
Abstract
In this study, it was aimed to compare the levels of serum endocan with commonly used markers, and also to define the suitability for determination of disease severity in patients with community-acquired pneumonia (CAP). The study included 60 patients and 28 healthy subjects. Pneumonia severity was determined according to British Thoracic Society guidelines for the management of CAP in children. Serum levels of endocan and C-reactive protein (CRP) and white blood cell (WBC), and neutrophil count were measured. Serum endocan levels were increased in patients with CAP. CRP levels, WBC count, neutrophil count and neutrophil lymphocyte ratio were also higher in the CAP group than healthy control group. Endocan was correlated with CRP and WBC count and disease severity. For the identification of CAP, the area under the receiver operating characteristic (ROC) curve of CRP was acceptable for CRP, but not for endocan (0.812 and 0.649, respectively). ROC analysis for endocan to differentiate between severe CAP (n = 29) and mild–moderate CAP (n = 31) gave an area under the curve of 0.769 compared to 0.667 for CRP. Serum endocan levels increase in patients with CAP and can therefore be a useful marker in diagnosis and as a particular indicator of the treatment in the clinical assessment of CAP disease severity. Serum endocan levels of patients with severe CAP were higher compared with patients with mild–moderate CAP. These results revealed that endocan might be a useful indicator of severity of CAP.
Introduction
C
Early diagnosis and determination of disease severity can reduce mortality and morbidity by creating a timely and optimal opportunity for appropriate antibiotherapy.3,4 White blood cell (WBC) count and C-reactive protein (CRP) are current commonly used laboratory data in the diagnosis and follow-up of CAP. However, the sensitivity and specificity of these diagnostic markers are low especially in the determination of disease severity. 1
Endocan, also known as endothelial cell-specific molecule-1, is a proteoglycan that is expressed in the lung and kidney endothelial cells. Its synthesis and secretion are mediated by proinflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin (IL)-1β.5–7 Endocan binds to the integrins known as leukocyte function-associated antigen (LFA)-1 and inhibits their binding to intercellular adhesion molecule-1, thus causing deterioration of the LFA-1-associated leukocyte functions. 8 The result is impaired leukocyte adhesion to endothelial cells and prevention of excessive leukocyte accumulation in the lungs. 9 The central role of leukocytes and endothelial dysfunction in CAP 10 led to the hypothesis that endocan could be used in the diagnosis of CAP and for determination of CAP disease severity.
The aim of this study was to determine the levels of serum endocan in children with the diagnosis of CAP, compare it with the control group, and examine its relationship with commonly used markers such as CRP, WBC, and neutrophil count. It was also aimed to investigate whether serum endocan levels differ or not in accordance with the disease severity.
Materials and Methods
Patients
Approval for this prospective study was granted by the Local Ethics Committee. The study included 60 children aged 3 months to18 years who were diagnosed with CAP on admittance to the Department of Pediatrics, Health Practice and Research Hospital, Faculty of Medicine, Namik Kemal University, between June 2015 and March 2016. Informed consent was obtained from all the parents. The diagnosis of CAP was made from clinical signs and symptoms according to the British Thoracic Society guidelines for the management of CAP in children, and patients were divided into 2 groups of mild–moderate and severe. 1 The demographic characteristics, comorbidities, and signs and symptoms of the patients were recorded. Patients with severe malnutrition, cystic fibrosis, chronic lung disease, chronic kidney disease, inflammatory and/or immunosuppressive diseases, or a history of hospitalization in the 14 days previous to the onset of symptoms were excluded from the study. A total of 28 healthy children were enrolled in the study as the control group.
Sample collection
Peripheral blood samples were taken from the patient and control groups at the time of admission. Whole blood samples were centrifuged for 5 min at 3,000 rpm and serum samples were separated. Serum CRP levels were measured immediately with the turbidimetric method in Cobas c 501 Biochemistry device. Sera were stored at −86°C for measurement of endocan levels. Blood samples were withdrawn into ethylenediaminetetraaceticacid-containing tubes for complete blood count and an automated blood cell counter was used for the analyses (Pentra DX Nexus-DF).
Endocan assay
Serum endocan levels were measured with the LSBio ELISA Kit (Life Span Biosciences, Inc.). The intra-assay and interassay variabilities of the ELISA kit were 3.7% and 4.6%, respectively. The minimum detectable dose of endocan was 10 pg/mL.
