
Abstract
Stress and distress have been suggested to prolong difficult-to-control asthma (DTCA), that is, asthma that is not under control despite optimal medical treatment. A pediatric pulmonologist referred a 16-year-old girl with DTCA in whom asthma-specific fear induced by disturbed memories and distorted cognitions following frightening asthma attacks were driving asthma exacerbations. We examined whether cognitive-behavioral therapy (CBT) and eye movement desensitization and reprocessing (EMDR) focusing on asthma-specific fear and disturbed memories could reduce asthma symptoms and its burden. The single-case experimental design included 48 weekly assessments of primary outcomes during all phases, and 4 assessments of secondary outcomes at intake, pretherapy, posttherapy, and follow-up. Analysis of the time series data with a piecewise regression model demonstrated that the level or slope (trend) showed an improvement during the intervention and a sustained improvement during follow-up on all primary outcomes: burden of asthma exacerbations, physical activities, social activities, physical complaints, and worrying. Analyses using the Reliable Change Index showed significant pretherapy to posttherapy changes on most domains of questionnaires measuring secondary outcomes: Asthma Control Test, Pediatric Asthma Quality of Life Questionnaire, Child Behavior Checklist, and Youth Self-Report. Moreover, use of rescue medication went down and lung function (FEV1) came just into the normal range at follow-up. The study showed that asthma symptoms and the burden of asthma were reduced after CBT and EMDR. This proof-of-principle study suggests that DTCA may improve by psychological interventions in pediatric patients with psychological stress or distress.
Introduction
A
DTCA may require a multidisciplinary approach, including thorough assessment of medical 2 and psychological 8 components. Because emotional stress may precipitate or exacerbate asthma,9,10 it has been recommended to develop and evaluate psychological intervention in children and adolescents with DTCA in whom psychological comorbidity may play a role. 11 The recent decade has witnessed surging interest in behavioral interventions that target the psychological pathways that might influence asthma. 11 Among these, education, training of breathing, stress reduction through relaxation techniques, hypnotherapy, and behavioral therapy have been found to be useful 12 and have shown a decrease in anxiety and asthma symptoms, an increase in quality of life,13–15 and a reduction in hospital admissions and length of stay. 16 In general, interventions incorporating cognitive-behavioral techniques have shown to be successful in targeting variables such as self-efficacy, self-management of disease, family functioning, psychosocial well-being, isolation, social competence, and days of absence from school17–19 in children with asthma. The only previous evaluation of the effects of cognitive-behavioral therapy (CBT) in 2 adults with DTCA indicated favorable effects, 5 as did the 1 study using self-hypnosis for anxiety in a child with severe asthma. 20 However, to decide on the usefulness of CBT for youth with DTCA and comorbid psychological stress, more evidence is needed.
“Sarah” is a 16-year-old adolescent with DTCA. She was referred to the department of pediatric psychology, because psychological stress was recognized by her pulmonologist as contributing to her DTCA. Sarah was preoccupied with and anxious of her asthma, which had led to medication overuse and deficient self-management, which appeared to play a role in the problems with controlling asthma. Anamnestic examination suggested that asthma-specific fear induced by disturbed memories and distorted cognitions following frightening asthma attacks were factors driving asthma exacerbations (Box 1).
“Sarah” is a 16-year-old Dutch girl from parents with a Mediterranean ethnic background living in the Netherlands. Asthma was diagnosed at the age of 3 years with regular exacerbations and hospitalizations. During early childhood, Sarah's asthma was not well handled by her parents and adherence to medication was poor. The past years, adherence had improved and the asthma was better accepted by Sarah and her parents.
Results of spirometry differed greatly in time from completely normal-to-severe partially reversible bronchial obstruction. Total Immunoglobulin E (IgE) was highly elevated. Specific allergy tests were highly positive to house dust mite, tree and grass pollens, and several nuts and moderately positive to a variety of other allergens. IgE against Aspergillus fumigatus was not elevated. Extended immunologic studies showed no abnormalities. Radiologic studies of the thorax showed a modest bronchial wall thickening only, without any sign of anatomic abnormalities. Her medication consisted of a combination of an inhaled steroid and a long-acting β2-agonist and a leukotriene receptor antagonist. During a long exacerbation, azithromycin and esomeprazole were added to the maintenance medication. Several trials to diminish the medication failed because more symptoms were reported and lung function declined.
