
Abstract
A bridging bronchus (BB) is an aberrant bronchus that is commonly associated with congenital cardiac and great vessel anomalies. We describe a rare case of a BB in a pediatric patient without complicated congenital cardiac and great vessel anomalies. Bronchoscopy and 3-dimensional reconstruction computed tomography may be useful in recognizing this rare airway malformation. Antibiotics, mucolytic, and mechanical vibration sputum expectoration treatments were recommended during episodes of respiratory infection. Slide tracheoplasty is an appropriate technique if the respiratory status deteriorates.
Introduction
T
Case Details
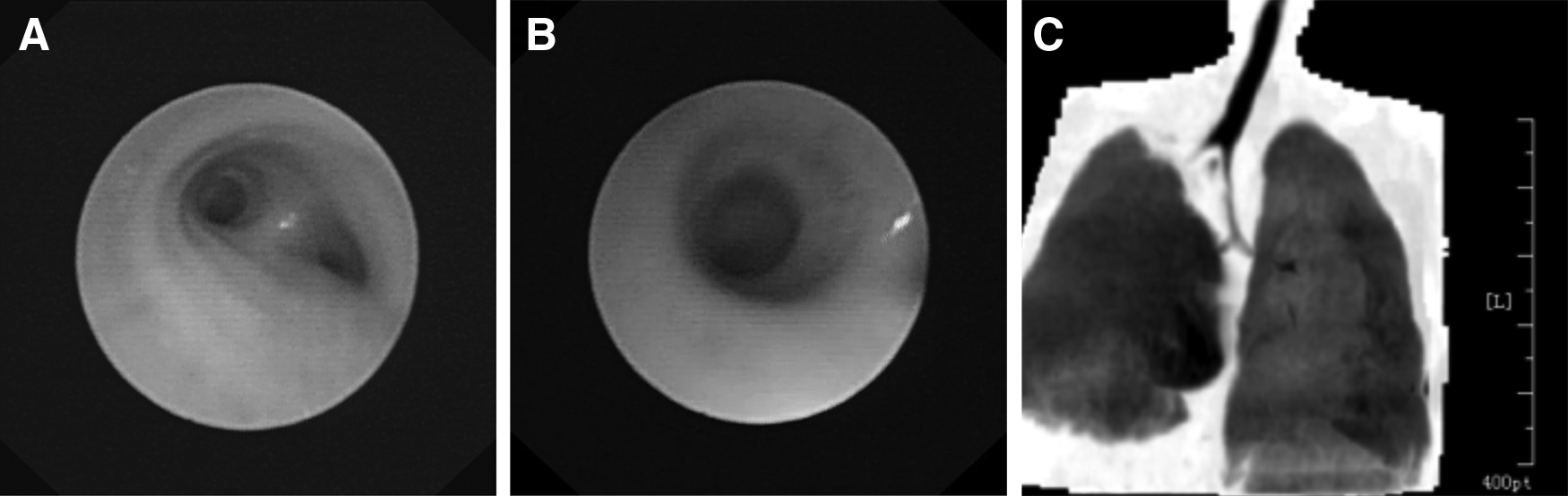
A 3,030 g female infant was delivered at term. At 4 h of age, she was hospitalized in the neonatal intensive care unit for wheezing, inspiratory stridor, and dyspnea. A chest X-ray showed generalized bilateral patchy infiltrates. Laboratory test results were significant for an elevated white blood cell count (WBC). A diagnosis of neonatal pneumonia was made. The patient was discharged after 7 days of antibiotic treatment. At 2 months, she was again hospitalized for wheezing, inspiratory stridor, and cough. The findings on chest X-ray and elevated WBC supported a diagnosis of bronchopneumonia. The patient was treated with bronchodilators, inhaled corticosteroids, and antibiotics. She recovered and was discharged after 9 days. At the age of 8 months, the patient was admitted to our hospital for wet cough, inspiratory stridor, and respiratory distress at rest and was again diagnosed with bronchopneumonia. Based on her medical history of several hospitalizations involving recurrent respiratory symptoms and respiratory infections, further diagnostic workup was initiated to determine a possible underlying etiology. Bronchoscopy showed the presence of stenosis of both the left and right mainstem bronchi, with an “O-shaped” tracheal cartilage in the left mainstem bronchus. Chest CT displayed bilateral diffuse ground glass opacity, patchy shadows, and stenosis of the left and right main bronchi. A 3-dimensional reconstruction of the tracheobronchial system revealed BB (Fig. 1). The BB originated from the left mainstem bronchus at a level of T6 and supplied the right lower and middle lobes. The trachea divides into 2 bronchi (right upper lobe bronchus and left main bronchus) at the level of T4-5_(true bifurcation). Echocardiography, abdominal ultrasonography, enhanced CT of the chest, and otolaryngology examination were performed to exclude associated anomalies. Aside from the aberrant tracheobronchial system, there were no other malformations detected. Treatment with bronchodilator inhalations and intravenous antibiotics was initiated for 2 weeks and combined with mucolytic treatment and mechanical vibration sputum expectoration. The infant recovered and was discharged home with instructions to follow-up in outpatient clinic. Antibiotics, mucolytic treatment, and mechanical vibration sputum expectoration were recommended during episodes of respiratory infections. She has grown appropriately in the first year of follow-up without further intervention.
