
Abstract
Poor socioeconomic circumstances and poverty are perceived to be barriers to successful home ventilation. Pediatric home ventilation has escalated rapidly in high-income countries but is underreported and underfunded in low-middle income countries. A retrospective chart review covering the past 20 years was carried out at the Red Cross War Memorial Children's Hospital in Cape Town, South Africa, a low-middle income country. Data collection included demographics, socioeconomic and family factors, clinical information, and ventilation-related information. Fifty-five children received home ventilation between 1994 and December 2015 from a median age of 3.5 years (range 0.4–17.6). Thirty-nine (71%) children received invasive ventilation and 16 (29%) children received mask-assisted ventilation. Most common primary diagnosis was a neuromuscular disease (60%). Twenty-six children (47%) were still on home ventilation in December 2015, 8 (15%) had been weaned off ventilation, and 21 (38%) had died. Median time between initiation of ventilation and discharge was 15 days (range 1–52) for mask-assisted ventilation and 88 days (8–991) for tracheostomy-assisted ventilation. Of the total 40 readmissions in the first year of home ventilation, 34 (85%) were emergency readmissions mainly necessitated by respiratory infections (n = 26; 65%). Despite a high prevalence of socioeconomic challenges, 89% of the children were successfully discharged on home ventilation. Main cause of death was acute infections (n = 11; 52%). Pediatric home ventilation in South Africa is feasible despite difficult socioeconomic circumstances. Survival outcome was comparable with that of high-income countries. However, a high level of psychosocial support and interventions is needed.
Introduction
I
Pediatric home ventilation has mainly been reported from high-income countries, where its use is on the rise.5–10 Based on the overall experience, it can be concluded that home ventilation is feasible.5–9 In contrast, home ventilation is rarely reported from low or middle-income settings with limited access to expensive medical equipment, expertise, and diagnostic modalities such as polysomnography (PSG). A study from Serbia of 29 children nevertheless concluded that home ventilation was feasible under low socioeconomic circumstances. 11
South Africa is a middle-income country with a wide distribution of wealth, which results in a wide range of socioeconomic circumstances and inequality. The South African healthcare system has parallel and separate public and private healthcare systems. There is a maldistribution of healthcare resources between the public and private sectors, on a geographic basis and between levels of care. 12 Private providers and private insurers still predominantly serve the minority higher and middle income population, leaving the public sector to serve the lower income majority. 12 The overall poverty rate is estimated at 11%, with marked socioeconomic inequality across racial and geographical divisions. 13 Approximately 23% of the economically active age group (15–64 years) are unemployed. 13 About 11% of households have no access to piped water, 40% have no access to flush toilets and waste removal, and 20% have no access to electricity. 13
The objectives of this study were (1) to describe a single-centre experience of home ventilation in children from various socioeconomic backgrounds in South Africa and (2) to retrospectively evaluate outcomes and readmissions within 1 year after discharge.
Materials and Methods
The design of the study was a retrospective chart review. The Medical Ethical Committee of Cape Town University approved the study (study number HREC REF 603/2013).
All children enrolled in the Breatheasy program of the Red Cross War Memorial Children's Hospital (RCWMCH) from January 1994 to December 2015 and receiving home ventilation, either tracheostomy-assisted or mask-assisted, were included.
The RCWMCH is a public tertiary level hospital in Cape Town, South Africa. Launched in 1989, the Breatheasy home program trains caregivers to take care of children with tracheostomies and children on home ventilation. 14 The program is run by an advanced clinical pediatric nurse-led multidisciplinary team, including a dietician, speech-language therapist, physiotherapist, occupational therapist, pediatric pulmonologist, and a social worker. 14 All equipments required for home ventilation in families without private medical insurance were acquired through private fund raising and charitable donations because of limited resources in the public sector healthcare system.
Indications and conditions for initiating home ventilation
Before 2011, children needing home ventilation were identified only through clinical presentation or clinical indications, the majority via the pediatric intensive care unit (PICU). Neonatal intensive care unit (NICU) is not provided on-site at RCWMCH, as this service is located at maternity hospitals in the drainage area. Due to resource constraints in PICU and neonatal services in South Africa, our home ventilation program does not offer long-term home ventilation in preterm infants with severe Bronchopulmonary Dysplasia (BPD). Infants with severe BPD requiring ventilation remain in NICU until they are able to be discharged home with domiciliary oxygen. Long-term ventilation was initiated either in the PICU or ward. PSG was not available at our institution until 2011 and then was only offered to patients with complex underlying medical conditions in whom sleep-disordered breathing was suspected.