At the intake, Sarah showed a lack of motivation for psychological therapy. She was convinced that only the pulmonologist could help her. Sarah was convinced of a biomedical basis of her asthma and was preoccupied with its severity. The overreaction, demonstrated by excessive worrying about symptoms of asthma, had led to medication overuse and deficient self-management, as mentioned by the pulmonologist. Frequent exacerbations and hospital admissions were part of a perpetuating cycle, including symptom hypervigilance, distress, and significant disruption of functioning for the past years, including many days of asthma-related absence from school, social isolation, and lack of social competence. Sarah had learned to fear her symptoms and had developed distorted perceptions of them. She described a preoccupation with worrying thoughts and feelings concerning her asthma and expressed anxiety about the course of her asthma and inadequate coping with asthma attacks. This was central to cycles of isolation and avoidance of pleasurable activities and anxiety, which aggravated Sarah's breathing difficulties and prevented her from leading a normal life. The illness was influencing all family members. Her overprotecting mother was extremely aware of triggers and signs of asthma exacerbations. Sarah showed difficulties in separation and individuation from her parents, which obstructed her development of independence and of adequate coping strategies. She also had a lack of knowledge about asthma self-management. She was insecure and helpless, depending highly on her mother and physician who had a leading and prescribing role.
To target Sarah's worries that she might “die of an asthma attack,” CBT was indicated. 5 Eye movement desensitization and reprocessing (EMDR) was included to treat her asthma-specific fear caused by disturbed memories.21,22 The aim of this study was to evaluate whether CBT, including EMDR, would reduce the burden of asthma and worrying in a 16-year-old female adolescent with DTCA and comorbid psychological problems. A sequential replicated single-case experimental design with multiple measurements was used for evaluation of therapy effectiveness. 23 A positive outcome of the intervention would be a proof-of-principle observation in support of the notion that DTCA may be improved by psychological means in pediatric patients characterized by comorbid psychological stress or distress.
Methods
Procedure
The study was approved by the medical ethics committee of the VU University Medical Center, Amsterdam, the Netherlands. Sarah signed an informed consent. Therapy by a licensed cognitive behavioral therapist (also qualified as an EMDR therapist) was provided for 20 one-hour weekly sessions of individual therapy within 3 phases (Table 1). EMDR was carried out on the basis of the children's protocol. 24 Box 2 presents an overview of the contents of the therapy.
Primary outcomes: 48 weekly assessments (P01–P48) with VAS.
Secondary outcomes: 4 assessments (S1–S4) with questionnaires.
ACT, asthma control test; CBCL, Child Behavior Checklist; CBT, cognitive-behavioral therapy; EMDR, eye movement desensitization and reprocessing; FEV1, forced expiratory volume in 1 second, expressed as percent of predicted (% pred); PAQLQ(S), Pediatric Asthma Quality of Life Questionnaire (Self-report); T & RP, termination & relapse prevention; VAS, Visual Analogue Scales; YSR, Youth Self Report.
Step 1: Getting acquainted, anamnesis, and explanation therapy (session 1 & 2)
The initial intake session included assessments and discussion of Sarah's goals for therapy. The second intake session was focused on educating Sarah about asthma management and psychotherapy in general, the importance of practicing and doing exercises at home, taking responsibility for change, and discussing expectations. Initially, it was challenging for Sarah to consider that physical and psychological circumstances are related. A collaborative understanding of Sarah's difficulties was developed and the intervention was based on this.
Step 2: Explaining therapy plan and motivating (session 3 & 4)
The therapy plan was explained and it was discussed what might be gained by therapy. Based on analysis of the functional relationship between situational triggers, asthma-related cognitions, and physiological fixation, cognitive-behavioral explanations were given of Sarah's asthma-specific fear and the impact of helpful thoughts on psychological well-being, physical health, and better asthma management.
