
Abstract
The respiratory impedance reference values for the forced oscillation technique (FOT) pseudorandom signal in Thai and Asian preschool population have not yet been established. The aim of this study was to determine the reference values for respiratory impedance as predicted by height and arm span using FOT and assess the feasibility and variability associated with the use of this technique in Thai preschool children. FOT pseudorandom signal was used to measure respiratory impedance (Zrs), which is composed of respiratory resistance (Rrs) and respiratory reactance (Xrs), in Thai healthy children aged 3–7 years. Feasibility, within-test variability, between-test repeatability, and association between Zrs values at 6, 8, and 10 Hz and independent variables, including age, weight, height, arm span, and gender, were assessed. Regression equations of Rrs and Xrs values were also determined. Of 291 children, FOT was successfully performed in 233 children (80.1%). Within-test variability was 2%–3% for Rrs and 9%–15% for Xrs. Between-test repeatability showed mean difference between the 2 sets of all Rrs and Xrs values to be nearly zero. Height was found to be the best predicting factor for 5 of 6 Rrs and Xrs values (excluding Xrs10) and arm span also has strong predictability and correlation with Rrs and Xrs values. Arm span can, therefore, be used in place of height in patients whose height cannot be measured, such as patients with kyphoscoliosis or neuromuscular diseases. FOT is a feasible and repeatable method for evaluating lung function in preschool-aged Thai children. The reference values for respiratory impedance as predicted by height and arm span using FOT were determined in this study. The results of this study may be useful in the determination of respiratory impedance reference values in preschool children from other Asian populations in the future.
Introduction
S
Ethnic differences in pulmonary function are evident.6–9 To achieve effective patient management and avoid misdiagnosis of pulmonary diseases, interpretation of PFT should be based on ethnicity-specific data.10,11 Previously reported reference values using commercially available FOT pseudorandom noise signal in preschool children have been established from Australian, 4 Italian, 2 and Mexican 12 children, all of whom are from the Caucasian race. To our knowledge, no study of this technique in Thai or Asian preschool-aged children has been published.
Generally, height, gender, and age are used to predict pulmonary function. However, in patients with neuromuscular diseases, spinal deformities, or chest wall deformities, height cannot be measured accurately. In these patients, arm span is recommended as a surrogate for height in predicting reference values.10,13,14 Based on our review of the literature, no report that describes the respiratory impedance reference values for FOT as determined by arm span has been published.
The aims of this study were to determine the reference values for respiratory impedance as predicted by height and arm span using FOT and assess the feasibility and variability associated with the use of this technique in Thai preschool children.
Materials and Methods
Study population
This cross-sectional study recruited healthy children aged 3–7 years from kindergartens and primary schools in Bangkok, Thailand, during the January 2012 to March 2014 study period. Evaluations of study children were conducted at Siriraj Hospital, Thailand's largest national tertiary referral center. The exclusion criteria were children with heart diseases, neuromuscular diseases, and chronic lung diseases, such as bronchopulmonary dysplasia and asthma. Children with history of wheezing, pneumonia, preterm birth, birth weight <2,500 g, respiratory tract infection within 2 weeks before the study, and environmental tobacco smoke were also excluded. Baseline data, including age, weight, height, arm span, and gender, were recorded. Written informed consent was obtained from the legal guardians of all children before inclusion. The protocol for this study was approved by the Siriraj Institutional Review Board (SIRB), Faculty of Medicine Siriraj Hospital, Mahidol University.
FOT measurement
The Quark i2 m forced oscillation system (Cosmed, Rome, Italy) was used to obtain respiratory impedance (Zrs), consisting of respiratory resistance (Rrs) and reactance (Xrs). This testing method generates a pseudorandom noise with multiple frequencies that range from 4 to 48 Hz, with a measurement period of 8 s in duration. Pseudorandom noise is an optimized form of composite signals applied to spontaneous breathing without any related discomfort to the patient.1,15 Coherence function, which is a measure of the linear relationship between input and output signals and reflects the validity of the measurements at individual frequencies, was automatically assessed at each frequency.