Statistical analyzes
All data were analyzed using the Statistical Package for the Social Sciences for Windows software (Version 18.0; SPSS). The Shapiro–Wilk W test was used to identify whether the variables were normally distributed. The differences between groups were assessed using unpaired t-tests for parametric data and the Mann–Whitney U-test for nonparametric data. Correlations between variables were evaluated with Pearson's correlation coefficient. Where individual correlations achieved statistical significance, variables were entered into a linear regression model. Receiver operating characteristic (ROC) curve analysis was used to define the power of endocan to identify diagnosis of pneumonia. A value of P < 0.05 was accepted as statistically significant.
Results
The data of the patients studied are presented in Table 1. No statistically significant difference was determined between the CAP and control groups in respect of age. The mean values of inflammation markers, WBC and neutrophil count, neutrophil–lymphocyte ratio (NLR), and CRP levels were higher in the CAP group than in the control group (P < 0.001, P < 0.01, P < 0.01, P < 0.001, respectively).
Parametric data presented as mean ± standard deviation and nonparametric data presented as median (min–max).
P < 0.001, **P < 0.01.
CAP, community-acquired pneumonia; CRP, C-reactive protein.
Serum endocan levels were higher in the patient group than in the control group [143.17 (47.44–467) ng/mL versus 96.12 (32.5–189.3) ng/mL, P < 0.01] (Table 1). When subjects with CAP were categorized according to disease severity, the differences became more marked, revealing significantly higher endocan levels in severe CAP subjects compared with mild–moderate