Step 3: Education about asthma management and symptom discrimination (session 5 & 8)
Explanation of the nature of breathing difficulties in asthma and promoting awareness of cognitions through self-monitoring, particularly catastrophic misinterpretations of somatic sensations (symptom education). Specific instances of asthma exacerbations experienced by Sarah were discussed. Sarah was helped to recognize the consequences of different ways of personally experiencing asthma exacerbations for dysfunctional breathing. Instead of experiencing all asthma attacks as life-threatening, Sarah was taught to differentiate asthma symptoms, dysfunctional breathing, and hyperventilation. She learned techniques to remain calm in an effort to prevent anxiety-induced asthma symptoms and had a prescribed asthma management plan to use.
Step 4: Cognitive restructuring and teaching positive thoughts (session 6 & 7)
Cognitive restructuring skills were introduced to decrease Sarah's general anxiety and distress. She was taught to replace dysfunctional with functional thoughts and behavior, how to develop adaptive explanations for anxiety-provoking events, as opposed to maladaptive, self-harmful explanations, and how to manage stress.
Step 5: Relaxation exercises (session 9, 13, & 14)
The therapist taught Sarah how to respond to panic versus asthma symptoms, and how to recognize and control hyperventilation. Adequate breathing technique, postural adjustments, and relaxation techniques such as progressive muscle relaxation together with visualization of relaxing situations were taught. To reduce dysfunctional somatic preoccupation, mindfulness was taught to retrain focus of attention and concentrate on the present moment rather than worry about what might happen or about what happened before.
Step 6: Coping strategies (session 11 & 12)
Sarah was taught problem-solving skills in an effort to reduce her general level of anxiety and distress as well as her asthma-specific anxiety. Concerning her school, an overview of problems and school-related stress was made and Sarah created a better planning system.
Step 7: Response prevention and interceptive exposure (session 10 & 15)
To reduce dysfunctional safety-seeking, techniques to control exposure to anxiety and increase anxiety tolerance (response prevention) were introduced. With physician's approval, Sarah practiced relaxation skills during an asthma attack at home or school to diminish the severity and duration. Sarah practiced interceptive exposure by breathing quickly in and out of a straw until she reported experiencing some of the physical sensations of a panic attack. This exercise re-exposed Sarah to her physical sensations during an asthma attack and allowed her to endure these sensations and realize that nothing catastrophic resulted. The exercise also allowed her to practice the relaxation skills that were most effective for her. Sarah was asked to practice this exercise at home (when an adult was in the house). Asthma rescue medication was available in the session and at all subsequent practice sessions at home in the event that Sarah experienced sustained difficulty with breathing as a result of asthma; however, Sarah never needed to use the medication during the interceptive exposure exercises.
Step 8: EMDR (session 16–18)
One goal of EMDR is to alleviate negative cognition during the desensitization phase and replace it by positive cognition during the reprocessing phase. To achieve this, many aspects of Sarah's cognition were stimulated in an 8-phase approach that included having Sarah's recall distressing images, while receiving bilateral sensory input.22 The 8 phases were as follows: history taking, preparation, assessment, desensitization, installation, body scan, closure, and reassessment. Sarah had experienced 2 traumatic asthma exacerbations, at the age of 13 and 16 years. The therapist started with the asthma exacerbation at age of 13 years. In the reprocessing phases, Sarah was instructed to recognize a picture that represents the most terrible part of this asthma exacerbation and a negative unreasonable self-belief related with the picture (a negative belief currently held). Next step was to add a desired positive belief, current emotion, and physical sensation. Then, first, Sarah was guided, according to standardized protocols to simultaneously move her eyes back and forward, following the therapist's finger as they moved across their field of vision for a set of about 24–36 s. This procedure continued until the target memory was desensitized. After that, more eye movement sets were used, while Sarah was thinking of a recognized adaptive belief. This was repeated until the new belief felt good to Sarah and physiological arousal was dissipated.
Step 9: Relapse prevention and termination (session 19 & 20)
Because of Sarah's steady progress based on her report and VAS, and her wish to end the therapy, the therapy could be terminated. Two termination sessions focused on reviewing the most effective components of therapy, relapse prevention, and practicing self-skills management.
