
Abstract
To date, Penicillium marneffei infection has mainly been reported in adults infected with human immunodeficiency virus (HIV); only a limited number of cases have been reported in children. The aim of the article is to study the clinical and laboratory characteristics of P. marneffei in pediatric patients without HIV infection. In this study, the medical records of 10 pediatric patients with P. marneffei infection at Guangzhou Women and Children's Medical Center were evaluated from May 2011 to November 2015. The duration of symptoms before admission ranged from 8 days to 1 month. Fever was found in all 10 patients. Hepatomegaly and splenomegaly were found in 9/10 and 8/10 patients, respectively. Two patients presented with skin lesions. The main life-threatening complications during hospitalization included hemophagocytic syndrome (8/10), acute respiratory distress syndrome (8/10), disseminated intravascular coagulation (DIC) (7/10), and septic shock (6/10). Two of the 10 patients had underlying immunodeficiencies characterized by an absence of IgG and decreased CD4 and CD8 cell counts, respectively. Phagocytosis in the bone marrow was observed in four patients. Eight patients had abnormal chest radiographs. Only two patients showed remission after treatment. The others died of multiple organ failure and DIC on days 1–17 of hospitalization. Our analysis suggests that P. marneffei infection is a severe disease causing high mortality even in infants and children without HIV. Pediatric clinicians should be vigilant in identifying this disease to ensure an early diagnosis and good prognosis. A systematic approach to immunological evaluations in pediatric patients with the disease is required. Further research is necessary to explore the pathogenesis of and appropriate therapy for this infection.
Introduction
P
Materials and Methods
Patients
This report is based on the clinical data of 10 pediatric patients with P. marneffei infection who were admitted to Guangzhou Women and Children's Medical Center from May 2011 to November 2015. All patients came from endemic areas and were diagnosed with P. marneffei infection by positive blood or bone marrow culture. The study was approved by the Ethics Committee of Guangzhou Women and Children's Medical Center, Guangzhou Medical University.
Methods
We collected and analyzed data on all patients' epidemiological and clinical manifestations; laboratory test results; immunologic status; positivity for P. marneffei infection by direct smear, culture, or histopathology; clinical course, treatment and reaction to therapy; and prognosis. In addition, bone marrow samples were obtained from all patients by needle aspiration and bone marrow smears.
Results
Clinical features
Five boys and five girls ranging in age from 3 months to 3 years were analyzed. All patients were from different regions within Guangdong province. Two had developed recurrent respiratory infections, while three had malnutrition. The duration of symptoms before admission ranged from 8 days to 1 month. Most patients were diagnosed immediately after admission, and the longest duration of admission to diagnosis was 12 days. No seasonal or yearly variation in the frequency of P. marneffei infection was detected. The main clinical symptoms were fever, coughing, weight loss, and diarrhea. Fever was found in all patients. Hepatomegaly was found in 9/10 patients, and splenomegaly was found in 8/10, but the degree of each varied among the patients. The patients' clinical characteristics are summarized in Table 1. Two patients (Patients 5 and 6) presented with skin lesions characterized by pustular eruption and central umbilication (Fig. 1), respectively, and only one patient had muguet. Life-threatening complications during hospitalization included hemophagocytic syndrome (HPS) (8/10), acute respiratory distress syndrome (ARDS) (8/10), disseminated intravascular coagulation (DIC) (7/10), septic shock (6/10), renal function injury (4/10), and hepatic failure (3/10). In addition, autohemolysis, hematochezia, and central nervous system involvement were observed in one patient each.

Skin lesions with central umbilication seen over the face of a child with P. marneffei infection.
Laboratory and imaging characteristics
The diagnoses were confirmed by positive blood culture of P. marneffei (Fig. 2) or infection of the bone marrow or other tissues (Fig. 3). Data extracted from the patients at diagnosis included routine blood test results, biochemical parameters, coagulation function, serum Ig level, and lymphocyte subset levels. All patients were HIV negative according to a serum specific antibody test (note that HIV RNA PCR was not performed at our hospital during the period when those patients were admitted). Various degrees of anemia (58–88 g/L) and hypoproteinemia (21.2–38.1 g/L) were detected in all patients. Thrombocytopenia was detected in most patients with cytopenia involving two or three cell lines simultaneously. Coagulopathy with a prolonged prothrombin time and/or activated partial thromboplastin time was noted in most patients.