CAP subjects [181.03 (65–467) ng/mL versus 107.75 (47.44–305) ng/mL, P < 0.001]. As inflammatory parameters, WBC, neutrophil, and lymphocyte count and NLR were higher in severe CAP cases than in mild–moderate cases, but not at a statistically significant level (P > 0.05 for all). In the severe pneumonia group, CRP levels were determined to be statistically significant (P < 0.05) (Table 2).
Nonparametric data presented as median (min–max).
P < 0.05, **P < 0.001.
In the CAP group, serum endocan levels significantly correlated with CRP (r = 0.330; P < 0.01) (Fig. 1), WBC (r = 0.534; P < 0.001) (Fig. 2), and disease severity (r = 0.433; P < 0.001). CRP was significantly correlated with WBC (r = 0.406; P < 0.001), neutrophil count (r = 0.538; P < 0.001), disease severity (r = 0.263; P = 0.042), and NLR (r = 0.690; P < 0.001).
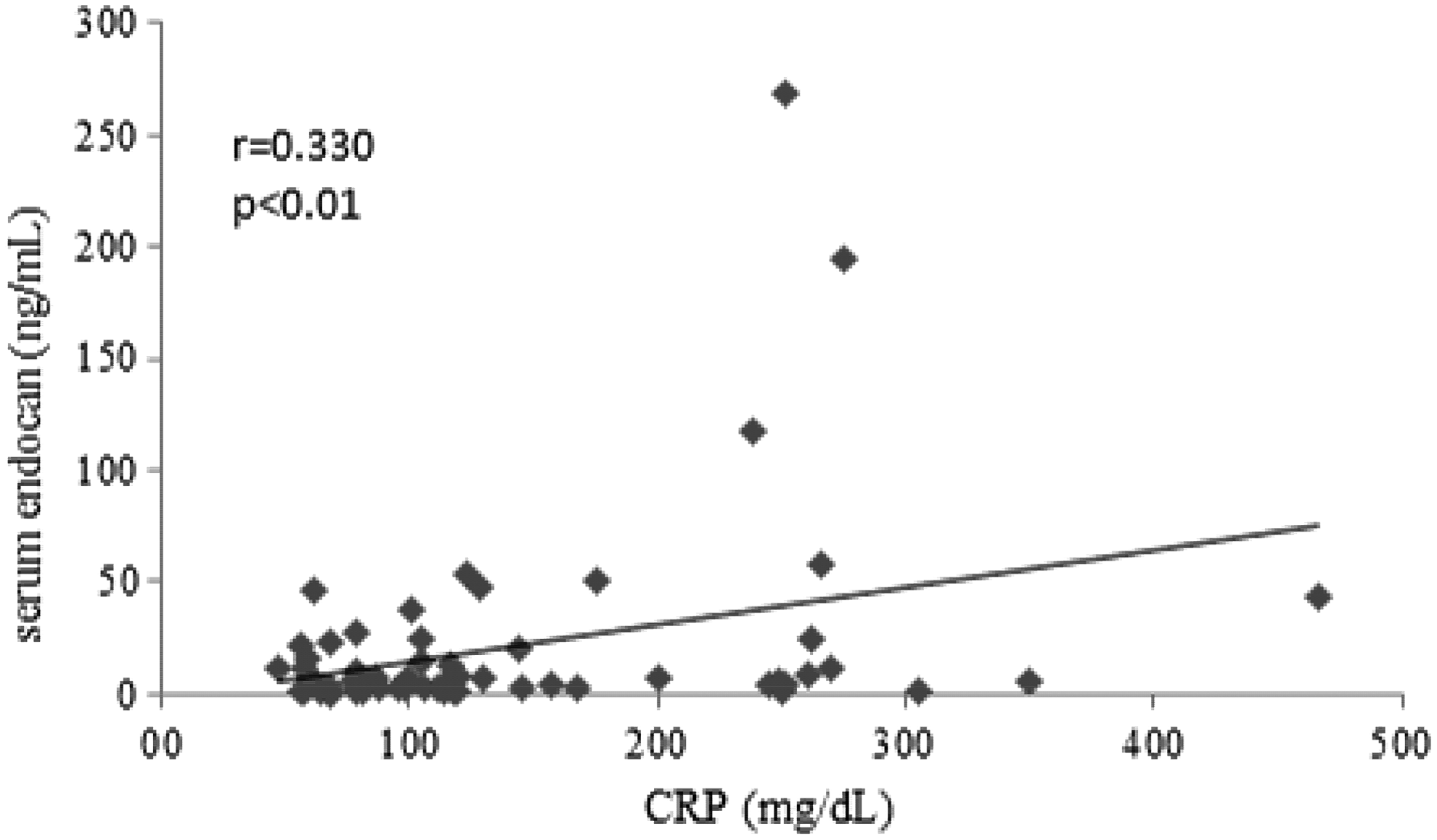
Correlations of serum endocan with C-reactive protein in CAP. CAP, community-acquired pneumonia.
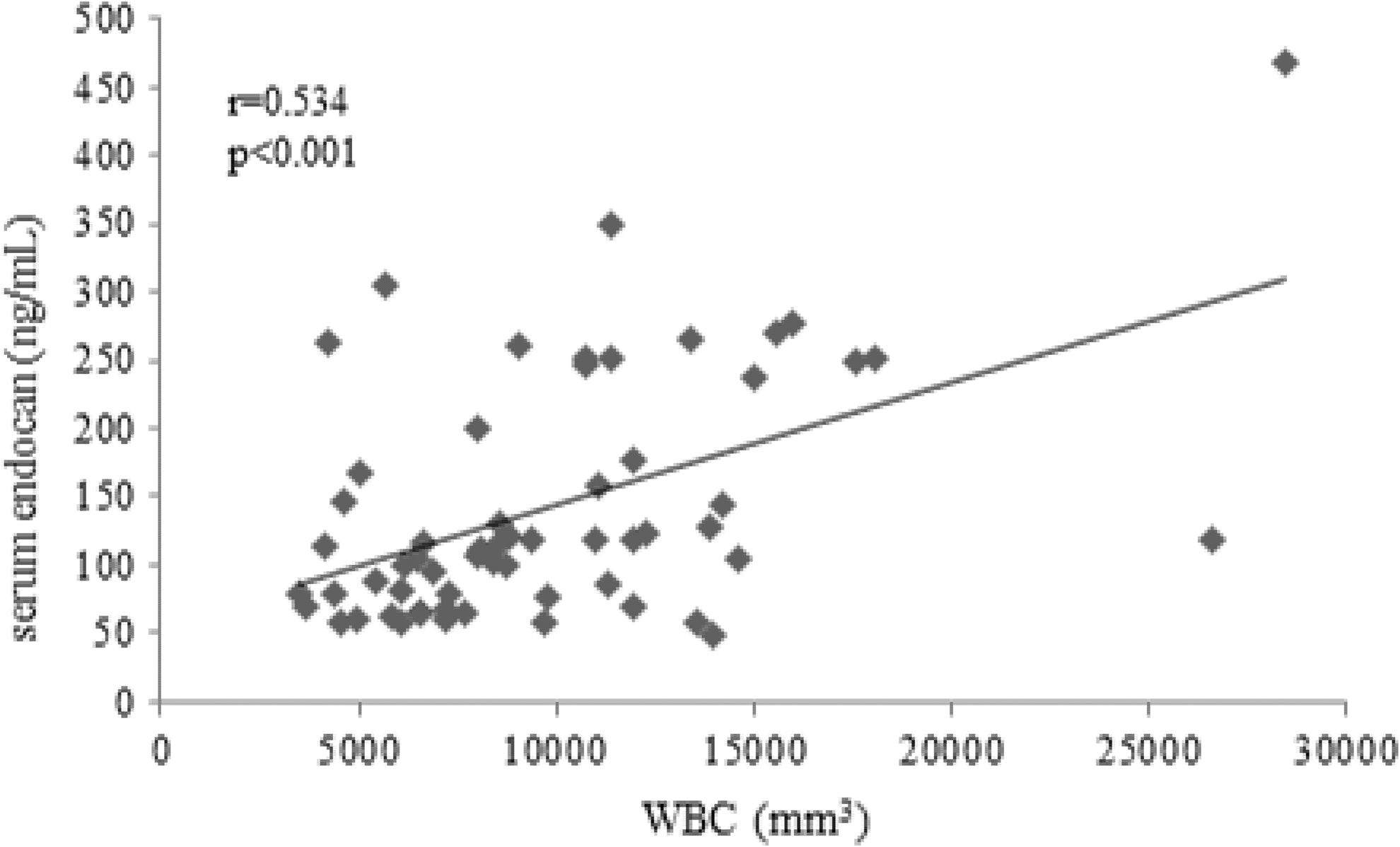
Correlations of serum endocan with white blood cell in CAP.
When ROC curve analysis was applied to analyze the suitability of endocan, CRP, WBC, and neutrophils to identify CAP, the area under the curve (AUC) for CRP was found to be acceptable (AUC = 0.812). The AUC for endocan was not found to be acceptable in the CAP versus control group (AUC = 0.649) (Fig. 3). When ROC curve analysis was used to analyze the suitability of endocan to identify severe CAP, the AUC for endocan was found to be significant (AUC = 0.769) (Fig. 4). The cutoff point for the prediction of intolerance was determined as 162.91 ng/mL with a sensitivity of 43.3% and specificity of 96.4%. The CRP level and WBC and neutrophil count were determined to be below the acceptable limit for the differentiation of disease severity (AUC <0.700).