Design
To evaluate the therapy, a sequential replicated single-case experimental design with multiple measurements was used. This procedure is able to examine clinically meaningful and statistically reliable changes in outcome variables as a function of the intervention. 23 The design included 48 weekly repeated assessments of 5 primary outcomes during baseline, therapy, and follow-up phases of 16 weeks each (Table 1, P01–P48). Secondary outcomes involved self-report scores of control of asthma, quality of life, behavioral problems, and lung function measurement, measured on 4 repeated assessments at intake, pretherapy, posttherapy, and follow-up.
Instruments
Primary outcomes
Five individual outcomes indicated most important by Sarah were set during the first intake visit and monitored weekly using Visual Analogue Scales (VAS): “Asthma exacerbations” (burden of asthma exacerbations), “physical activities” (suffocative and wheezed breathing during physical activities), “social activities” (suffocative and wheezed breathing during activities with family and friends), “physical complaints” (suffering from other physical complaints), and “worrying” (worrying and being concerned and anxious).
Secondary outcomes
The Asthma Control Test (ACT) 25 assesses the control of asthma from the past 4 weeks. The patient rates 5 questions on a 5-point scale ranging from 1 (“not controlled at all”) to 5 (“completely controlled”). The items are as follows: (1) “Asthma keeps me from getting much done at work/school,” (2) “Shortness of breath,” (3) “Asthma symptoms wake me up,” (4) “Use of rescue medication,” and (5) “Patient rating of control.” The summated total score ranges from 5 to 25; a higher score reflects better control. A score of 20 or higher denotes good disease control, 15–19 partly controlled asthma, and 5–14 uncontrolled asthma. ACT scores were shown to be reliable and valid. 25
The Pediatric Asthma Quality of Life Questionnaire (Self-report) [PAQLQ(S)] 26 is a disease-specific health-related quality of life self-report measure for children and adolescents aged 7–17 years. The questionnaire assesses 3 domains: symptoms (10 items), activity limitations (5 items), and emotional function (8 items). The item range of 1–7 is reported per domain and for the whole instrument; higher scores indicate better quality of life. The Dutch PAQLQ(S) is responsive to change of asthma control and has strong measurement properties. 27
The Child Behavior Checklist (CBCL) and Youth Self Report (YSR) 28 are standardized questionnaires for assessing emotional and behavioral problems filled out by parents (CBCL) or adolescents (YSR). The CBCL and YSR consist of 120 questions. Results are expressed in a global score and scores for internalizing and externalizing behavioral problems. In all analyses, CBCL T-scores were used, with higher scores indicating more behavioral problems. The Dutch versions of the CBCL and YSR showed good reliability. 28
To assess lung function, standardized pulmonary function testing was performed using the Masterscreen (Jaeger®; CareFusion Corporation), using a standardized protocol for spirometry according to the ATS/ERS guidelines. 29 Short- or long-acting β2-adrenergic agonists were stopped 12 h before testing. Lung function parameters that were obtained and evaluated were forced expiratory volume in 1 second (FEV1), vital capacity (VC), and Tiffeneau index (FEV1/VC) before and after use of short-acting β2-agonists (Salbutamol). Even in children with severe asthma, FEV1 in between asthma attacks is often within a normal range of 80%–120% predicted. We did not assess bronchial hyperresponsiveness.
Data analysis
Several statistical techniques have been applied to analyze single-case data with as a guiding criterion that the method should complement visual analysis.23,30,31 To analyze the change in primary outcomes, we used a change-point model (also known as structural break or turning point model). Analysis consisted of estimating a piecewise regression model to the time series data. 32 Specifically, the level and slope (trend) during the baseline were compared to the level and slope during therapy and during the follow-up phase. In addition to changes in trend across the 3 phases, sudden changes were allowed when moving from one phase to another. The linear regression procedure of SPSS version 22 was used.
To evaluate the change in secondary outcomes, the reliable change index (RCI) 33 was used. The RCI expresses the change relative to measurement error. For posttherapy versus pretherapy measurements, the formula is as follows: RCI = (Xpost-therapy − Xpre-therapy)/√(2*SEM 2 ), in which X is the score before and after therapy and SEM is the standard error of measurement that can be computed knowing the standard deviation (SDx) and reliability (rxx) of a test (x), SEM = SDx √(1-rxx). An RCI larger than 1.96 reflects a significant improvement (P < 0.05).
