
Abstract
Clinical features of atopic dermatitis change with age as skin homeostatic mechanisms develop. In some cases, symptoms persist from childhood to adult. In early childhood, the characteristic features of this disease are eczema or exudative papules accompanied by itching. After childhood, lichenified dermatitis preceded by severe itching is the major skin manifestation. Presumably, this difference in clinical symptoms between childhood and adulthood may derive from the age-specific physiological function of skin, such as maintenance of proper stratum corneum, secretion of lipids, and perspiration. The volume and composition of secreted lipids and sweat change with age; these changes affect water retention, skin surface pH, and the microbiome. These physiological activities do not follow a hierarchy, but instead are coordinated to harmonize the maintenance of skin homeostasis. Thus, daily skin care based on the characteristic age-specific physiological function of skin should be considered to manage atopic dermatitis. The usage of moisturizers contributes to reduce skin dryness and the incidence of atopic dermatitis, and is recommended immediately after bathing. A water temperature of 38 to 40 degrees during bathing can be beneficial for barrier recovery, and gentle detergents or soap should be chosen if necessary. After exercise, excess sweat on the skin surface should be rinsed off. Avoidance of perspiration-inducing activities is not necessary. High temperature and humidity on skin surface may cause the development of miliaria and subsequent anhidrosis. Wearing hygroscopic and breathable underwear is recommended.
Physiological Function of Skin in Childhood
T
Skin barrier function
Pediatric skin plays an important role in thermoregulation and protection against external physical or chemical stimuli. 4 Infants born at full term have immature skin with incomplete barrier function. This immaturity of the skin barrier allows the penetration of specific external substances and allows newborns to accumulate outside information and adapt to their environment. 5
Despite its immaturity, the infant skin barrier can prevent leakage of water and also has the ability to retain water. Transepidermal water loss (TEWL) is maintained at low levels due to low perspiration. This is because, although infants possess mature sweat glands (∼2 to 5 million of sweat glands/individual), their ability to perspire is not activated at birth. Infants gradually activate their sweating ability by crying or temperature adaptation. Eventually, infants exhibit a minimal sweating ability 6 (Fig. 1).

Relationship between the characteristic distribution of atopic dermatitis and the maturation of perspiration ability with age. In early infancy, eczema frequently localizes the face, trunk, and extremities. In childhood, both eczema and lichenified dermatitis tend to localize to the neck, cubital fossa, and popliteal fossa. In early infancy, immature sweating ability possibly contributes to the widespread distribution of eczema. From birth to 36 months of age, the ratio of active sweat glands to perspiration ability is fluid. This instability renders the maintenance of skin homeostasis difficult. As the ability to perspire matures, skin surface pH decreases, and the distribution of dermatitis is concentrated in the sweat-collecting flexor surfaces of joints.
However, the TEWL value tends to be high in infants born before 32 weeks of gestation. This phenomenon may derive from their immature barrier function, thin epidermis, and increased peripheral blood flow. 6 The TEWL volume in immature infants can be up to 30% of their body weight. With maturation, the TEWL value gradually decreases. TEWL values are varied in each body area. Ordinarily, the TEWL value is higher on the face than the trunk, and is especially high in the nasolabial area and around the lips. Thus, the skin around the mouth may be susceptible to irritants or allergens. This characteristic is commonly observed from early infancy to childhood. 7
After birth, the skin is exposed to air rather than amniotic fluid for the first time. This drastic change in the humidity of the environment affects the water retention of the stratum corneum. The water retention capacity of infant skin impacts its elasticity, flexibility, and the development of the mature stratum corneum. Gradual maturation of the eccrine sweat glands compensates this susceptibility to skin dryness. As a result, water retention by the skin continues to increase until 90 days after birth and will decrease to adult levels 1 year after birth. 8
pH of pediatric skin
The pH of infant skin is almost neutral (6.5–7.5), due to the higher pH of amniotic fluid, insufficient normal moisturizing factors (NMF), immature microbiota, and immature enzymatic activation cascades.9–11 During the first 2 days after birth, the skin surface pH starts to decrease, reaching 4.5–6.0 after 3 months.8,12 Therefore, skin surface pH is unsettled, changeable during this period, and contributes to the increased susceptibility of the skin barrier toward disruption (Fig. 1).