As soon as it is apparent that a child requires home ventilation, a caregiver is identified, and he or she participates in decision-making and the planning process. 14 Important information such as socioeconomic circumstances, social support structures, and level of skills of the primary caregiver is assessed so that custom-made training can be provided. A home visit is conducted to gain insight into the socioeconomic circumstances of the family. After a child's condition has stabilized, he or she is transferred from the PICU to the step-down ward where training and preparation for home ventilation begins. The primary caregiver and other family members are taught step-by-step how to care for the tracheostomy tube if present. Building confidence in taking care of their child and knowing what to do if complications occur are important parts of the training. A protocol-based checklist is followed and completed by a nurse practitioner to ensure that all aspects of caregiver education, training, equipment needs, and emergency procedure are addressed before discharge home. In addition, a locally developed educational and informational booklet is provided to all caregivers. Once a child is medically stable and the caregiver training is complete, discharge home or to another institution is possible such as another hospital or a pediatric intermediate healthcare institution (a step-down facility between acute hospital and home) for children and families from poorly resourced areas. 14
Data collection
A database was completed retrospectively in December 2015 capturing data of all children participating in the Breatheasy program since 1994. These data include all demographic, socioeconomic and family factors, clinical and medical information, tracheostomy-, and ventilation-related information. Socioeconomic factors such as type of housing, level of caregiver education, substance abuse, and having sanitation and/or running water indoors or outdoors were collected. Missing and additional information was retrieved from medical records, the PICU, and the hospital electronic admissions databases.
Home ventilation commenced when children were discharged to their own home or to another institution. Patients were seen every 2 months in an outpatient clinic and outcomes were collected for 1 year after the initiation of home ventilation. For children who were still on home ventilation on December 15, 2015, the time on ventilation was calculated from start date to December 15, 2015.
Caregivers may be entitled to receive a “Care Dependency Grant” from the government, which is a noncontributory monthly cash transfer to caregivers of children with severe disabilities who require permanent care. 15 “Formal housing” is defined as brick structures and informal housing as corrugated iron structures. 16
Data were analyzed using SPSS 20. Differences between groups receiving private medical aid and no private medical aid, complete/higher schooling and incomplete schooling, and informal versus formal housing were established with the independent sample Mann–Whitney U-test. A P value of <0.05 was considered statistically significant.
Results
Fifty-five children received home ventilation between 1994 and December 2015. Twenty-six children (47%) were still on home ventilation in December 2015, 8 (15%) had been weaned off ventilation, and 21 children (38%) had died (Fig. 1). Sixteen children on home ventilation had been treated at the RCWMCH and 10 children in private practice during follow-up. The number of patients on home ventilation has yearly increased from 1994 to 2015 (Fig. 2).

Flowchart study population.

Cumulative number of children deceased, weaned, and on home ventilation 1994–2015 (n = 55).
Thirty-nine (71%) children received tracheostomy-assisted ventilation and sixteen (29%) mask-assisted ventilation. More patients were started on mask-assisted ventilation after 2010 compared to earlier years.
Table 1 summarizes the characteristics of the study group. The median age at the start of home ventilation was 3.5 years (range 0.4–17.6). Forty-eight children (87%) were born with a congenital anomaly or genetic defect. The most common primary diagnosis was a neuromuscular disease (60%).
n = 46, for nine children information is lacking.
n = 54, for one child the information is lacking.
MVA, motor vehicle accident; SMA, spinal muscular atrophy; SMARD, spinal muscular atrophy with respiratory distress.
Twenty-five children (45%) were initially intubated and ventilated as an emergency. In 34 children (62%), ventilation was initiated during PICU admission. Six of 55 (11%) patients initiated on home ventilation after 2011 had PSG before starting home ventilation. Of these, three had PSG-demonstrated hypoventilation and/or obstructive sleep apnea. The other three were started on home ventilation as they had severe underlying congenital myopathies and presented with recurrent pneumonia and atelectasis. The median time between the initiation of the ventilation in hospital and discharge from hospital was 12 days (range 5–53) for mask-assisted ventilation and 84 days (47–170) for tracheostomy-assisted ventilation.
Before 2002, children were discharged after a much longer period than in 2002 or later (Fig. 3). Children commenced on tracheostomy-assisted ventilation had a longer in-hospital stay than children commenced on mask assisted-ventilation. Exact dates of start of ventilation in hospital and discharge home were available for 55 children. Of these children, 17 had private medical aid, and for one child the information is lacking.