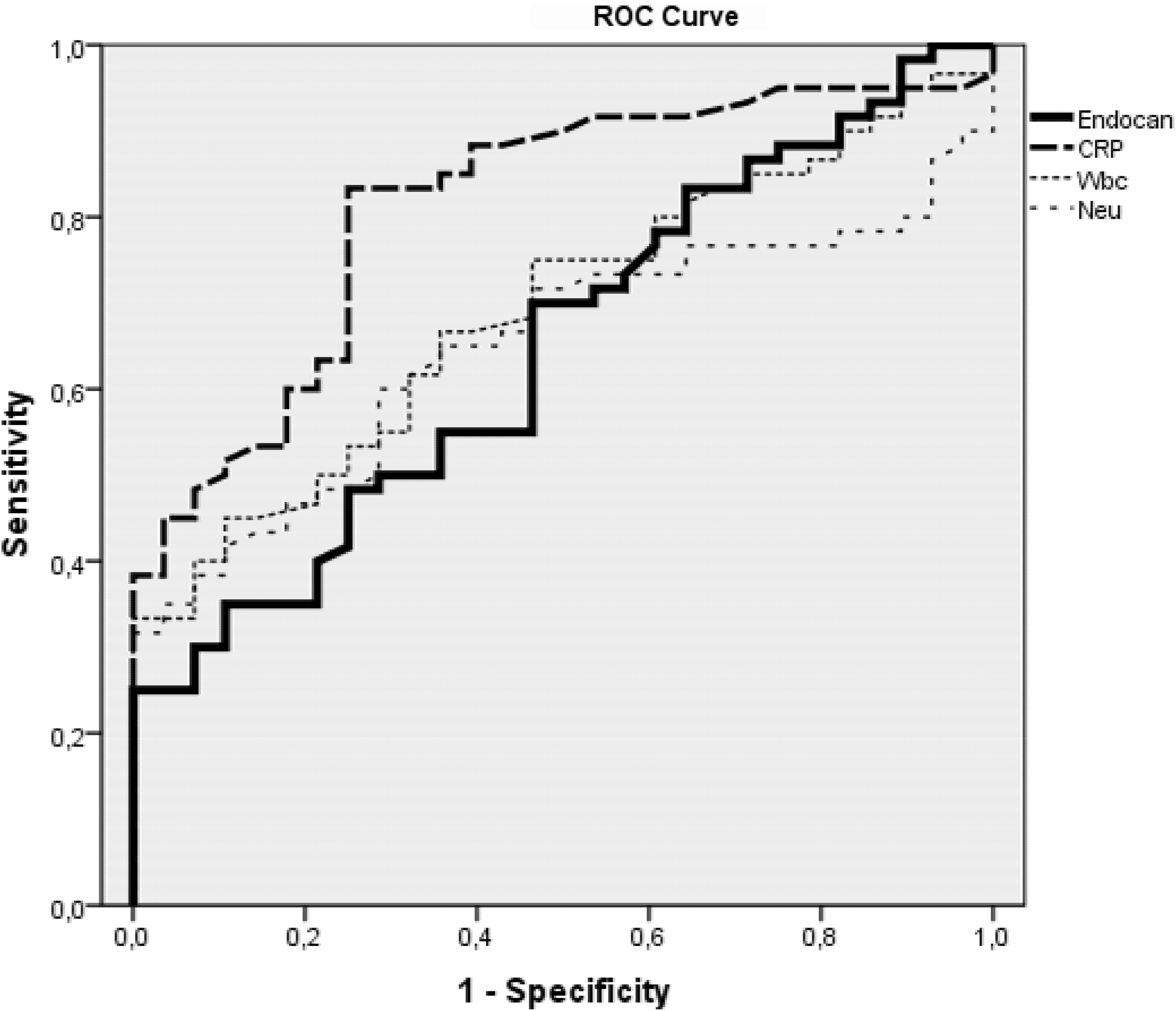
ROC analyses of biomarkers in patients with CAP. ROC, receiver operating characteristic.

ROC analyses of biomarkers in patients with severe CAP.
Discussion
In this study, serum endocan levels were significantly higher in children with CAP compared to the control group. To the best of our knowledge, there has been no study of serum endocan levels in pediatric patients with CAP. In a single study by Kao et al. conducted on adults with pneumonia, serum endocan levels were found to be higher compared to the control group. 11 That study result is consistent with the results of this study. Synthesis and secretion of endocan are performed by endothelial cells. The stimulation of endothelial cells by proinflammatory cytokines such as TNF-α and IL-1β increases the synthesis and secretion of endocan. The inflammatory response that occurs in patients with CAP is expected to increase the serum endocan levels. 12
Studies associated with serum endocan levels have also reported on diseases leading to inflammation of the lungs other than pneumonia. In a study of adult patients with a diagnosis of acute respiratory distress syndrome (ARDS) accompanied by pneumonia, serum endocan levels were found to be significantly higher. 9 Similarly, Scherpereel et al. determined higher endocan levels in patients with sepsis. 12 Saldir et al. showed that endocan can be useful in the early diagnosis of neonatal sepsis. 