
Abstract
Fungi are considered one of the most common allergens responsible for type I allergies. This allergic response can be triggered by inhalation of mold spores, skin contact, or ingestion of mushrooms. There are some case reports in the literature advocating an association between sensitization to mold spores and systemic reactions caused by ingestion of mushrooms. However, this association is scarce and not completely explored. The authors report a case of a 12-year-old girl, with symptoms compatible with allergic rhinitis not previously studied, who developed an anaphylatic reaction after ingestion of mushrooms (Macrolepiota procera). The skin prick test revealed sensitivity to Cladosporium herbarum and the prick-to-prick test with the Parasol mushroom (M. procera) was positive, which highlighted the possibility of cross-reactivity between molds and mushrooms, hypothesis that was suggested by Western blot and inhibition test.
Introduction
F
Mushrooms may rarely be responsible for symptoms of food allergy in sensitized patients. Fungal allergens can cause allergic reactions by inhalation of mold spores, skin contact with saprophytic species, or ingestion of mushrooms. 3 Although respiratory allergy is induced mainly by mold spores, allergic symptoms after ingestion commonly can also occur through other structures of the mushroom. 4 There are 1.5 million species of fungi in the world, but the most allergenic species are molds belonging to the genera Alternaria, Aspergillus, and Cladosporium. 5 The overall extent of allergy of mushrooms is not known, varying from 1% in food allergy to 10% to 30% in pollen and mold allergy. 6
Previous reports suggest an association between sensitization to mold spores and systemic reactions, namely anaphylaxis, caused by ingestion of mushrooms, although this relationship is not well understood.4,7–9
The authors report a case of an adolescent with sensitivity to molds (Cladosporium herbarum) who developed an anaphylactic reaction after ingestion of Parasol mushroom (Macrolepiota procera).
Case Report
A 12-year-old girl was referred to the pediatric clinic because of anaphylaxis after ingestion of scrambled eggs with mushrooms. Almost 1 h after the meal, the adolescent suffered an episode of generalized urticaria, tachycardia, dyspnea, and tachypnea, symptoms that motivated admission in the emergency department, where ephinephrine and steroids were administrated with success.
When asked about personal medical background, symptoms compatible with rhinitis were identified, but she was not previously subjected to any allergy diagnostic tests or treatments. No other allergy diseases were identified, namely food allergy or atopic dermatitis. The adolescent denied any previous allergic reaction to the compounds of the meal responsible for the anaphylaxis. No family history of allergy was identified.
The laboratory tests realized in the pediatric clinic revealed an elevation of total immunoglubulin E (IgE) and a positive multiple aeroallergen screen and the specific IgE test was negative for the egg. The skin prick test (SPT) was positive for Lepidogliphus destructor (5 mm), C. herbarum (7 mm), Canis familiaris (7 mm), nuts (6 mm), and walnuts (5 mm). The prick-to-prick tests to Psalliota campestris and Tricholome equestre mushrooms were negative, but they were positive for different portions of Parasol mushroom (M. procera), confirming that the anaphylaxis was caused by this type of mushroom.
Because of the suspicion of a cross-reactive mechanism underlying the anaphylaxis, other investigation tests were undertaken to demonstrate a cross-reactivity between the aeroallergen C. herbarum and the food allergen M. procera. Mushroom extracts and sera from our patient were collected and analyzed by Western blot, which showed a protein with a molecular weight between 80 and 100 kDa in both allergens (Fig. 1). The inhibition assays confirmed that those proteins are related (Fig. 2). There were no similarities between the mushroom and the other allergens identified by the SPT. These results point to an existence of a cross-reactivity allergen between the aeroallergen C. herbarum and the food allergen M. procera.
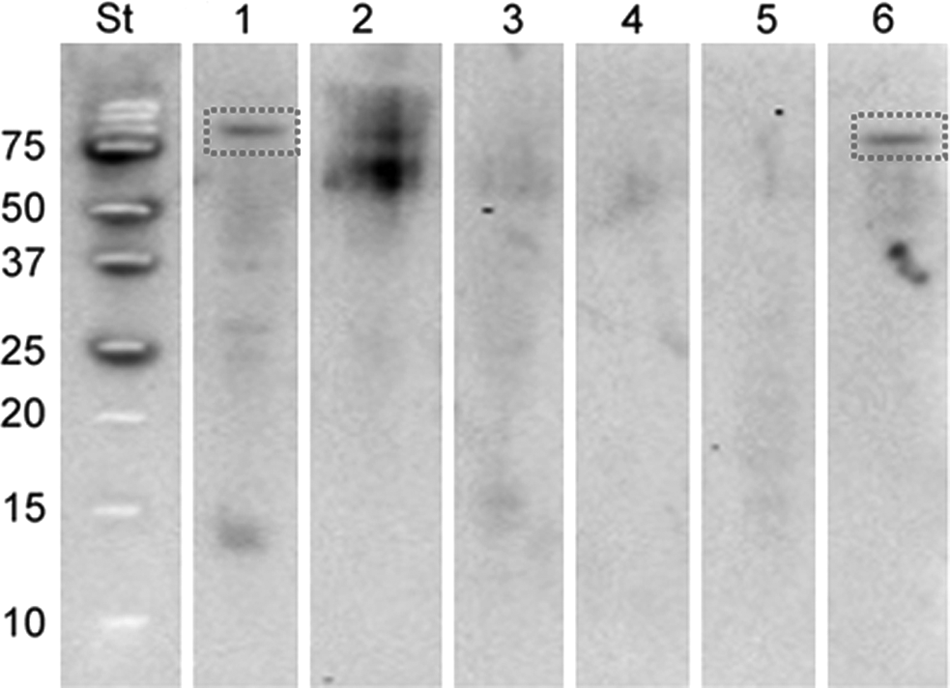
Western blot test with allergens identified in the skin prick test: 1, mushroom Macrolepiota procera; 2, Canis familiaris; 3, Lepidoglyphus destructor; 4, nuts; 5, walnuts; 6, Cladosporium herbarum.
