
Abstract
We describe a 7-year-old girl with recurrent prolonged periods of coughing since 2 weeks of age. First seen at the University of Iowa Pediatric Pulmonary Clinic at 5 months of age, a flexible bronchoscopy and bronchoalveolar lavage found tracheomalacia (TM) and protracted bacterial bronchitis (PBB). A repeat bronchoscopy at 4 years of age performed because of continued recurrences of chronic cough showed TM essentially the same as seen at 5 months with the neutrophilia and bacteriology typical for PBB. Computerized tomography (CT) at age 7 performed because of continued recurrences of prolonged coughing responsive to amoxicillin–clavulanate demonstrated a narrowed anterior mediastinum causing vascular compression of the trachea by the great vessels. The decrease in the anterior mediastinal space was caused by the absence of the normal dorsal curvature of the upper spine. This abnormality is known as the straight back syndrome (SBS). While previous reports of the SBS focused on the potential for cardiac anomalies, this patient manifested recurrent PBB as a result of this anomaly. The observations in this patient are consistent with other data that support intrathoracic airway malacia as being an important contributing factor for PBB.
Introduction
P
Straight back syndrome (SBS) is a congenital disorder resulting in an absence of the normal dorsal curvature of the upper thoracic spine. This results in a decrease in the anterior/posterior (AP) diameter of the upper chest, which can cause compression of the heart and great vessels. In an early report, SBS was noted to be a cause of “pseudo” heart disease. 7 While often asymptomatic, chest pain or palpitations from compression and lateral displacement of the heart were described. 8 While respiratory symptoms have generally not been prominent with this disorder, dyspnea and restrictive lung disease were described from tracheal compression in four adults requiring surgical correction. 9
We identified recurrent episodes of PBB in a girl with SBS that, atypically, persisted to school age. The anatomic abnormality of the SBS in this child was associated with compression of structures in the anterior mediastinum. The purpose of this presentation is to demonstrate respiratory consequences of SBS causing intrathoracic airway malacia resulting in recurrent PBB persisting from infancy to school age. The parents and patient were agreeable to reporting this case without personal identification for educational purposes.
Case
Our patient was first seen at the University of Iowa Children's Hospital Pediatric Pulmonary Clinic at age 5 months for persistent coughing and noisy breathing present since 2 weeks of age. Chest radiograph at that time was unremarkable. Flexible bronchoscopy demonstrated tracheomalacia (TM) with ∼80% loss of cross-sectional area observed during exhalation (estimated by clinical observation). BAL showed minimal neutrophilia (5%), but high colony counts of H. influenzae, 4 × 105 colony forming units per milliliter (cfu/mL), and M. catarrhalis, 5 × 105 cfu/mL. She was treated for PBB with 14 days of amoxicillin–clavulanate and had complete resolution of cough and noisy breathing.
However, she continued to have recurrent exacerbations of symptoms consistent with PBB, which were successfully treated in each instance with 14 days of amoxicillin–clavulanate. 10 Since this child did not follow the pattern we usually saw with PBB where the frequency decreases with age, 5 repeat flexible bronchoscopy was performed after 4 years of recurrent noisy breathing and prolonged coughing. Severe TM was again seen. Similar to the description seen during the first year of life, there was an estimated 80% loss of cross-sectional area during exhalation (Fig. 1). BAL findings showed very high neutrophilia (61% of nucleated cells). Culture grew 2 × 105 cfu/mL of S. pneumoniae.

Bronchoscopy at age 4 years showing the trachea during inspiration (upper panel) and ∼80% loss of cross-sectional area of the same patient during exhalation (lower panel).
Cough cleared again with amoxicillin–clavulanate, but prolonged coughing episodes continued to recur several times per year requiring repeat treatment with amoxicillin–clavulanate. To further characterize her TM, computerized axial tomography (CT) of the chest was performed at age 7. That study showed narrowing of the trachea of at least 50% at the crossing of the innominate artery (Fig. 2). Also noted was decreased AP diameter of the upper chest (Fig. 3). A lateral chest view of the CT (Fig. 4) showed that the normal gentle kyphotic curve of the upper dorsal spine was absent. She was otherwise a normal appearing 7-year-old girl with no apparent pectus abnormality. Although a heart murmur was present, an echocardiogram was normal, and the murmur was judged to be functional. Spirometry, performed on four occasions at ages 5–7, was consistently within the normal range.

CT at age 7 years with 3D reconstruction showing tracheal compression by the innominate artery. CT, computed tomography.