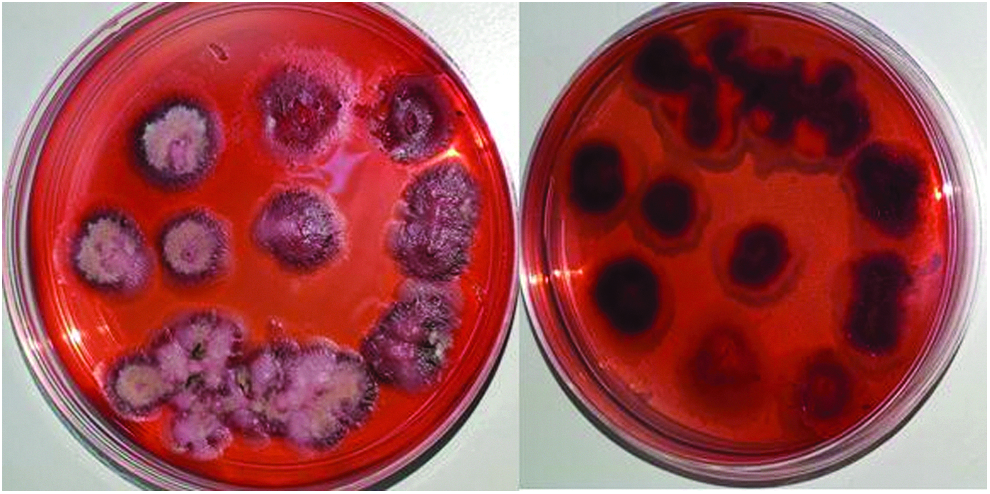
Granular colony of P. marneffei with a characteristic soluble red pigment that diffused into the agar after 7 days of incubation at 25°C.

Wright–Giemsa staining of bone marrow smear shows phagocytes engulfing P. marneffei pathogens. The pathogen exhibits a round or oval shape; a few of sausage-like P. marneffei and unstained septa can also be seen.
The laboratory findings at the time of diagnosis are shown in Table 2. Two of the 10 patients had underlying immunodeficiency; one had absence of IgG (Patient 4) and another had decreased CD4 and CD8 cell counts (Patient 8). Six patients had a documented coinfection according to blood or sputum culture, and the infective agents were hemolytic streptococcus (Patient 1), Enterococcus faecium (Patient 5), Hemophilus influenzae (Patients 5 and 6), Staphylococcus hominis (Patient 8), S. epidermidis (Patient 10), and Mycoplasma pneumoniae (Patients 5, 8, 9, and 10). Phagocytosis was observed in four bone marrow samples (Patients 1, 2, 5, and 8) (Fig. 4). Abnormal chest radiographs were also found in eight patients. Chest X-ray examination results mostly exhibited diffuse infiltration of both lungs. However, a chest scan revealed enlargement of the hilar and mediastinal lymph nodes in four patients (Patients 1, 4, 5, and 6) (Fig. 5) and interstitial pneumonia in one (Patient 1). An abdominal computed tomography scan was performed in four patients (Patients 1, 4, 6, and 9) and indicated abdominal lymphadenopathy, hepatosplenomegaly, and ascites.
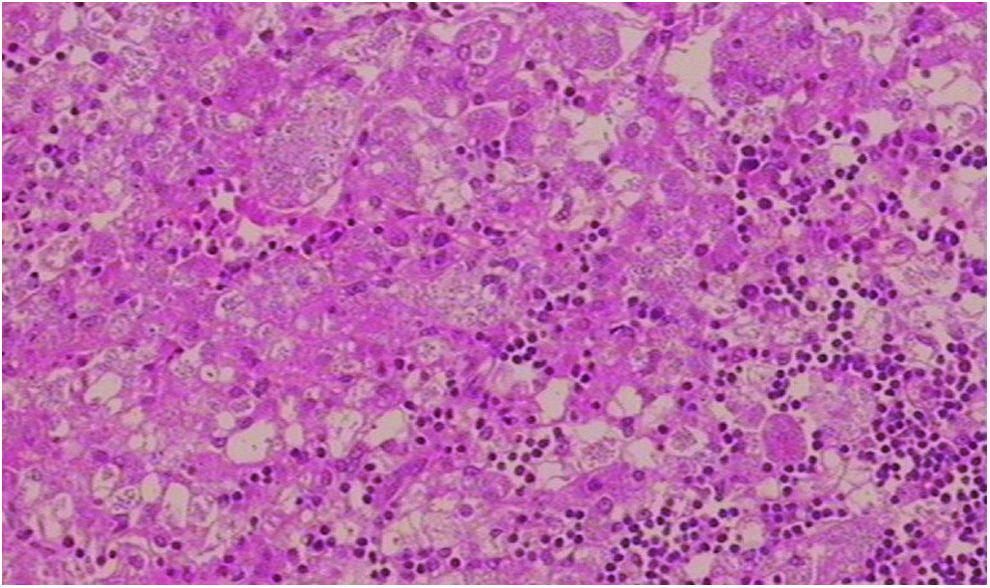
Lymph node biopsy showing histiocytic proliferation with numerous round to oblong yeast cells (hematoxylin and eosin, × 400).