Acidification of the skin surface is maintained by several processes, such as skin lipid synthesis and sweat secretion. Synthesized free fatty acids, derived from the cleavage of intrinsic phospholipids by phospholipase A2 and from the hydrolysis of triglycerides in sebaceous lipids by bacteria, play an important role in skin acidification.13,14 De novo synthesis of free fatty acids may be affected by the ceramide or filaggrin content and the lactate acid-related content in sweat.13,15
The acidification of skin results in not only decreased susceptibility to infection but also in the proper functioning of pH-responsive enzymes to formulate the corneocyte lipid envelope, and to regulate the proper peeling of unnecessary stratum corneum by controlling pH-sensible serine proteases.16,17
Skin Dryness and Utility of Moisturizer
As mentioned above, early infants have immature skin barrier function and exhibit skin dryness. Such symptoms are apparent in infants with “atopic diathesis.” In recent years, a mutation in the filaggrin gene, which is thought to be related to the disease ichthyosis vulgaris, has been found in a small subset of patients with atopic dermatitis. 18 Filaggrin plays an important role in the maturation and maintenance of skin barrier function. Filaggrin is derived from the serine protease-mediated cleavage of profilaggrin in keratohyalin granules, and the cleaved product, the filaggrin peptide, bundles keratin filaments in the corneocyte to maintain the strength of the cell. Further cleaved products of filaggrin become NMF, and contribute to water retention in the stratum corneum. Thus, a genetic decrease in filaggrin expression results in fragility and dryness of the stratum corneum. 19
On another front, the corneocyte lipid envelope, consisting of free fatty acids, ceramides, and cholesterol, also contributes to strength and moisture retention in the stratum corneum. 20 In atopic dermatitis, an abnormal ratio of corneocyte lipid components, such as decreased ceramides, is involved in barrier dysfunction.
The use of moisturizers can compensate for impaired barrier function in atopic dermatitis, contribute to preventing water loss or pathogen penetration, and increase the water retention capacity of the stratum corneum.21,22 The use of moisturizer from early infancy has been found to decrease the incidence of atopic dermatitis. 23 Several moisturizers exist and can be functionally divided into those that aid protection and water retention; these moisturizers cover the skin surface and capture water, respectively. The moisturizer should be chosen based on the patient's skin condition and the patient's perception of its texture to increase their adherence. For example, Vaseline is frequently chosen to shield the damaged skin barrier, and is useful to avoid the unfavorable impact of washing or rinsing repeatedly with or without detergents. Vaseline is hard to remove from skin using hot water, because of its melting temperature of 38°C–60°C; thus, it prevents the loss of skin lipid during hand washing, showering, and bathing. 24 However, its sticky texture sometimes decreases patient motivation to use it. A moisturizer-mimicking corneocyte lipid envelope has been found to decrease skin inflammation. 25 Interestingly, topical cholesterol application attenuates hapten-induced contact hypersensitivity by maintaining the expression of 11β-HSD1, which converts corticosteroids from an inactive to active form, in keratinocytes. This unique function of cholesterol may contribute to the merit of using the moisturizer-mimicking corneocyte lipid envelope, and leads to the notion that topical cholesterol application may be better than the use of topical corticosteroid to treat mild skin inflammation. 26
Moisturizers are recommended after bathing, at waking up, and every time patients experience skin dryness. 22 Children sometimes play with sand and thereby lose moisture from their hands, and are recommended to use moisturizers after playing. The volume of moisturizer recommended is as much as will stick to the skin when applied.