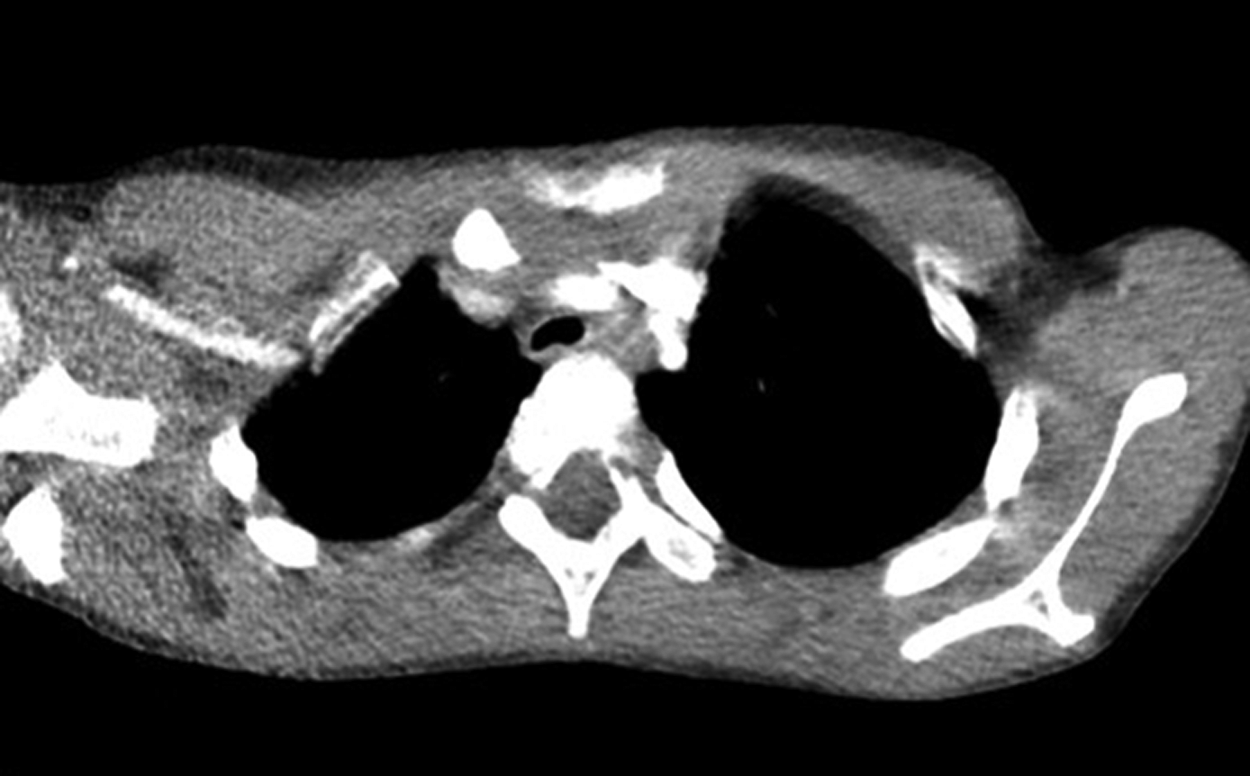
CT of the chest at 7 years showing tracheal compression by the innominate artery and the narrowed anterior mediastinum.

Lateral view of the thorax at age 7 years showing the absence of the normal kyphotic curve of the upper thorax.
Consultation was requested from pediatric surgery for the parents to consider surgical options. Surgical correction of TM with aortopexy is usually satisfactory at decreasing vascular compression of the trachea. 11 The procedure involves attaching the aortic arch to the sternum, thereby putting tension on the connective tissue between the great vessels and the anterior wall of the trachea. The tracheal lumen is then stented open. However, the space between the sternum and the aorta in our patient was insufficient for the procedure to offer a therapeutic option. Surgery, if needed for this girl, would require a more complex procedure. 12
Parents elected to defer surgical correction for now so long as the child functioned without chronic respiratory distress and the recurring coughing from PBB was becoming less frequent with age and continued to respond to 2-week courses of amoxicillin–clavulanate.