Respiratory impedance was measured according to American Thoracic Society/European Respiratory Society (ATS/ERS) guidelines. 16 Measurements were performed with children in a sitting position, with their head in a neutral position, and with a noseclip in place. Cheeks and lower jaw were supported by a technician's hands. Each child was instructed to breathe normally through a mouth piece fitted with an antibacterial filter (part no. A182 300 004) (Cosmed, Rome, Italy), which was connected to the previously described forced oscillation system. Before data collection, children were given time to familiarize themselves with the environment, equipment, and technicians, and training was provided to each child to ensure consistent tidal breathing on measurements.1,16
Three to five technically acceptable measurements were obtained in 1 testing session. Two sets of measurements were obtained 15–20 min apart to determine the between-test repeatability of FOT (short-term repeatability) in 108 children. Measurements were considered to be acceptable if coherence at an individual frequency was ≥0.95, and excluded if ≥3 individual frequencies had a coherence of <0.95. Measurements with swallowing, mouth leak, mouth movement, glottic closure, or audible noise were excluded. Respiratory resistance and reactance at 6, 8, and 10 Hz were reported and analyzed. These parameters were described as Rrs6, Rrs8, and Rrs10 for respiratory resistance and Xrs6, Xrs8, and Xrs10 for respiratory reactance at 6, 8, and 10 Hz, respectively.
Statistical analysis
Data analysis was performed using SPSS for Windows version 18 (SPSS, Inc., Chicago, IL). Data are expressed as mean ± standard deviation (SD). Within-test variability of all Rrs and Xrs values was assessed from SD and average mean in the first set of measurements, and determined by coefficient of variability (CV) (CV = SD × 100/mean). Between-test repeatability was analyzed by paired t-test, intraclass correlation coefficient, and Bland-Altman analysis. Correlation between Rrs and Xrs and independent variables, including age, weight, height, and arm span, were assessed using Pearson's correlation coefficient. Unpaired t-test was used to assess association between gender and Rrs and Xrs variables. Finally, multiple linear regression was used to analyze association between significant independent variables and Rrs and Xrs values. A P-value <0.05 was considered to be statistically significant.
Results
Basic characteristics and feasibility of FOT at different ages
Of the 291 preschool-aged children (range: 3–7 years) enrolled in this study, FOT pulmonary function testing was successfully performed in 233 (80.1%) children. Regarding gender distribution, 101 (43.3%) children were boys and 132 (56.7%) were girls. Mean ± SD age, weight, height, and arm span were 5.3 ± 1.02 years, 19.1 ± 3.8 kg, 110.3 ± 7.6 cm, and 109.1 ± 8.3 cm, respectively. The success rate increased with age by 64.6%, 72.4%, 82.5%, and 95.7% in children aged 3–4, 4–5, 5–6, and 6–7 years, respectively.
Within-test and between-test variability
Respiratory resistance (Rrs) demonstrated lower within-test variability than respiratory reactance, as observed from lower CV values for all Rrs values relative to the CV values for all Xrs values (Rrs6 of 2.64 versus Xrs6 of 9.47; Rrs8 of 2.19 versus Xrs8 of 14.94; and Rrs10 of 2.27 versus Xrs10 of 11.57) (Table 1). The mean difference between the first and second set of all Rrs and Xrs values was nearly zero and not significantly different (P > 0.5) (Table 2). Bland–Altman analysis also demonstrated agreement between the first and second sets for all Rrs and Xrs values, and the example of Bland–Altman plot of agreement for Rrs6 is given in Figure 1.