Management of Exacerbating Factors in Pediatric Atopic Dermatitis
Management of exacerbating factors is important not only to prevent the spontaneous flare up of disease but also to prevent the progress of allergy.21,22 There are several exacerbating factors in atopic dermatitis, and they change with age. To reduce the risk of exposure to allergens in living spaces or in the work place, cleaning and maintaining cleanliness are important. 22 Because scratching the itch causes wounding of skin and aggravates the disease, clipping nails should be considered. Secondary bacterial infection sometimes complicates the disease, and bleach baths may be applicable in cases associated with bacterial infection. 27 Nighttime itching frequently becomes problematic, especially just before sleep, due to increased skin temperature. 28 Cooling with ice pack can help the patient fall asleep. 29 Body temperature changes with circadian rhythm during the day, increasing by degrees as the evening goes on, and decreasing during sleep as a consequence of melatonin, which is known to induce cutaneous vasodilatation, secreted from the pineal gland by means of decreased exposure to light. 28 Thus, staying awake late watching TV or electronic devices will decrease melatonin secretion and will impair both the regulation of body temperature and the quality of sleep. Regulation of life rhythm is important in the management of atopic dermatitis. 28
Food antigens comprise the characteristic exacerbating factor for pediatric patients, and are thought to be sensitized from both mucosal membrane and inflamed skin. 30 As described above, the skin around the mouth is susceptible to irritation and exposure to antigens (mainly derived from food). Eczema around the mouth should be noted and treated as soon as possible. If breast milk or food sticks to skin, these should be removed by wiping or rinsing without scrubbing.
Preventing food allergies may provide an additional advantage. A previous article reported that food allergy has been found to be a factor inducing the progress of the allergic march, and increases the incidence odds ratio of atopic dermatitis, progression from atopic dermatitis to asthma, and progression from atopic dermatitis to asthma and subsequently allergic rhinitis, to 8.7, 12.5, and 32, respectively. 31 Thus, early intervention to prevent food allergy will contribute to prevent the progression of multiorgan allergic reactions.
A diet that avoids suspected allergens has been considered as an approach for pediatric patients who have confirmed food allergy based on a positive reaction in the oral challenge test along with history, skin test, and blood testing. 21 The oral allergy test should be performed carefully by experienced experts in the case of children at risk of anaphylaxis. 21 On the contrary, to avoid malnutrition, medical staff should minimize the avoidance of foods, by determining the specific causative food.