13 When these findings are taken together with the results of this study, endocan can really be considered a parameter for inflammatory diseases. Interestingly, Mikkelsen et al. found significantly lower levels of endocan in patients with acute lung injury (ALI) due to major trauma than in the control group. Endocan is known to have the effect of decreasing leukocyte recruitment. A reduction in the levels of endocan has been reported to cause dysregulation in leukocyte recruitment and therefore increase the risk of developing ALI. 14
The most important point in the guidelines for the treatment of CAP is to decide whether or not to hospitalize the patient. This decision is best informed by an accurate assessment of the severity of the disease at presentation. According to the disease severity, microbiological research, initial antimicrobial therapy, and treatment route and duration vary. 1 In this study, a positive correlation was found between serum endocan levels and disease severity. Similarly, in a study by Kao et al. of adults with pneumonia, serum endocan levels were reported to correlate with the severity of pneumonia according to the APACHE II, CURB-65, and PSI scoring systems. 11 Serum endocan levels have also been reported to be able to show the disease severity and mortality in patients with ARDS. 9 Scherpereel et al. showed that serum endocan levels are concordant with sepsis severity in adults. 12 In another study conducted on patients with sepsis, the serum endocan levels were reported to be more useful than the SOFA and APACHE II scoring systems to determine sepsis severity, organ failure, and mortality. 15 Similarly, in a recent study of adults with sepsis, serum endocan levels were reported to be a usable marker for diagnosis and to determine the severity of sepsis. 16 All these results indicate that endocan is a potentially important biomarker in the assessment of disease activity.