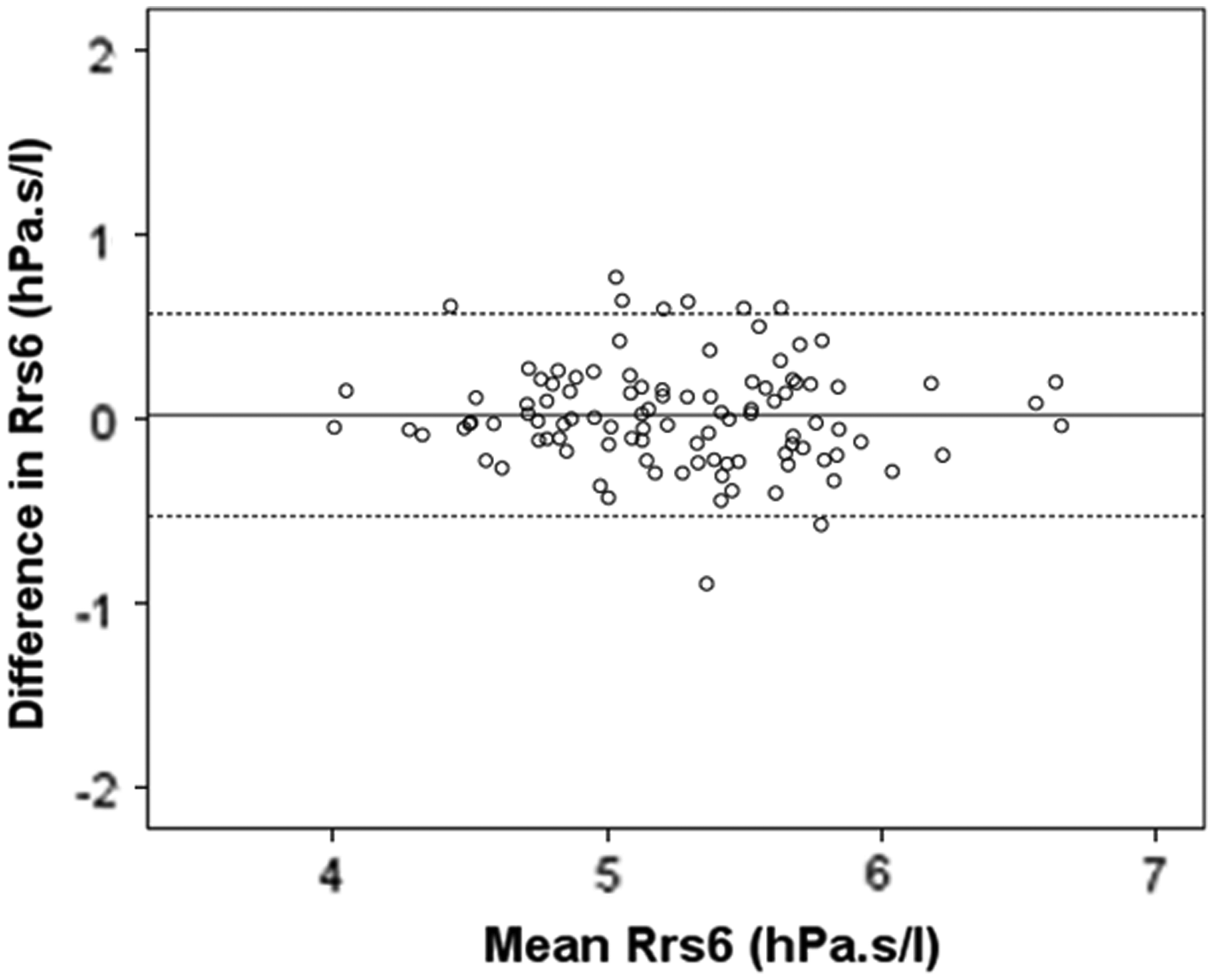
Bland–Altman plot showing agreement between the first and second sets for Rrs6. Solid line represents the mean of difference and dashed lines represent the upper and lower limits of agreement.
SD, standard deviation; CV, coefficient of variation; Rrs, respiratory resistance; Xrs, respiratory reactance; NS, no significance.
ICC, intraclass correlation coefficient; Rrs, respiratory resistance; Xrs, respiratory reactance; NS, no significance; SD, standard deviation.
Correlation, multiple regression analysis, and regression equation
Gender was found not to be related with any FOT outcome variable (Table 1). With the exception of Xrs10, all 5 other Rrs and Xrs value measurements were found to be correlated with age, weight, height, and arm span (Table 3). When analyzed by stepwise multiple regression analysis that included gender, age, and height as independent variables, height was the only predicting factor for all Rrs values (Rrs6, Rrs8, and Rrs10) and for Xrs6 and Xrs8. When substituted for height, arm span was also found to be a significant predictor for all Rrs values and for Xrs6 and Xrs8. Weight was not included in the analysis because it was highly correlated with height. The regression equations are shown in Table 4. R2 value in regression equations was higher for height than for arm span. The reference ranges of respiratory impedance as a function of height and arm span are shown in Figures 2 and 3.
