
Abstract
Background:
Patients with status asthmaticus admitted to the hospital contribute tremendous costs to the healthcare system. Treatment protocols directed at improving care to pediatric inpatients have improved both clinical and financial outcomes; however, there are limited data demonstrating the impact of goal-driven therapy for patients with status asthmaticus in the pediatric intensive care unit (PICU). The purpose of this initiative was to standardize care of children with status asthmaticus in the PICU to improve clinical outcomes.
Materials and Methods:
A goal-directed clinical pathway using a validated pediatric asthma severity score was developed. A pre–post intervention assessed patients 2–17 years of age admitted to the PICU with status asthmaticus. The effect of the protocol was measured from October 2015 to October 2016. The primary outcome was the transition time interval from continuous nebulized bronchodilator therapy to every 2 hourly intermittent treatments. Secondary outcomes related to treatment options and clinical complications were also assessed.
Results:
Postintervention patient (n = 124) demographics were similar to those in the preintervention group (n = 130). Compared with baseline, there was a 4.9-h decrease in the mean transition time from continuous to intermittent bronchodilator use (31.9 versus 27.0, P = 0.033) following the intervention. The mean and median hospital length of stay (LOS) was significantly decreased in the postintervention group by 14.76 h (P = 0.011) and 16.68 h (P = 0.003). There were no readmissions to the PICU in the postintervention group. The use of rescue BiPAP (Bi-level positive airway pressure ventilation) was significantly higher in the preintervention group compared with the postintervention group (42% versus 28%, P = 0.036).
Conclusions:
A severity-tiered, goal-driven treatment pathway for pediatric patients admitted to the PICU with status asthmaticus reduced the time required to transition from continuous to intermittent inhaled bronchodilator use. As a result, overall hospital LOS was significantly decreased with no increase in clinical complications.
Introduction
A
In 2005, over 13% of hospital costs in the United States were attributed to critical care medicine. 10 In one study of costs of care between medical and surgical patients in an academic PICU, the mean daily costs for patient care during the pediatric intensive care hospitalization ranged from $5,138 to $5,903. 11 Additionally, these data revealed that cost of PICU care was independent of illness severity and dependent on intensive care unit (ICU) LOS. Thus, reducing pediatric intensive care LOS may be an effective cost control measure within the PICU setting.
National evidence-based guidelines outline best practices for the diagnosis and management of asthma; however, adherence to guidelines, particularly in urban settings, is poor due to fast-paced clinical environments, limited resources for testing and patient education, and lack of provider familiarity with specific guideline components.12–15 Furthermore, studies have shown poor adherence to evidence-based guidelines and large regional variability in practice among PICUs for acute asthma management.16,17 Stepwise escalation of therapy for severe acute asthma exacerbations has been proposed for patients in the PICU with status asthmaticus, but not studied for clinical outcomes. 18
The purpose of this quality improvement initiative was to implement an evidence-based, stepwise approach directing escalation and de-escalation of therapy to pediatric patients presenting to the PICU with status asthmaticus to improve clinical outcomes and reduce cost of care.
Materials and Methods
Setting
The University of Chicago Medicine Comer Children's Hospital is a 172-bed acute care hospital, which contains a 30-bed PICU. The PICU is a multidisciplinary medical and surgical unit with a closed ICU model wherein all patients are primarily managed by a pediatric critical care physician. The usual care team participating in the daily rounding process and clinical management decisions includes one attending physician, one critical care fellow, two to three pediatric residents, and a PICU-based pharmacist and dietician. There are two care teams in the PICU daily, and 16 board-certified pediatric intensivists make up the core of the Attending Physician group.
Planning the intervention
Data consistently show wide variation in practice style in pediatric inpatient asthma care. 19 It was observed that patients admitted to the PICU at Comer Children's Hospital underwent differential management depending on the Attending Physician's preference of medication as well as respiratory support modalities. To standardize practice, a new evidence-based stepwise escalation of asthma management was developed as part of a quality improvement initiative. Applying implementation science theory, multidisciplinary stakeholders were engaged to develop and implement a clinical pathway for the management of status asthmaticus in the PICU. 20 Interdisciplinary focus groups with clinical content experts, including pediatric intensivists and pulmonologists, were convened. A goal-oriented pathway driven by a previously validated pediatric asthma severity score (PAS) was developed to guide escalation and de-escalation of therapy. 21 The asthma severity score was modified with respect to oxygenation as to not risk clinical deterioration while testing oxygen saturations in room air for critically ill patients requiring supplemental respiratory support (Table 1).
Range of available score from 5 to 15.
BiPAP, Bi-level positive airway pressure ventilation; HFNC, high-flow nasal cannula.