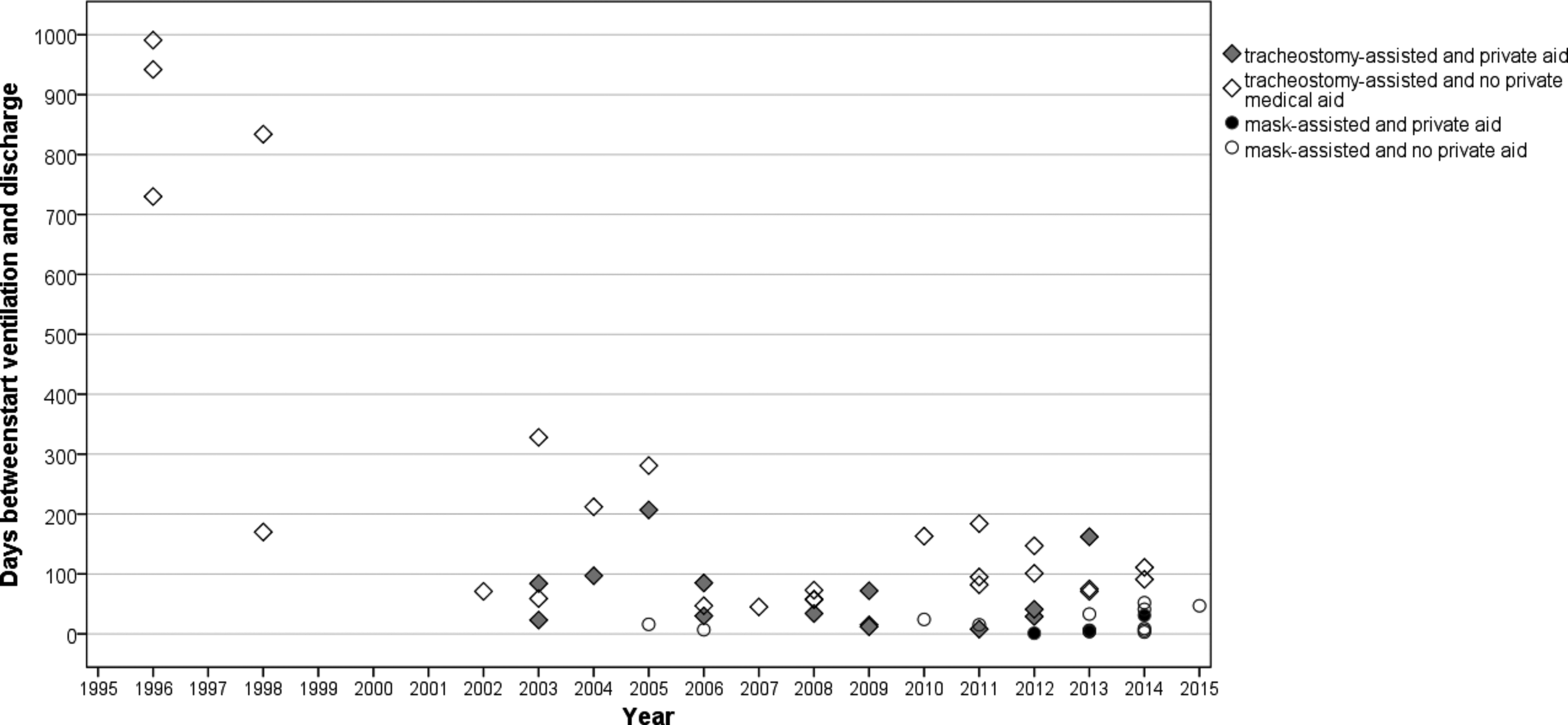
Scatter diagram; showing time from start of in-hospital ventilation to first home discharge of home-ventilated children 1994–2015 (n = 55).
Median duration between start of ventilation and discharge was not significantly different for children with or without private medical aid, [respectively, 54 days (interquartile range {IQR} 26–95)] and 73 days [(IQR 27–160), P = 0.43]. Significant difference was found between parents with incomplete schooling and those with complete or higher schooling for the median duration between start of ventilation and discharge (P = 0.002). Length of stay until discharge was 82 days (IQR 47–117) for children with parents who had incomplete schooling and 31 days (IQR 9–176) for children with parents who had complete or higher schooling. With respect to the effect of housing, it took significantly longer for children from informal settlements to be discharged on ventilation than for children in formal settlements (P = 0.02) with medians (IQR) of 95 days (58–730) versus 46 days (15–95).