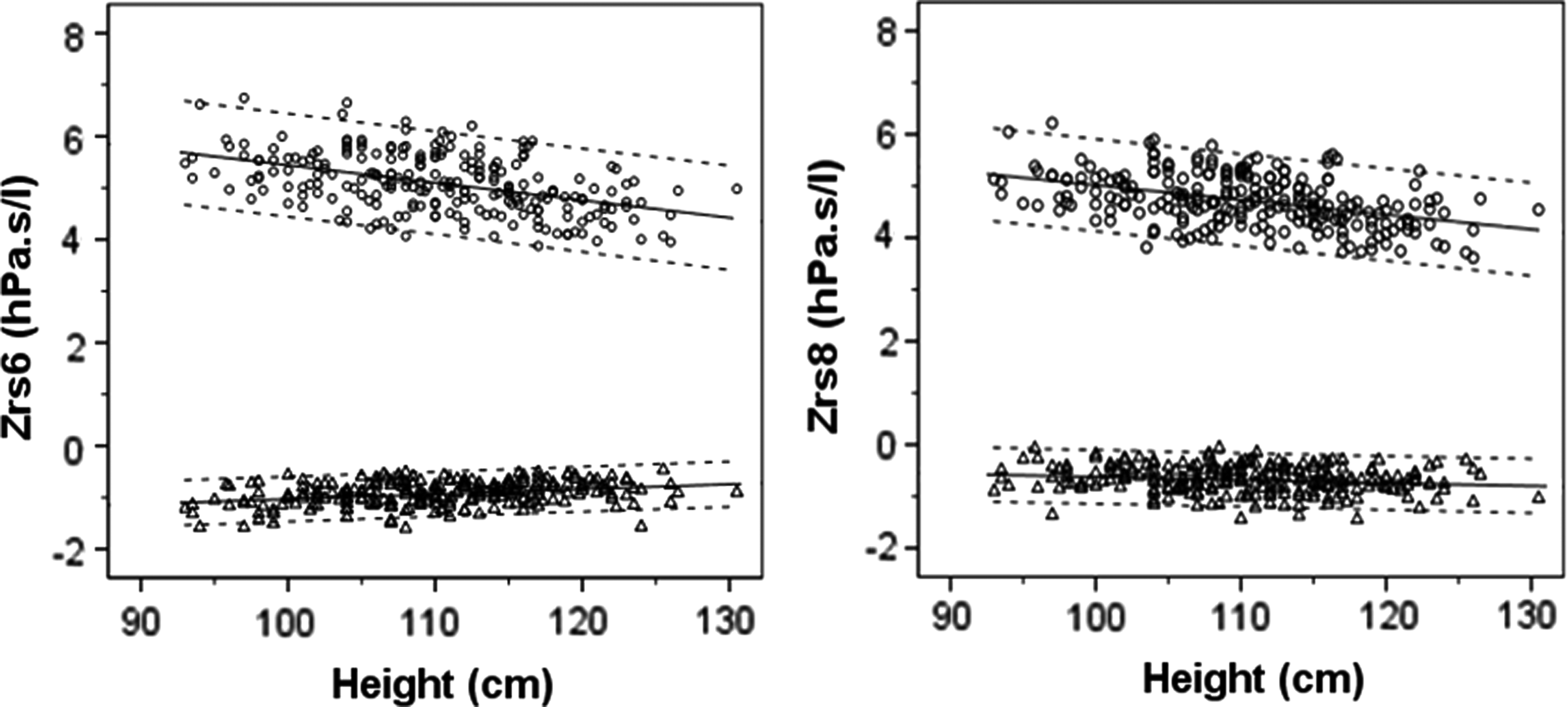
Correlation between height and respiratory impedance (Zrs) at 6 and 8 Hz. Respiratory resistance (Rrs) values and reactance (Xrs) values are plotted as circle and triangle, respectively. Regression lines and 95% confidence interval are shown as solid lines.

Correlation between arm span and respiratory impedance (Zrs) at 6 and 8 Hz. Respiratory resistance (Rrs) values and reactance (Xrs) values are plotted as circle and triangle, respectively. Regression lines and 95% confidence interval are shown as solid lines.