Sweat has been considered an exacerbating factor. In providing guidance to patients, we should consider both the beneficial and harmful aspects of sweat.21,32 Sweat has important beneficial roles in the maintenance of skin homeostasis, such as regulation of body temperature, host defense mechanism, and moisturizing the skin.21,32 The heat of vaporization derived from sweat decreases body temperature. Antimicrobial peptides (eg, β-defensin, cathelicidin, dermcidin), moisturizing factors (eg, lactic acid, urea), and cysteine protease inhibition in sweat contribute to proper microbiome maintenance, water retention, and inactivation of antigens with cysteine protease activity (eg, Derp1, actinidin), respectively.33–35 Thus, if the patients are able to sweat properly, they will not need to avoid activities that cause sweating. 21 Regarding the harmful aspects of sweat, we should keep in mind that some atopic dermatitis patients perspire less compared to nonatopic subjects. To date, several articles have reported decreased acetylcholine-induced sweating in both pediatric and adult patients with atopic dermatitis.36–39 The mechanism underlying decreased sweating in atopic dermatitis has been shown to involve the obstruction of sweat flow by plugging of the sweat pore, continuous anxiety, leakage of sweat, allergic inflammation involved histamine, and autonomic nerve failure32,36,40 (Fig. 2). Thus, any treatment should relieve these skin symptoms as well as anxiety, to allow patients to sweat properly. Guidance regarding exacerbating factors should be provided carefully so as to not cause parents and patients unnecessary anxiety. Activities that induce perspiration are not harmful to children with atopic dermatitis, and these activities need not be prevented. In patients with normal sweating, leaving excess sweat on the skin surface will aggravate the disease, because the benefits of sweat will be lost with time.32,34 For instance, increased pH, loss of protease inhibition activity, and contamination from dirt or antigens on the skin surface were found in old sweat, and these factors negatively impacted atopic dermatitis.32,34 Showering or rinsing to wash away the excess sweat is recommended after activities that involve perspiration21,41 (Fig. 3). From the view of appropriate regulation of body temperature, use of underwear made from hygroscopic and breathable fabric (eg, polyester) may be better than absorbent fabric (eg, cotton). 42
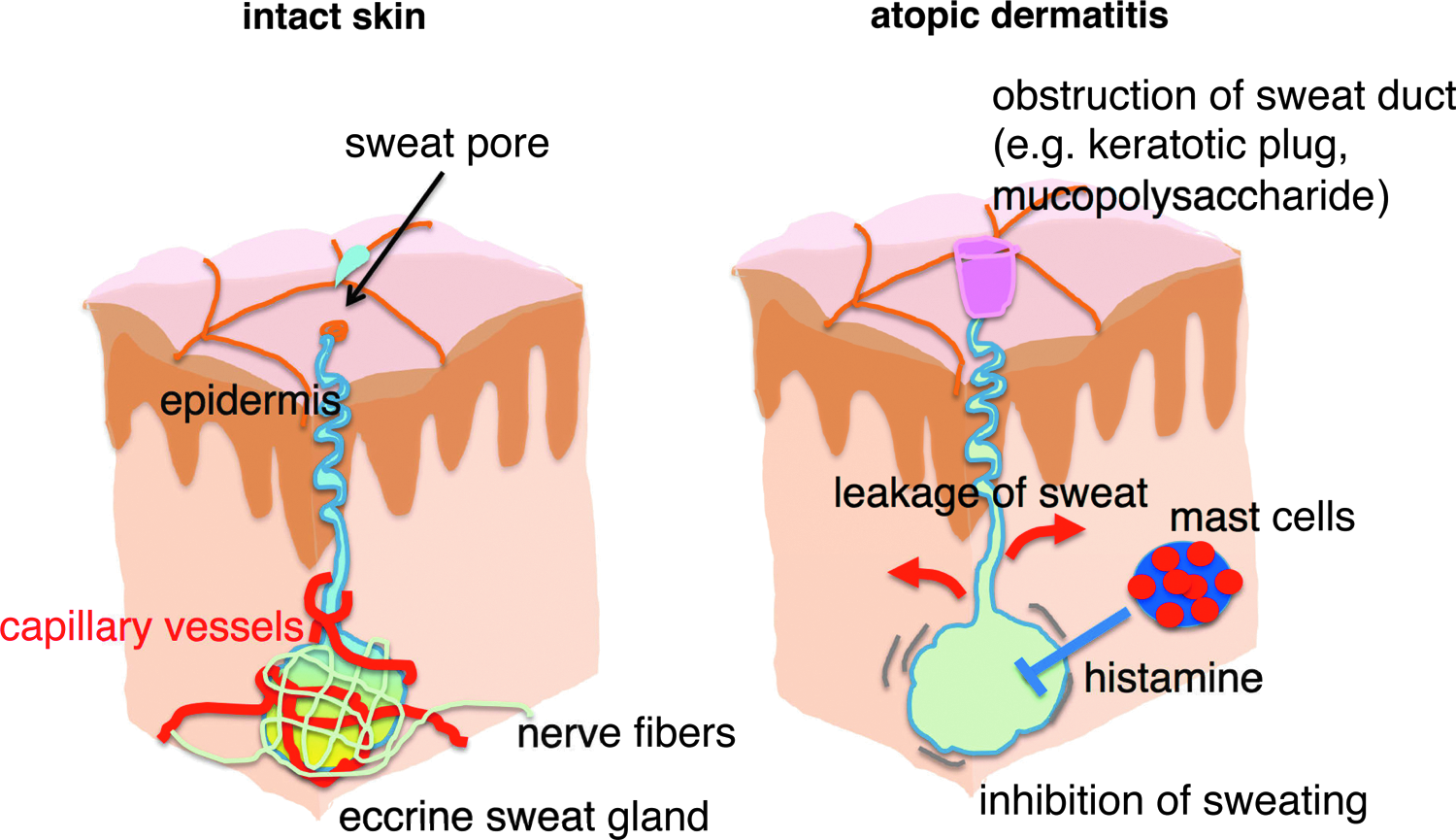
Illustration of the abnormalities of sweat glands in atopic dermatitis. In atopic dermatitis lesional skin, obstruction of sweat gland by a keratotic plug or mucopolysaccharides, leakage of sweat from the sweat apparatus into dermal tissue, or histamines have been found to contribute to decreased sweating activity.