To compute the RCIs, reliabilities (test–retest or internal consistency) and standard deviations were derived from norm population articles. For the ACT, the internal consistency reliability for not controlled asthma was α = 0.83 and SD = 4.4. 25 For the PAQLQ(S), test–retest reliability [intraclass correlation (ICC)] for Dutch adolescents aged 15–18 years was 0.66 and SD = 0.99 for the total score, ICC = 0.42 and SD = 1.22 for symptoms, ICC = 0.73 and SD = 1.25 for activities, and ICC = 0.80 and SD = 0.94 for emotions. 27 For the CBCL, r = 0.94 and SD = 10.0 for the total score was used, r = 0.91 and SD = 9.7 for internalizing, and r = 0.92 and SD = 9.5 for externalizing behavioral problems. 28 For the YSR, r = 0.87 and SD = 9.9 for the total score was used, r = 0.80 and SD = 10.1 for internalizing, and r = 0.89 and SD = 10.0 for externalizing behavioral problems. 28
Results
Primary outcomes
Figure 1 presents the weekly measurements of the 5 primary outcome variables. All 5 visual analogue scales reflected a high burden of asthma exacerbations, suffocative and wheezed breathing during physical activities and activities with family and friends, suffering from other physical complaints, and worrying and being concerned and anxious. Baseline average values ranged from 7.2 to 7.9. At the end of baseline, Sarah had an asthma exacerbation and was hospitalized for 3 days with the use of oral prednisolone.
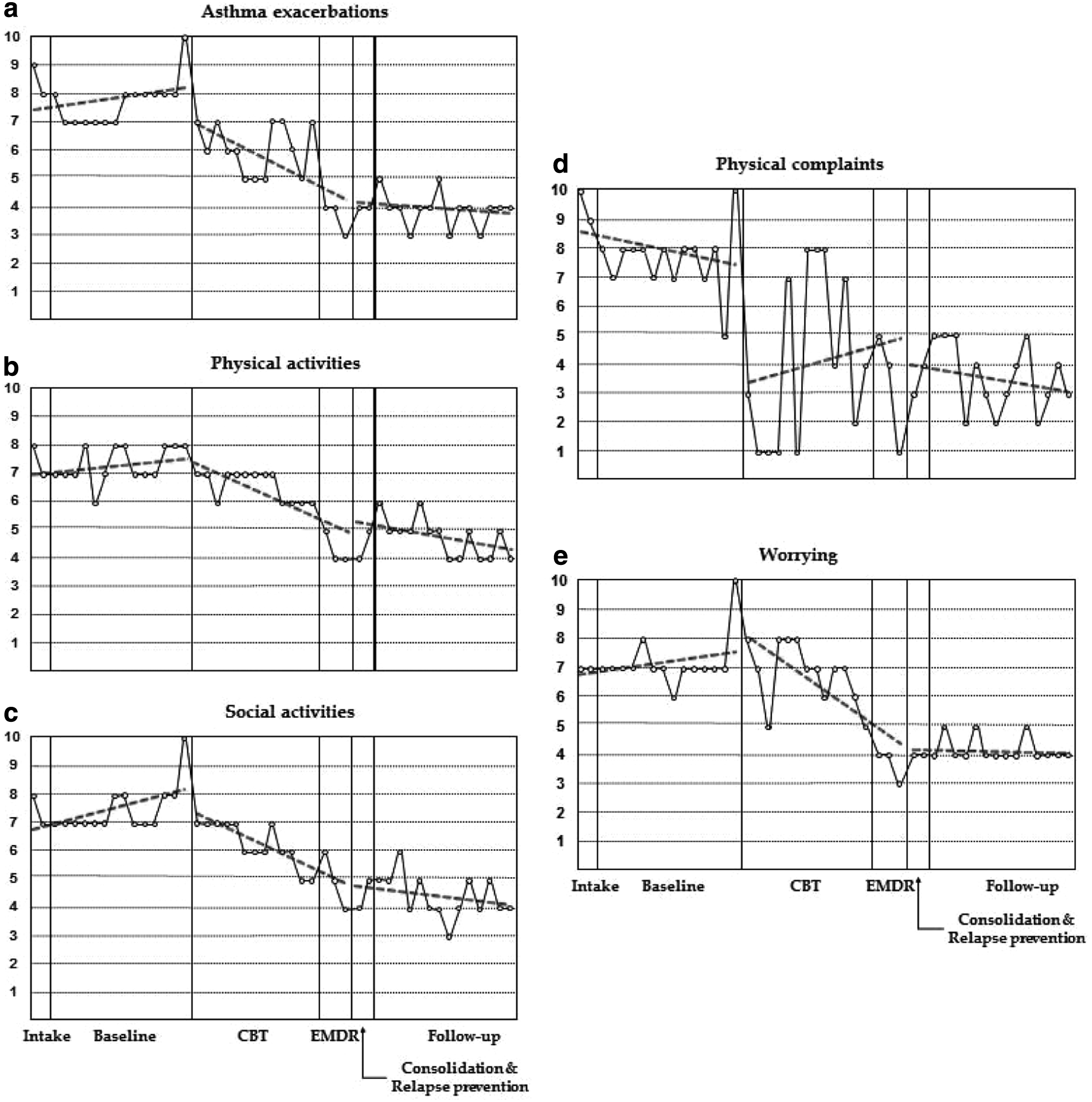
Weekly assessments during baseline, therapy, and follow-up of observed (straight line) and predicted (dotted line)
Table 2 shows the statistics of the time series analysis comparing the level and slope (trend) of the outcomes during baseline with the level and slope during and after therapy. A significant effect of “Time” reflects a linear change across 32 repeated measurements (baseline and therapy phase or baseline and follow-up phase), while adjusting for the other effects (level and slope); it is used in this analysis as a control variable to adjust for changes across time that are independent of changes within the conditions (baseline versus therapy or follow-up).
Time reflects the linear change of the outcome across conditions; level refers to differences in outcome levels between conditions; slope refers to differences in linear change of outcome levels between conditions.