Discussion
BB is a very rare anomaly that was first reported in 1976 by Gonzalez-Crussi et al. The most common BB variant is a large bronchial branch that originates from the left mainstem bronchus and crosses the mediastinum to supply the right lower and middle lobes. Frequently, BB occurs in conjunction with congenital cardiac and great vessel malformations, especially with SLPA and atrial septal defect (ASD). Hagl et al. 5 described a 4-year old child with SLPA, ASD, and BB as already mentioned. Baden et al. 6 reported bronchography and 3-dimensional CT of a female newborn that revealed an abnormal bronchus originating from the left mainstem bronchus and supplying the right lower lobe that was associated with an SLPA and ASD. Wells et al. 7 reported a case similar to that seen in Baden's report. 6 Our patient had a comparable bronchial malformation; however, there were no associated malformations of the cardiac and great vessel system, nor of the skeletal and gastrointestinal systems.
In the normal airway, the angles of the right mainstem bronchus and left mainstem bronchus are 30° ± 5° and 51° ± 9°, respectively. The carina is located at the level of T4-5. Although the carina is located at a normal position in patients with BB, the angles of the right mainstem bronchus and left mainstem bronchus are both increased (65 ± 5° and 61 ± 5°, respectively). The BB coursed more horizontal, leading to the “inverted T” pattern.8,9 In a review of BB by Schnabel et al., 10 5 types of BB were identified. The most common type is the BB that creates a large bronchial branch originating from the left mainstem bronchus. The second most common type is the BB that is a stenotic bronchus between the right upper lobe bronchus and the carina. A third BB type is a large bronchial branch originating from the right mainstem bronchus. A fourth form occurs when a third bronchus (BB) originates from the carina on the right side and crosses the mediastinum to the right lower lobe. The fifth form is the BB that arises from the left main bronchus at a level of T6-7 to supply the right lung with a concurrent upper lobe bronchus that is a bud. Almost all reported cases of BB occur with tracheal stenosis. For patients with BB and severe tracheal stenosis, tracheoplasty may be required to relieve some of the respiratory symptoms.6,11 The prognostic factors for BB include the severity of the stenosis and whether there are additional anomalies (eg, univentricular heart, hypoplastic right lung, esophageal atresia, and anal atresia; VACTERL syndrome). Patients with isolated BB usually have a relatively good prognosis.10,12 Seven patients have been identified postmortem with multiple malformations.4,7,13–16 Factors associated with poor prognosis include (1) multiple severe malformations, (2) limited medical resources and treatment options, and (3) failure to diagnose (Table 1).
VACTERL syndrome: vertebral anomalies, anal atresia, cardiac anomalies, tracheoesophageal fistula (TEF), renal anomalies, limb anomalies.
ASD, atrial septal defect; SLPA, sling left pulmonary artery; VSD, ventricular septal defect.