Chest computed tomography scan showing enlargement of hilar and mediastinal lymph nodes (Patient 4).
Hb, hemoglobin; CRP, C-reactive protein, ALT, alanine aminotransferase; LDH, lactate dehydrogenase; PT, prothrombin time; APTT, activated partial thromboplastin time; FIB, fibrinogen; ND, not done.
Treatment and outcome
One patient (Patient 5) was misdiagnosed with tuberculosis at another hospital and received antituberculosis therapy for 3 weeks before admission to Guangzhou Women and Children's Medical Center. All patients received antibiotic treatment before hospitalization. Eight of the 10 patients received antifungal therapy (intravenous amphotericin B and/or itraconazole) because of the diagnosis of P. marneffei infection. Antifungal treatment could not be initiated for two patients because one died on the first day of admission and one died on the second day following diagnosis. All eight of these patients received immunomodulatory therapy with supportive treatment (intravenous immunoglobulin and/or plasma, albumin). Plasma exchange and continuous renal replacement therapy were performed in two patients (Patients 1 and 6). Two patients (Patients 3 and 4) showed remission after treatment, while the others died of multiple organ failure and DIC on days 1–17 of hospitalization. The length of hospital stay ranged from 1 to 67 days. Only 2 of the 10 patients survived; 1 had fungal pneumonia 1 year later, and the other was still in remission, but with excellent recovery at the time of this writing. The etiologies, treatments, and outcomes of the 10 children diagnosed with P. marneffei infection are shown in Table 3.
MP, mycoplasma pneumonia; BM, bone marrow; ALB, albumin.
Discussion
P. marneffei is an emerging pathogenic fungus that can cause fatal systemic mycosis in immunocompromised hosts and occurs mostly in humid tropical climate regions, including the south and southwest regions of China.3–5 The incidence of infection increases during the rainy seasons. The incidence has also increased in recent years in association with an increase in HIV infection among the population of China. Factors that affect transmission of the pathogen remain unclear. However, studies have suggested that exposure to conidia after inhaling infectious particles combined with heavy rainfall, which provides favorable conditions for growth of the fungus, probably increases the risk of infection.6–8 Nevertheless, the incubation period of the disease is not well defined. P. marneffei appears to disseminate to many organs through the reticuloendothelial system. All of our patients were <3 years of age, and three of them were <6 months of age. This provides evidence that primary infection can develop in toddlers and young children. The duration of symptoms before admission ranged from 8 days to 1 month and exhibited no seasonal or yearly variation. Thus, no definite timing of P. marneffei infection was identified in terms of either primary infection or reactivation from latent infection. In addition, all patients came from different regions of Guangdong province and had no history of exposure to rodents, suggesting that the infection has little regional preference within tropical China.
Because this infection has a low incidence in children, many pediatric clinicians are unfamiliar with it. The initial clinical symptoms of the disease therefore remain unclear, and both diagnostic delays and misdiagnosis frequently occur. Our findings suggest that pediatric physicians should be vigilant of identifying this disease when patients from epidemic areas are admitted with a persistent high fever that cannot be controlled by antibiotics and/or progressive loss in body weight. The diagnosis of P. marneffei infection may also be made through examination of blood, bone marrow, or other infected tissues such as lymph nodes.