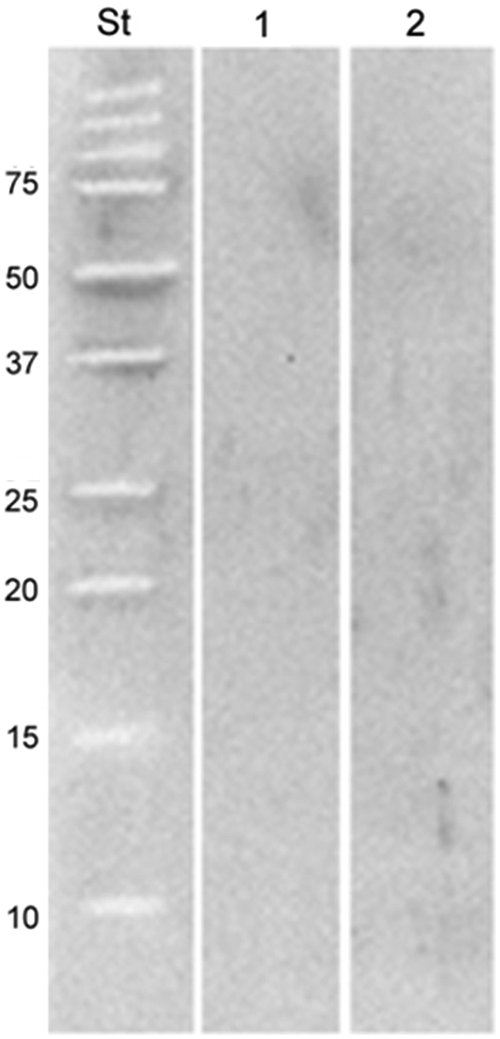
Inhibition test against C. herbarum. 1, mushroom M. procera; 2, C. herbarum.
The adolescent was encouraged to avoid any contact with the allergens identified, and since then, no other anaphylactic reactions happened.
Discussion
There are about 1.5 million species of fungi in the world, of which only 70,000 have been fully described. 10 Of the 1.5 million species of fungi, it was estimated that 140,000 species produce fruiting bodies of sufficient size and suitable structure to be considered macrofungi, also known as mushrooms. 11 The overall extent of mushroom allergy is unknown. Although mold allergy could be as prevalent as 10% to 30% of all allergic population, food allergy is very slight, being responsible for about 1% of all mushroom allergies. 6 Despite being rare, mushroom allergy is being recognized as a food allergen responsible for severe systemic allergic reactions.4,9,11,12 As demonstrated in the reported case, severe allergic reactions can occur even in people who have never had a previous allergic reaction. In fact, our patient had no previous symptoms of food allergy, even when mushrooms were eaten. One possible explanation for this late reaction is her sensitivity to mold spores, namely C. herbarum, which predisposed the adolescent to a cross-reaction with the mushroom M. procera. Actually, although there is increasing evidence of severe allergic reactions to mushrooms, clinical reports defending a cross-reactive mechanism underlying the association between aeroallergens and ingestion of mushroom symptoms are still scarce.4,7–9 In fact, knowledge of allergenic proteins that cause cross-reactions between molds and food is limited, which justifies the necessity of reporting this rare case to make possible a better understanding of the underlying immunological mechanisms.
The authors reported a case of an adolescent with respiratory symptoms compatible with allergic rhinitis caused by mold aeroallergens (C. herbarum), who suffered an anaphylactic reaction after ingestion of mushrooms (M. procera). Suspicion of cross-reaction between the mold aeroallergen and food allergen was confirmed by Western blot and inhibition test. The Western blot test identified a protein with similar weight in both C. herbarum and M. procera, and the inhibition test with antibodies against C. herbarum inhibited both allergens, which confirmed the cross-reactivity between them.
Our findings suggest a cross-reactivity between the aeroallergen C. herbarum and the mushroom M. procera, which can lead to severe food allergic reaction in mold-sensitized people. This highlights the importance of the recognition and knowledge of this possible relationship between aeroallergens and food allergens, looking for an effective avoidance and prevention of severe systemic reactions.
Consent
The authors state that they have obtained parental permission to publish this case report.
Footnotes
Author Disclosure Statement
No competing financial interests exist.