Discussion
Our case shows an SBS as a cause of tracheal compression by the great vessels. PBB, presenting as chronic wet cough beginning in infancy, continued to recur beyond the age where symptoms of PBB are usually associated with clinical remission. 5 In a review of the literature, Soleti et al. stated that most patients with SBS are asymptomatic, and those who were symptomatic frequently had mitral valve prolapse and bicuspid aortic valve. 13 An echocardiogram of our patient identified no cardiac abnormalities. One of the cases described by Grillo et al. had a long history of symptoms thought to be asthma and progressed with development of prominent inspiratory and expiratory stridor. 9
We previously reported seventy patients (20 female and 50 male) with PBB. Similar to this patient with SBS, all but five children had onset of symptoms before the age of 1 year (median 3 months of age). Neither this patient with SBS nor the patients from our previous report had fever or toxic appearance associated with their respiratory symptoms. Airway malacia, tracheal and/or bronchial, was observed in 74%, 52 of the 70 patients. Bronchomalacia alone was most common (43%), TM was present in 20%, and 11% of the 70 had both bronchomalacia and TM. Quantitative culture from BAL showed levels of bacteria ≥104 cfu/mL (most ≥105 cfu/mL) of S. pneumoniae, H. influenzae, and M. catarrhalis. Two or three organisms were seen in nearly half of cases, 4 with S. pneumoniae and H. influenzae, 7 with S. pneumoniae and M. catarrhalis, 13 with H. influenzae and M. catarrhalis, and 9 showing high colony counts for all three organisms. Penicillinase production was common in both H. influenzae and M. catarrhalis. Resistance to penicillin was not seen for S. pneumoniae. Substantial neutrophilia was present in most (median 44%).
The persistence of TM and recurrent PBB in this patient with SBS, beyond the usual age when remission of symptoms from PBB usually occurs, is consistent with other data supporting intrathoracic airway malacia as an etiologic factor for PBB. Donnelly postulated that intrathoracic airway malacia was a cause of PBB. 14 Masters et al. observed that children with airway malacia have increased frequency of respiratory illness, severity of illness, and tendency for delayed recovery. 15 Boogaard et al. also reported chronic bacterial bronchitis in children with TM and bronchomalacia who presented with cough, noisy breathing, and recurrent wheeze. 16 While bacterial infection might in some cases be a primary event that causes tracheal or bronchial damage resulting in malacia, 17 the current patient with SBS supports malacia as the primary factor that results in PBB.
The natural history of untreated PBB is not known. However, in a study of 161 children with PBB (66% boys), 13 were diagnosed with early signs of bronchiectasis over the study period (8.1%). 18 Episodes recurred in 43.5% of the children, a frequency somewhat lower than the 61% seen in our study of 70 children. 5 Major risk factors for bronchiectasis included lower airway infection with H. influenzae recovered in BAL fluid (P < 0.013) and recurrent episodes of PBB (P < 0.003). 18 H. influenzae infection conferred a more than seven times higher risk of bronchiectasis (P < 0.009) compared with no H. influenzae infection. The majority of H. influenzae isolates were nontypeable (82%). No risk factors predicted recurrences of PBB. Despite multiple episodes over the prior 7 years of her life, the chest CT of our patient with SBS showed no evidence of bronchiectasis. Perhaps that related to the vigorous prompt treatment with antibiotics that had been given in each instance when cough returned.
The relationship between intrathoracic airway malacia was suggested by the presence of bronchomalacia and/or TM in 74% of the 70 patients in our previous report. 5 Support for intrathoracic airway malacia as a potential etiologic factor for PBB is also suggested by the observation that TM is associated with an increased risk of Pseudomonas infection in children with cystic fibrosis (CF). 19 Whereas TM has been estimated to occur in about 1 in 2,100 of all infants and toddlers, 16 TM was documented in 15 of the 97 patients (15%) with CF who had been bronchoscoped in the course of their treatment. Chest CT was performed in 11 of the 15 patients with TM. Tracheal abnormalities were visible on CT for six of them. Pulmonary function testing was completed for 11 of the 15 patients with TM. Large airway obstruction was apparent on spirometry (reduction in peak expiratory flow rate or oscillations on peak flow) for five of those patients. Patients with CF with a diagnosis of TM acquired their first Pseudomonas aeruginosa infection earlier than those without TM, median of 1.3 and 2.6 years, respectively (P < 0.01). Mucoid P. aeruginosa, a surrogate for chronic Pseudomonas infection, also was present significantly earlier in CF patients with TM (P < 0.04).
This case provides further evidence that intrathoracic airway malacia is a major contributing factor for PBB, presumably by interfering with normal airway clearance. There are continuing unknown aspects of both this case and other children with PBB. Will the girl in this report with SBS eventually have greater compression of her trachea from the innominate artery resulting in a greater obstruction than is currently present or will fewer acute symptomatic periods occur with age and growth? And there continues to be concern for the long-term outcome of all children with PBB. Only a minority (13 of 161) had evidence of bronchiectasis during a 2-year follow-up in the one report that examined for this potentially serious consequence. 18 However, will longer follow-up increase the prevalence of irreversible damage to the infected and inflamed peripheral airways of PBB, particularly if not adequately treated?
Footnotes
Acknowledgments
Michelle Kompare, pediatric neonatology fellow, assisted with the original case report, Simon Kao, pediatric radiologist, assisted with the radiology, and Dean Potter, pediatric surgeon, provided surgical consultation.
Author Disclosure Statement
No competing financial interests exist.