Isolated BB is rare, anomalous bronchial branching without other associated malformations. Most of the children in previously described cases presented with symptoms of lower airway obstruction and recurrent respiratory tract infections.10,12 Diagnosis of this rare malformation may be missed if no further diagnostic procedures are performed. In this patient with BB, the trachea divided into 2 bronchi (right upper lobe bronchus and left mainstem bronchus) at the level of T4-5_(true bifurcation). The BB arose from the left mainstem bronchus at the level of T6-7 (pseudocarina). 8 Bronchoscopy alone may miss the diagnosis of BB if the pseudocarina is not recognized. In addition, if the junction of the BB within the left main bronchus is misinterpreted as the true bifurcation, the right main bronchus may be mistakenly classified as a tracheal bronchus. Despite these potential pitfalls, bronchoscopy remains a valuable tool in the assessment of tracheal and bronchial stenosis and is a powerful method to evaluate the presence or absence of cartilage rings. Three-dimensional reconstruction CT is an excellent tool to demonstrate the structural abnormalities of the aberrant tracheobronchial system and to detect any anomalous great vessels that may also be present. 9 In addition, a complete cardiac evaluation is important. Echocardiography allows further assessment for associated intracardiac malformations.
Patients diagnosed with BB commonly present with recurrent respiratory tract infections. Antibiotics, mucolytic, and mechanical vibration sputum expectoration treatments are often recommended during episodes of respiratory infection. Controversy exists regarding the benefit of bronchodilators. Reports by Stokes et al. 17 as well as by Topcu et al. 11 support symptomatic improvement after bronchodilators, whereas Schnabel et al. 10 did not show a significant improvement.
CT scan imaging and bronchoscopy are the important techniques for both surveillance and diagnosis during episode of respiratory infections. CT scan imaging is a noninvasive and short acquisition time imaging technique that is sufficient to establish a reliable diagnosis of airway stenosis and pneumonia. 9 Radiation exposure is always a consideration in making imaging decisions in children. Bronchoscopy is a powerful method to dynamically evaluate the tracheobronchial system and cartilaginous rings. In this circumstance, bronchocoscopy served both as a diagnostic and therapeutic modality. Some challenges in bronchoscopy in infants and children with BB include (1) need for sedation, (2) respiratory distress may complicate the procedure, and (3) smaller bronchoscopes may be necessary in cases of tracheobronchial stenosis. 18
Although BB is commonly associated with tracheal stenosis, those who are asymptomatic do not require additional interventions. However, if the patient's respiratory status deteriorates, slide tracheoplasty can be considered. Huang et al. 19 described the use of tracheoplasty to solve the problem of stenosis on both the BB and the distal main bronchi. Their patient was not readmitted for respiratory symptoms during the first year of follow-up. Hagl et al. 5 reported a similar surgical technique to solve the problem of stenosis of a long segment of the trachea associated with SLPA and BB. Slide tracheoplasty has become one of the preferred techniques to solve the problem of long-segmental tracheal stenosis. 20 Younger patients were at increased risk for complications with slide tracheoplasty. In high-risk cases, bronchoscopic balloon dilation may be considered as a temporizing option.
Conclusion
We report the diagnosis of BB in a female infant by utilizing both bronchoscopy and 3-dimensional reconstruction CT of the tracheobronchial system. BB is a rare tracheobronchial anomaly that commonly presents with signs of pediatric lower airway obstruction or recurrent respiratory tract infections. Diagnosis of BB will likely be missed without further diagnostic workup. Patients diagnosed with BB frequently have concomitant cardiac anomalies (ASD, ventricular septal defect, SLPA) and tracheal stenosis. Diagnosis of BB often requires a combination of different diagnostic modalities, including (1) bronchoscopy to perform the initial assessment of the aberrancy of the tracheobronchial system (including recognition of areas of airway stenosis and complete cartilaginous rings), (2) 3-dimensional reconstruction CT of the tracheobronchial system to delineate the anatomical relationship of the structural abnormality, (3) echocardiography to assess for cardiac malformations, and (4) enhanced CT examination of the chest to detect possible great vessel anomalies. Careful follow-up with judicious use of antibiotics, mucolytics, and airway clearance techniques during respiratory infections will be continued. Slide tracheostomy will be considered if the infant's respiratory status deteriorates.
Footnotes
Acknowledgments
Informed consent was obtained from the child's parents. The authors wish to thank the parents for allowing us to discuss and present this case.
Authorship and Contribution
Y.D. drafted the first version of the article, L.Q. was involved in conception and design, and acquisition of data, and F.Y. made critical revision to the article and added important intellectual content.
Consent to Participate
Informed consent was obtained from the parents of the child.
Author Disclosure Statement
No competing financial interests exist.