablast cells in CVID patients, which was also found in this study.
Only a similar work that reports BCMA protein expression in patients with CVID is related to the study by Salzer et al. that indicated BCMA protein expression was normal. 32 This is contrary to our findings. Due to racial differences, the cause of disease can be different.
However, other diseases have been studied in association with the BCMA. Previous studies demonstrated that the number of plasma cells and the expression of Blimp1 and BCMA were upregulated in patients with active systemic lupus erythematosus (SLE), and in principle, BCMA deficiency in the context of SLE might reduce the number of pathogenic autoreactive long-lived plasma cells and thereby attenuate SLE phenotype.33,34 Several recent studies have also documented the expression of BCMA in malignant as well as normal plasma cells and have shown that B cell activating factor belonging to the TNF family (BAFF) signaling through BCMA can result in myeloma cell proliferation in vitro. Taken together, these studies suggested that BCMA is commonly expressed in myeloma and signaling through BCMA may also contribute to the expansion of myeloma cells in vivo and 1 candidate antigen for immunotherapies of multiple myeloma is BCMA. 35
In the current study, the performance of BCMA expression results was measured by calculation of the AUC. The data suggest that BCMA could be a powerful diagnostic biomarker for CVID patients with very high sensitivity and specificity.
According to the results of our study and others, it is confirmed that BCMA plays an important role in the survival of plasma cells and its reduction could act as an important factor in reducing plasmablast cells. Thus, it could be considered as one of the important factors causing CVID and also as a discrimination biomarker helping to diagnose CVID.
In our previous study, we also performed exon sequence analysis of BCMA in the same group of CVID patients to find any mutation. The results did not show any mutations associated with CVID disease. 36 The results of that study were consistent with results of 3 previous studies in Japanese, European, and Greek patients with CVID.32,37,38 This indicates that reducing BCMA expression in CVID patients shown in the current study might be due to probable mutations in regions such as the promoter of BCMA gene. However, this requires a separate study. On the other hand, given that the present study is the first study that shows decreased BCMA expression in patients with CVID without any mutations in its coding area, epigenetic factors such as miRNAs might have a role in lowering the expression of BCMA in CVID patients compared with normal individuals.
One reason for decreasing BCMA expression could be due to defective signaling in B cells of CVID patients. Recently, we demonstrated in another study that there is a defect in phosphorylation of Akt in B cells of CVID patients. 39 Since it has been indicated that Akt could contribute to regulation of BCMA expression in B cells, 40 defective Akt activation could be involved in decreased BCMA expression.
In conclusion, our data showed decreased plasmablast cell count and decreased BCMA expression level in CVID patients that confirm the importance of BCMA in development of CVID. In addition, BCMA expression could be considered as a new diagnostic biomarker for CVID.
Footnotes
Acknowledgments
This work was financially supported by Acquired Immunodeficiency Research Center (Grant No.: 293267), Isfahan university of Medical Sciences. The authors wish to thank all the participants, especially patients, for their generous help in this project, with special thanks to Sanaz Afshar and Faeze Abbasi for their help in gathering some clinical information.
Author Disclosure Statement
No competing financial interests exist.