A P-value <0.05 indicates statistical significance.
Rrs, respiratory resistance; Xrs, respiratory reactance; r, correlation of coefficient.
A P-value <0.05 indicates statistical significance.
R2, coefficient of determination; Rrs, respiratory resistance; Xrs, respiratory reactance.
Discussion
This study found the FOT to be both feasible and repeatable for measuring lung function in Thai preschool children with a success rate of 80%. Moreover, we found that the success rate increased with age, which is comparable to previous reports.5,12,17 Also, consistent with previous reports, our study demonstrated low within-test variation, as determined by the coefficient of variation (CV), of respiratory resistance (Rrs) and the good short-term repeatability of FOT.2,4,5 This result emphasizes that FOT pseudorandom signals can be used as a PFT in preschool children. However, the within-test variation of Rrs and Xrs was slightly lower than previously published data. The CV of Rrs6, Rrs8, and Rrs10 in our study was 2.64%, 2.19%, and 2.27%, respectively, compared with other studies that used the same technique that reported 6%–9%.2,4,5 For within-test variation of Xrs, previous studies by Hall et al. 4 and Calogero et al. 2 reported CV of Xrs of 16%–20% and 17–19%, respectively. Our study found a CV of Xrs of 9%–15%. This difference in findings may be due to the fact that we provided a significant amount of time for children to familiarize themselves with the technicians and the FOT machine, and to train them in the process before lung function testing.1,16 Hall et al. 4 found that children performing the FOT test in a laboratory setting had lower test variability when compared with time-limited field study. They further concluded that training children in the test-taking process before lung function measurement affected within-test variability. Another possible explanation for the difference in CV of Rrs and Xrs between studies may be differences in the type of testing equipment used.
When we analyzed the effect of gender, age, and height as independent variables, height was found to be the best determinant of respiratory resistance. This finding is consistent with that of several previous studies.2,4,12,18–22 Our reference equations for respiratory impedance were different than those reported from other studies that used the FOT pseudorandom signal technique (Fig. 4).2,4,12,23,24 This discrepancy is likely due to ethnic differences and differences in equipment specifications. We do not think the difference can be attributed to our technique, since we carefully followed standardized measurement protocol according to ATS/ERS recommendations. 16 Regarding ethnicity, Shackleton et al. 12 reported that reference values of respiratory impedance established from Caucasian preschool children overestimated the lung function of Mexican preschool children. However, no reference value using FOT pseudorandom signals established from Asian preschool children has been published for comparison. The findings of Shackleton et al. 12 and those from this study support the hypothesis that FOT reference values should be race specific, and perhaps even ethnicity specific. Further studies are needed to elucidate the reasons why different studies have found and reported different results.