We found that the main symptoms of P. marneffei infection include fever, anemia, coughing, diarrhea, and weight loss, in agreement with previous studies.2,8–10 In adult patients, skin lesions are of particular importance for rapid diagnosis of disseminated P. marneffei infection because they draw the clinician's attention; in addition, a high frequency (70%–80%) of skin lesions has been found in adult patients with disseminated disease.2,10,11 However, skin lesions were much less common among our pediatric patients. The typical skin lesion (central umbilication) occurred only in one patient. Instead, our patients presented with other symptoms involving the hematologic system, including hepatosplenomegaly, anemia, pancytopenia, and HPS. Thus, secondary HPS should also be considered as a differential diagnosis for pediatric patients. Abnormal chest radiographs were reportedly present in approximately one-third of adult patients. 2 Most of our patients (8/10) exhibited lung abnormalities; this frequency of occurrence ratio appears to be higher than that in adult patients. Seven of our patients required mechanical ventilation because of complication by ARDS. Previous reports have described the clinical courses of two pediatric patients infected with localized and disseminated P. marneffei infection. 12 Disseminated infection is much more common in patients infected with than without HIV, while localized infection is more prevalent in non-HIV-infected or immunocompetent patients.12,13 Most of our patients presented with disseminated infection, although they were not infected with HIV. In addition, most of our patients were complicated by ARDS, DIC, and/or multiple organ failure; they also satisfied the diagnostic criteria of HPS at some point during the course of the disease. This is probably why the fatality rate was very high among our patients.
Although early diagnosis is of great significance to this disease, there was a significant difference in age between cured or recovered patients and those who died of P. marneffei infection.3,9 Although our patients used antifungal therapy and immunomodulatory therapy with other supportive treatment, the fatality rate was still very high (8/10 patients died). This suggests that P. marneffei infection may be associated with higher lethality in younger infants in accordance with previous studies.12,14 However, we could not confirm that the high mortality rate was specifically due to P. marneffei infection because some patients were coinfected with other pathogens. A previous similar study reported a mortality rate of 3/7 (42.86%), 15 which was considerably lower than ours. We noted that the outbreak of their patients usually occurred in summer, while there is no seasonal variation in our case. Eight of our patients had normal immunity according to routine serologic test results, two had recurrent respiratory infections, and one had a marked elevated serum IgE level (6440 IU/mL). This might suggest that these patients could have had potentially severe underlying immunodeficiencies that were not identified or that their fatality was linked to a more systemic impairment in immunity. It appears that in the present study, the HIV-negative children with P. marneffei infection but without secondary immunodeficiencies might have had primary immune deficiencies. This is especially applicable to those patients with disseminated P. marneffei infection who died. Unfortunately, because our patients had not been approached for genetic testing and other detections of immune function such as mitogen stimulation testing, IgG subclass testing, activity of natural killer cells, and so on, we could not identify the exact cause for their death.
P. marneffei is usually seen in patients in the late stages of HIV infection with a low CD4+ cell count. Many such patients (≥80%) have a CD4+ cell count of <100 cells/μL.2,8 Because infection with P. marneffei is opportunistic, however, immune function is of great significance to its pathogenesis, especially when affected patients are HIV negative. The pathology of P. marneffei infection in different organs varies depending on the host's immunity, but the mechanisms by which P. marneffei protects itself from the host's immune defense remain unclear. Some researchers have recommended that a reduction in the number of T lymphocytes or cellular immunity is probably the most important predisposing factor to P. marneffei infection or reactivation.14,16 Notably, all of our patients were HIV negative and had no relevant family history. Instead, two children were diagnosed with primary immunodeficiency disease, which is a common disease among pediatric patients in addition to HIV infection and secondary immunodeficiency. We suggest that a possible pathophysiological mechanism of P. marneffei infection among our patients was disruption of the balance between immunological function and fungal pathogenesis. Despite the fact that one of our two survivors had primary immunodeficiency disease, we advise undertaking a systematic approach to immunological evaluations in pediatric patients with a detailed history of inherited family disease and performing a basic immunological investigation in all children with P. marneffei infection. Further research is necessary to explore the effectiveness of immunity on the pathogenesis of P. marneffei and its associated methods of therapy.
Footnotes
Author Contribution
H.F.F. and G.L.: Created the concept and design of this study. L.H. and K.Y.J.: Participated in diagnosis and collection of case data in pediatric intensive care unit (PICU). H.F.F. and W.D.Z.: Responsible for the collection of case data in department of respiration. C.C. and H.W.J.: Performed the experiments. H.F.F., L.H., and G.L.: Drafted, revised, and edited the article. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.