Forty-two children (89%) were discharged home; the remaining 5 (11%) were discharged to an institution (n = 3) or another hospital so that they could be closer to home (n = 2).
For 18 children (33%), it was unknown whether they had been readmitted in the first year of home ventilation. Ten of them had private medical aid and were treated elsewhere, three were treated before 2000, two left South Africa, and for three this information is lacking. Twenty-two of the remaining 37 children were readmitted in the first year after discharge from 1 to 6 times (Table 2).
n = 44, for 11 children the information is lacking.
n = 43, for 12 children the information is lacking.
n = 38, for 17 children the information is lacking.
Forty readmission in the first year of home ventilation for n = 22 children.
IQR, interquartile range; PICU, pediatric intensive care unit.
In total, there were 40 readmissions in the first year of home ventilation for 22 children (7 mask-assisted ventilated and 15 tracheostomy-assisted ventilated children); 34 (85%) were emergency readmissions, the majority for respiratory infections (n = 26). The median time elapsed between the start of the home ventilation and first readmission was 71 days (range 4–362).
Twenty-one of the 55 children had died (38%), 4 children (20%) of them were mask-assisted ventilated and 17 tracheostomy-assisted ventilated (80%) (Table 1 and Fig. 1). Two had died after being weaned off the ventilator (n = 1 and n = 19 in Table 3). Main cause of death was acute infections (pneumonia, sepsis, and severe diarrhea) in 11 patients (52%). Death was attributed to progression of the underlying condition in eight patients (38%). In two patients, death was related to failure of medical equipment: in one case a power failure at the time (1994) when back-up battery supplies were not yet available. The second case concerned a sudden occlusion of the tracheostomy on a bus ride to school when no suction device was available.
SMA, spinal muscular atrophy.
Twenty-one primary caregivers (40%) were unemployed and relied on the Care Dependency Grant to provide a household income. Table 4 gives an overview of the socioeconomic background. Seven out of the nine children who lived in informal housing could be discharged home.
n = 51, for four children the information is lacking.
n = 52, for three children the information is lacking.
n = 47, for eight children the information is lacking.
CDG, care dependency grant.
Discussion
This study describes outcomes of a home ventilation program in South Africa, a low-middle-income country with high prevalence of difficult and unique socioeconomic circumstances. Objectives were to describe a single-center experience of home ventilation in children from various socioeconomic backgrounds and to evaluate outcomes and readmissions within 1 year after discharge. This study is novel in that there are few published reports of home ventilation in children from low-middle income countries. The first important finding of our study is that home ventilation is feasible despite socioeconomic challenges. The second important finding is that children on our home ventilation program were discharged home earlier in comparison to other studies.7,17 Furthermore, readmission rates at 1 year were similar to other settings.17,18
Patients on tracheostomy-assisted ventilation in our study were discharged sooner (median 84 days) on home ventilation than patients on tracheostomy-assisted ventilation reported in studies from developed countries,7,17,19 These numbers are to our knowledge not available for mask-assisted ventilation patients. Children on mask-assisted ventilation in our study were discharged after a median of 12 days.
Edwards et al. reported a median of 288 days (range 108–1,260 days) elapsed before discharge. 17 Amin et al. reported on long-term tracheostomy-assisted ventilation in 35 infants in Canada. 19 Fifteen children were discharged home directly, and 18 were moved to a rehabilitation hospital. 19 Six children were still inpatients of a rehabilitation hospital at the time of reporting. The median length of stay at the acute hospital from the time of tracheostomy insertion was 162.0 days and 97.0 days at the rehabilitation hospital, respectively.
Com et al. reported a median duration of 180 days from entry in the program until home discharge in a study of 91 children in the United States. 7 Several studies have looked at factors delaying the discharge process. One study identified funding for staffing, equipment, and local organizational delays as delaying factors. 17 Other factors found were failure to recruit qualified nursing staff for home care, unsuitable home conditions, and complex social issues.20,21 In Switzerland the majority of the children receive home care support from a qualified nurse. 21 A national survey in Italy showed that in 47% of cases, the parents are the sole caregivers of children on home ventilation, but still 40% is taken care of by a professional. 22
Most of these delaying factors are evident in our setting, too, but are dealt with in another way. Our ability to discharge patients sooner to better-resourced settings reflects the success of our home ventilation program, which relies exclusively on rapidly accessible donated equipment and the need for the caregiver to provide comprehensive care at home as home-based nursing services are not available. Comprehensive care at home is made possible by means of training the primary caregiver to take care of the child and manage the ventilation equipment without delay. As highlighted by our data, difficult socioeconomic circumstances that potentially prevent the ability to provide home ventilation are common in low-middle income settings. Innovative solutions to overcome these challenges are required, which include fundraising for equipment and actively recruiting relatives to care for a child where parents may be incapable or unreliable, for example, in the case of parental substance abuse.