The significant negative b-value for “Level” reflects that the level of the outcome during therapy or follow-up was lower than the level during baseline, while adjusting for the other effects (time and slope). A lower value of the outcome reflects improvement. The results show that the levels of 3 outcomes (asthma exacerbations, social activities, and physical complaints) were lower during therapy than during baseline and the levels of all outcome variables were lower during follow-up than during baseline.
The significant negative b-value for “Slope” reflects that the decrease during therapy or follow-up was higher than the decrease during baseline, while adjusting for other effects (time and level). Significant decreases during the intervention were observed for all outcomes, but physical complaints. During the follow-up, a further decrease was observed for physical activities and social activities. In 4 of the 5 outcome measures as shown in Fig. 1, the scores appeared to be better during the EMDR than during the CBT phase of the study. However, it is not possible to analyze whether this is a continuing effect of CBT or an effect of EMDR.
Thus, during the intervention, compared to the baseline, the level or slope of all primary outcomes reflected an improvement, while during the follow-up phase, compared to the baseline phase, all outcome levels reflected an improvement and 2 outcomes showed an ongoing positive change.
Secondary outcomes
Table 3 shows the secondary outcomes at intake, pretherapy and posttherapy, and follow-up. For example, in the first line, the scores of the ACT are shown at intake (T0), pretherapy (T1), posttherapy (T2), and follow-up (T3). The RCI at posttherapy compared to intake was −1.95 (P > 0.05) and compared to pretherapy was −2.34 (P < 0.05). The RCI at follow-up compared to intake was −1.56 (P > 0.05) and compared to pretherapy was −1.95 (P > 0.05). Thus, the ACT score significantly improved from pretherapy till posttherapy, but it did not improve further from posttherapy to follow-up. Sarah reported improvements on all items (eg, “Asthma keeps me from getting much done at work/school,” “Shortness of breath,” “Asthma symptoms wake me up,” “Use of rescue medication,” and “Patient rating of control”). However, her scores at posttherapy and follow-up were still in the uncontrolled asthma range (total score 5–15).