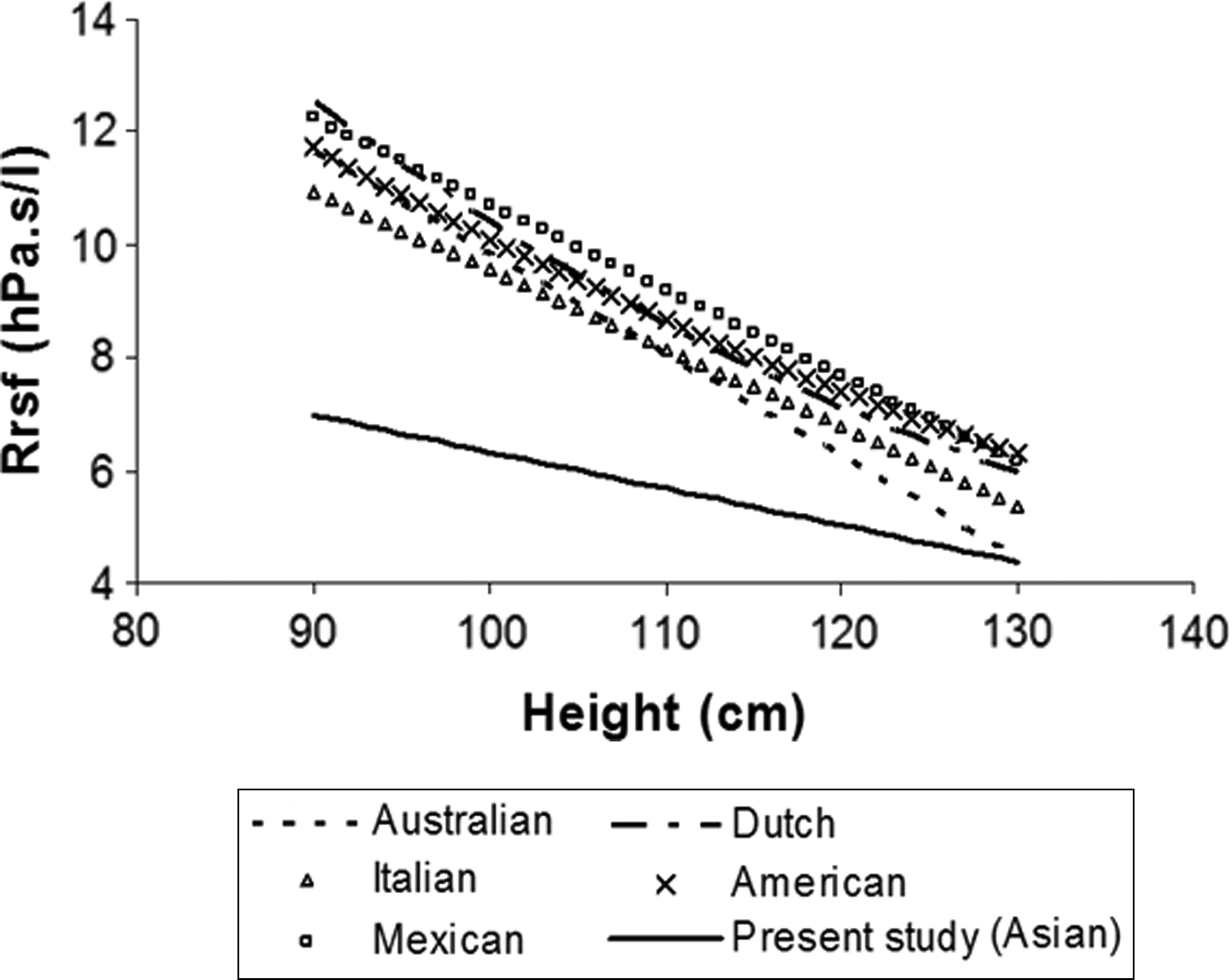
Reference equation of respiratory resistance compared with previous studies.
Our study determined reference equations for respiratory resistance and reactance predicted by arm span. ATS/ERS recommends using arm span when height cannot be measured. 10 Prediction equations for spirometry based on arm span have been reported. 25 However, and to our knowledge, reference values for preschool lung function using FOT predicted by arm span have not been reported. Arm span is suitable for predicting lung function in patients whose height cannot be measured or whose height measurement is likely to be inaccurate, such as in patients with neuromuscular disease or kyphoscoliosis. Height should be used in cases where patient height can be accurately obtained because the reference equations for respiratory resistance by height have a higher coefficient of determination, as demonstrated by R2.
This study has some mentionable limitations. While we intend that our findings will have benefit for pulmonary clinicians in other Asian countries, we cannot be certain that these findings can be extrapolated to preschool children from other countries in Asia.
The strengths of this study include low variability, high repeatability, and that children living in Bangkok are often from families that originate from all regions of Thailand. We propose that these findings will have immediate value for pulmonologists who treat young children in Thailand and will provide baseline data for future larger studies, both within Thailand and in other countries in Asia.
Conclusions
FOT is a feasible and repeatable method for evaluating lung function in children who have limited attention span and could follow only a simple and easy procedure, such as preschool age between 3 and 7 years. The reference values for respiratory impedance as predicted by height and arm span using FOT were determined in this study. The results of this study may be useful in the determination of respiratory impedance reference values in preschool children from other Asian populations in the future.
Footnotes
Acknowledgment
The authors gratefully acknowledge the children and parents who agreed to participate in this study. The authors would also like to thank Assoc. Prof. Vip Viprakasit and Mr. Kevin P. Jones for editing the article. This research project is supported by the Siriraj Routine to Research Management Fund, Faculty of Medicine, Siriraj Hospital, Mahidol University.
Author Disclosure Statement
No competing financial interests exist.