The readmission rate in our program compares well to that reported elsewhere.17,18,23 The mortality rate in the study period (38%) was higher, however, than the rates reported in high-income settings (from 5% to 24%).7–10,17,18 Still, only two deaths were related to equipment failure, which is comparable to other centers. Consistent with other reports, progression of the underlying condition and pneumonia were the main causes for death in our cohort. The higher mortality in our study could be explained by a number of factors. First, the majority of children in our study were PICU survivors, thus reflecting a greater proportion of children with severe respiratory failure and complications. Second, poor socioeconomic circumstances such as lack of adequate sanitation or safe water supply are factors responsible for higher rates of infectious diseases such as pneumonia, sepsis, and diarrhea. Finally, difficulties or delays in accessing emergency services, an unfortunate reality in our setting, may have contributed to the higher mortality as suggested by the number of children who died outside of hospital. Nevertheless, given the complex and difficult socioeconomic challenges in our setting, the number of avoidable deaths due to these circumstances for the outcomes of patients on home ventilation is acceptable.
The Breatheasy program's success and achievements are attributed to early caregiver participation in the preparation and planning for long-term ventilation, which takes into consideration the unique socioeconomic circumstances of individual families. Ironically, the lack of home-based nursing care services, reported in some settings to delay discharge, permits more rapid discharge to the community in our setting. This is important in resource-constrained settings such as South Africa where high-dependency beds and PICU-beds are relatively few and in high demand. The model developed over time by the Breatheasy program thus compares favorably with recently published recommendations in the American Thoracic Society (ATS) clinical practice guidelines for chronic home invasive ventilation. 24 However, the ATS recommendation that an awake, trained caregiver should be present at all times and that at least two family caregivers should be trained specifically for the child care is not feasible in our setting in most cases. The favorable outcomes, with only two children dying because of equipment failure, reported in our cohort suggest that this recommendation may not apply in all settings.
Baker et al. recently described that implementation of a standardized discharge process for children requiring home ventilation reduces the hospital length of stay and the hospital cost. 25 This practice and policy has also been followed by our home ventilation program and is likely to be an additional factor that has contributed to the success and favorable outcomes reported in this study. The role of PSG in low-middle income countries for the diagnosis and monitoring of children who require home ventilation is controversial due to lack PSG in these settings. Low-cost widely available alternatives such as blood gas analysis and overnight saturation monitor are more appropriate and feasible alternatives to PSG under these circumstances. 26
The Breatheasy program's continued existence relies on donated equipment and a dedicated advanced pediatric nurse practitioner with skills and experience in tracheostomy care and home ventilation. The model adopted by the Breatheasy program of providing and sustaining home ventilation serves as an example for other low-middle income settings that face similar challenges.
A limitation of this study is that data were collected retrospectively over 20 years. Some information was missing, especially for the children treated before the year 2000 and children having private medical aids who were followed up primarily at a private institution where access to medical records was limited. Children from regional hospitals and private sector who require home ventilation are all referred to the Breatheasy program because these institutions do not offer a home ventilation program. Follow-up for these children is therefore not readily available if they return to their own hospital after completing the program. Another limitation is that this study population is not representative of all children who would benefit from home ventilation. Historically, only children surviving long-term PICU admission were offered home ventilation in our setting due to limited resources. Because of greater awareness and improved capacity to screen children at risk of sleep-disordered breathing with PSG in recent years, more patients are initiated earlier on nocturnal mask-assisted home ventilation. With time, it is likely that mask-assisted home ventilation will be more common and reflect the experience in high-income countries across the world.
Conclusion
Despite challenging socioeconomic circumstances in a low-middle income country such as South Africa, home ventilation is feasible. Children were discharged home earlier than children in studies from developed countries and the 1-year readmission rate was comparable to those studies. Successful home ventilation in low-middle income countries is dependent on resources such as the Breatheasy program, which provides comprehensive caregiver training, education, and equipment to make home ventilation possible.
Footnotes
Author Disclosure Statement
No competing financial interests exist.