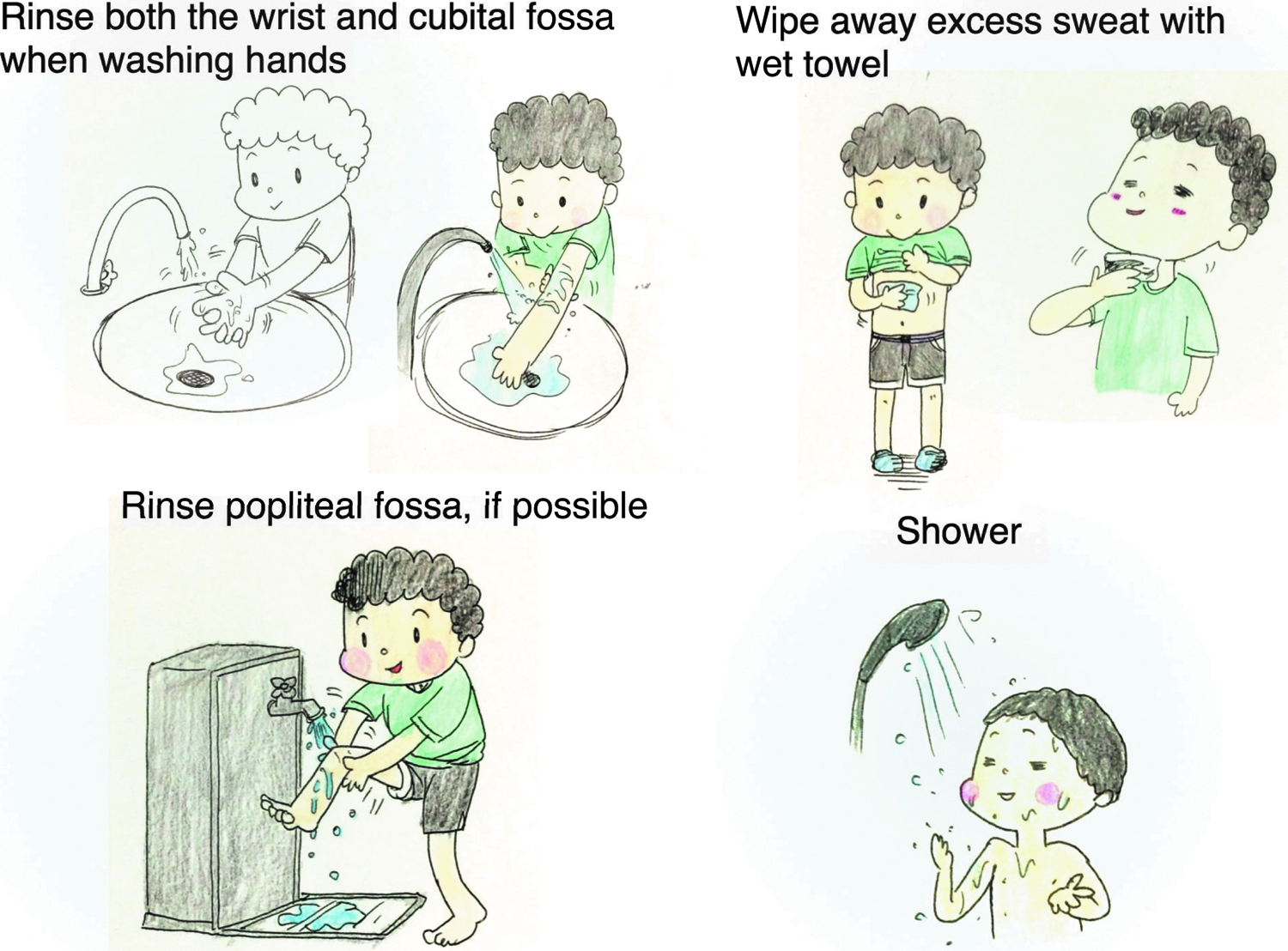
Practical visualization of how to cope with sweat in pediatric subjects with atopic dermatitis. Rinse both the affected cubital fossa and wrist under running water when patients wash their hands. If possible, rinsing the popliteal fossa is also recommended. Wipe away excess sweat with wet towel (without rubbing). Showering is also recommended to reduce the severity of atopic dermatitis.
Footnotes
Acknowledgment
The authors thank Ms. Ryoko Sugiyama for help with the illustrations.
Author Disclosure Statement
No competing financial interests exist.