ACT: range 5–25; 5–14 uncontrolled asthma, 15–19 partly controlled asthma, and 20–25 controlled asthma.
PAQLQ(S): range 1–7; a higher score indicates better quality of life.
CBCL and YSR: a higher score reflects more problems (T-score ≥60 borderline clinical significant, T-score ≥63 = clinical significant).
P < 0.05 (RCI >1.96); **P < 0.01 (RCI >2.58); ***P < 0.001 (RCI >3.29).
RCI, reliable change index.
Overall, a reliable increase in all domains of quality of life [PAQLQ(S)], especially emotional functioning, was found. Also, a reliable decrease in total behavioral problems and internalizing symptoms was found at the CBCL and the YSR.
Lung function and medication
Lung function measurements (FEV1) at the 4 occasions were 73 (intake), 60 (pretherapy), 61 (posttherapy), and 81 (follow-up) % predicted. At follow-up, the value was just within the normal range of 80%–120% predicted (Table 4).
% pred, percentage predicted.
VC, vital capacity.
Inhaled corticosteroids (ICS) are the cornerstone of asthma treatment. Long-acting β2-adrenoceptor (LABA) agonists are commonly prescribed for moderate-to-severe persistent asthma patients, combined with ICS. For Sarah, during all phases, intensive medical treatment with high dosage of inhaled ICS and LABA (both twice a day), leukotriene antagonists, and antibiotic maintenance treatment remained stable. In addition, Sarah reduced daily use of short-acting β2-agonists (Salbutamol). During therapy, Salbutamol could be reduced to a maximum of 4 times a day with at least 3 h in between in comparison with the baseline phase when she used Salbutamol every hour. Sarah had no exacerbations with need for oral prednisolone during the therapy or follow-up phases, but she needed oral prednisolone against exacerbations 3 months before intake and at the end of the baseline phase.
Discussion
The hypothesis of this proof-of-principle study was that CBT, including EMDR, would be able to reduce the burden of asthma and worrying in a 16-year-old female adolescent with DTCA and comorbid psychological problems. In agreement with the hypothesis, weekly assessments of asthma symptoms and the burden of asthma showed an improvement after CBT and EMDR, focusing on cognitions and asthma-specific fear. Also, most secondary outcomes showed an improvement. Overall, Sarah's physical health, as well as her psychosocial well-being, improved substantially.
Although asthma guidelines consider the potential role of nonpharmacological interventions in DTCA and recommend the assessment of psychological comorbidity, they do not indicate how identified psychological morbidity is best managed. 5 In adults, there is only one previous study that evaluated CBT in DTCA. “Third wave” CBT (Acceptance and Commitment Therapy; Compassion Focused Therapy) was given to 2 adults with DTCA. 5 One patient with denial of asthma severity demonstrated an improved psychological status, improved well-being, and a reduction of prednisolone and hospital admissions. The other patient with overidentification with asthma demonstrated improvements in well-being and psychological symptoms. In this study, the techniques used (especially EMDR) were different, and our patient involved an adolescent. However, both the study in adults and our study in an adolescent clearly indicate that CBT may bring relief of DTCA.
In clinical practice and research, self-reports and reports by parents, such as the ACT,25,34 are common outcome variables in the standardized and multidimensional evaluation of children with asthma. 35 In a clinical setting, spirometry and other pulmonary function tests are often used, of which FEV1 is the most frequently used index for airway obstruction. However, in children and adolescents, even in severe asthma, FEV1 is often within a normal range of 80%–120% in between asthma attacks. In this study, FEV1 of Sarah had improved to a level that was just in the normal range at follow-up, giving some indication of improvement. Using a 9% change in predicted FEV1 as a significant change with responsivity to short-acting β2-agonists, Sarah showed an improvement at follow-up. A clear indication of improvement of asthma was given by the significantly reduced daily use of short-acting β2-agonists and prednisolone during therapy, and follow-up without hospital admission. The improvement during intervention and sustained improvement during follow-up on all primary outcomes were convincing. Unfortunately, our design did not allow to statistically verify an additional effect of EMDR on top of the effect of CBT. However, during this specific combination of CBT and EMDR, our results showed a progressive, beneficial course of asthma symptoms and the burden of asthma in this adolescent with DTCA and psychological comorbidity.