In this study, inflammation markers such as WBC and neutrophil count and CRP were investigated, as well as serum endocan levels, and all were statistically significantly higher in the patient group. In previous studies of adult patients with CAP, the CRP level and WBC and neutrophil count have been found to be higher in addition to serum endocan levels, although only serum endocan levels have shown a significant correlation with disease severity, and no significant correlation of CRP has been demonstrated. 11 Seo et al. did not detect a correlation between endocan and CRP levels in subjects with infection. 17 In contrast, besides the positive correlation between endocan levels and disease severity, we found endocan levels positively correlated with CRP levels in the CAP group. In studies of adults with ARDS, the level of CRP and WBC count have been shown to be higher, in the same way as the endocan levels, in the patient group, but CRP and WBC have been reported not to have sufficient power of differentiation of disease severity and organ failure unlike endocan. 9 While some studies have reported a correlation between traditional markers and disease severity in patients with CAP, 18 others have not.19,20 As endocan has a relationship with disease severity, it may be more useful than other traditional markers.
In this study, CRP and serum endocan levels were significantly higher in pediatric patients with severe pneumonia. The significance level of endocan was particularly noteworthy (P < 0.001). To the best of our knowledge, there has been no study in literature as yet that has examined the relationship between disease severity and endocan in patients with CAP. In studies of patients with sepsis, serum endocan levels were found to be higher in severe disease.12,15,16 Studies examining the relationship between disease severity and endocan levels are limited in literature. However, the evaluation of the findings of this study and the results of patients with sepsis suggest that endocan could be an important parameter with a positive correlation with disease activity.
In this study, the ROC analysis was evaluated to determine the diagnostic role of endocan in the diagnosis of patients with CAP; only CRP levels were found to be sufficient (AUC = 0.812). Endocan levels remained below acceptable limits (AUC = 0.649). However, when the role of these markers in distinguishing patients with severe pneumonia was examined, the only acceptable level was found to be for endocan (AUC = 0.769). Taking the level of 162.91 ng/mL as the cutoff value, sensitivity was 43.3% and specificity 96.4%. These results support that compared to the traditional markers, endocan can be a more valuable parameter in determining disease severity.
In a recent study, present scientific knowledge on endocan and some respiratory system disorders was reviewed. Together with the ones mentioned above, endocan was also found correlated with severity of obstructive sleep apnea and pulmonary thromboembolism.21,22
There were some limitations to this study. The number of patients was low and serum endocan levels were only measured once at the beginning of the study. Measurements of endocan during the different periods and treatments of the disease could better demonstrate the suitability of endocan as a biomarker in patients with CAP. There was no examination of the microbiological agents causing pneumonia in patients in this study, and although the routine investigation of the agents in pediatric patients with CAP is not recommended, it could be useful to investigate whether or not endocan has a role in the differentiation between bacterial or viral pneumonia.
In conclusion, serum endocan levels are seen to rise in patients with CAP. As the disease severity increases, endocan levels also continue to rise. Endocan can be used as a biomarker in diagnosis and especially in the determination of disease severity of CAP. Further studies are needed to assess the role of endocan in diagnosis and the monitoring of CAP therapy.
Authors' Contributions
Conception and study design: C.P., A.P., and S.G.; data collection: C.P., A.P., and M.D.; data analysis and interpretation: C.P., S.G., O.E., and M.D.; drafting of the article for intellectual content: C.P., A.P., O.E., M.D., and S.G. All authors approved the final version of the article before submission.
Footnotes
Author Disclosure Statement
No competing financial interests exist.