All secondary outcomes showed significant improvement. However, although Sarah's control of asthma improved as measured by the ACT, her asthma remained in the uncontrolled range according to the norms of this test, 25 showing that CBT did not heal her DTCA. Both quality of life (especially emotional functioning) and behavioral problems, (especially internalizing behavioral problems) showed a significant improvement. Unfortunately, when children and adolescents with asthma and severe psychological problems are presented to primary care and emergency departments, treatment often focuses on medical management only, which leads to medication overuse and increased admittance to hospital, 20 especially in children who overreact emotionally to the symptoms of asthma. 36 Therefore, it is important to identify and treat psychological problems in DTCA. This study and a previous study 37 support the recommendation that psychological evaluation and intervention should be considered early in the course of management of a patient with DTCA because it may help avoid unnecessary overmedication and investigation, and it may yield rapid improvement in the patient's clinical condition.
Our study did not examine why anxiety and stress can exacerbate asthma. In response to stress and anxiety, the hypothalamic-pituitary-adrenal (HPA) axis and the autonomic nervous system (ANS) are commonly activated and these variables may be critically involved in asthma as well. Children with asthma who simultaneously experienced stress showed marked reductions in glucocorticoid receptor mRNA (HPA) and β2-adrenergic receptor mRNA (ANS), 9 and stress was associated with ANS variables that may underlie airway obstruction in asthma.9,38 To the extent that reduction in glucocorticoid receptor mRNA reflects diminished sensitivity to the anti-inflammatory properties of glucocorticoids and the reduction in β2 adrenergic receptor, mRNA reflects a reduction of bronchodilatory properties of β-agonists, this physiological process might play a role in resistance to therapy in patients with difficult-to-treat asthma and comorbid stress. Inclusion of physiological stress variables in experimental studies can test this notion.
Our study design has strengths and limitations. A strength is the use of a single-case experimental design with multiple repeated measurements, which allowed to thoroughly evaluate the effects of the intervention. However, this study does not more than offering a proof-of-principle demonstration. Replication in more cases is needed to offer empirical support to the recommendation to consider these psychological interventions in pediatric patients with DTCA characterized by psychological stress or distress. Another limitation inherent to assessment in asthma is the lack of objective measures of asthma exacerbations outside the hospital and the need to rely most on reports of exacerbations by the patient. Self-reports are subject to recall and other forms of biases. A potential way to obtain an indication of asthma exacerbations at home using repeated objective measures is to continuously assess oxygen saturation, heart rate, and respiration with ambulatory devices. However, this would be very cumbersome in a study that lasts such a long time. Moreover, in the specific case in our study, not the real occurrence of exacerbations appeared to be the problem, but perceiving any instance of shortness of breath as an exacerbation was the core problem for which she was treated with CBT.
This single-case study suggests that a psychological intervention customized to the individual psychological comorbidity is beneficial to adolescents with DTCA. A realistic option for future research is a design with small groups using multiple repeated measures as in this single-case experimental design. A sufficiently powered randomized controlled trial customized to individual patients with DTCA and with as severe psychological comorbidity as in the case of Sarah is only possible if multiple centers participate.
Conclusion
Our study tested the notion that psychological problems related to asthma attacks may prolong DTCA. It was shown that asthma symptoms and the burden of asthma were reduced after CBT and EMDR. Therefore, this proof-of-principle study suggests that DTCA may be improved by offering a psychological intervention to pediatric patients who are characterized by psychological stress or distress.
Footnotes
Acknowledgments
This study was partially supported by an unrestricted gift from the Dutch foundation “Vrienden van de S.T.E.A.” We thank the patient and her parents for their cooperation, Eric Haarman, PhD, pediatric pulmonologist of the VU University Medical Center Amsterdam for his valuable advise, Anita Beelen, PhD, for helping with the design of the study, and Ellen Hamaker, PhD, for help with statistical analysis.
Author Disclosure Statement
No competing financial interests exist.