The status asthmaticus pathway was developed using targets from the asthma severity score. Evidence-based severity-tiered medication options were driven by the calculation of asthma severity score (Table 2).17,18,22 Nurses (RN) and respiratory therapists (RT) assigned the PAS severity score and documented in the electronic medical record (EMR) at least hourly during clinical assessments or respiratory interventions, with each individual clinician scoring on alternate hours. The RN/RT communicated to the physician if a change in score would allow for escalation or de-escalation as per the pathway. Physicians were free to choose any management option within each category without restriction and all management changes were ultimately made at the discretion of the treating physician.
MDI, metered dose inhaler; PAS, pediatric asthma severity score; PO, by mouth.
Education was provided to the interdisciplinary care team using various modalities, including formal didactics, handouts, case examples of asthma scoring, and on-demand individualized learning sessions to bedside clinicians at the time of admission. Tools, including a laminated PAS card and a visual clinical pathway card, were distributed for quick reference. Education was initiated in September 2015 and the implementation start date for postintervention data collection was October 1, 2015 coinciding with the ability to document the asthma severity score in the EMR.
Plan-Do-Study-Act (PDSA) cycles were performed following pathway rollout. Documentation of the patient asthma severity score in the EMR was initially poor and inconsistent with frequent hourly omissions from the patient record. Subsequently, the EMR clinical flowsheet was optimized to allow for improved accessibility to the asthma severity score and ease of charting for the bedside clinicians. Additional educational endeavors were implemented to address identified gaps in clinician knowledge of the new pathway. Finally, an EMR admission order set was created and implemented in January of 2016 to further encourage asthma severity scoring and tiered medication use.
Study population
Patients were eligible for inclusion if they were 2–17 years of age with known history of asthma or reactive airway disease who were admitted to PICU at Comer Children's Hospital with a primary diagnosis of status asthmaticus and receiving continuous inhaled bronchodilator therapy. Exclusion criteria were children with congenital cardiac disease, chronic respiratory conditions, including chronic lung disease or bronchopulmonary dysplasia, tracheostomy, home ventilator, or any child presently intubated and mechanically ventilated or who subsequently underwent endotracheal intubation in the PICU.
Study design and duration
This study used a pre–post intervention design. Preimplementation period was from October 2014 through September 2015, and postimplementation period was from October 2015 through October 2016 coinciding with the availability of the asthma severity scoring tool in the EMR. There were no iterative changes to the stepwise pathway over time; however, the EMR-based admission order set was not available until January 2016. Institutional review board approval was not required for this study as per the University of Chicago Institutional Review Board policies governing quality improvement initiatives.
Data collection
A retrospective pre–post intervention study of continuous bronchodilator transition time using a hospital-based clinical dataset was performed. Clinical-level data migrated from the EMR directly into a clinical data warehouse at the Center for Quality at the University of Chicago were abstracted. The Center for Quality Data Warehouse is a repository of University of Chicago medical data dating back to 2012. The data warehouse team brings together data from disparate sources, including the EMR. Available data include laboratory values, procedure and diagnosis codes, demographics, medications, and visit information.
The International Classification of Diseases 9th and 10th Revision codes along with asthma-related Medicare Severity Diagnosis-Related Groups were used to identify patients with status asthmaticus who were then screened for inclusion and exclusion criteria by manual chart review. For patients who required endotracheal intubation in the PICU, data were collected to assess for clinical complications; however, asthma severity scoring could not be performed after intubation and thus they were excluded from the primary transition time analysis.
Data analysis
The primary outcome was the time required to transition from continuous inhaled bronchodilator therapy (albuterol) to the first 2-h intermittent inhaled dose. Duration of therapy was defined as time interval between physical admission to the PICU, and the time the physician order to transition to every 2 hourly bronchodilator therapy was placed. Secondary outcomes included PICU and hospital lengths of stay; clinical complications, including endotracheal intubation, pneumothorax, cardiac arrest, or death; incidence of PICU readmission; and frequency of adjunct medication therapies used for asthma management. Pearson Chi-square tests for independence, t-tests for independent samples, or Wilcox rank-sum were used to evaluate differences between the two intervention groups. Data were analyzed using R (version 0.99.903) and SQL Server Management (Microsoft, Redmond, WA).
Results
A total of 202 patients were screened for inclusion in the preintervention group and 199 screened in the postintervention group. Seventy-one (35%) patients in the preintervention group and 71 (36%) patients in the postintervention group met exclusion criteria. Specifically, 9 (4.5%) patients in the preintervention and 8 (4%) patients in the postintervention cohorts were excluded due to intubation and mechanical ventilation status. Of note, only two patients in the preintervention group and one patient in the postintervention group required intubation in the PICU after hospital admission.
Following application of inclusion and exclusion criteria, there were 130 and 124 patients analyzed in the pre- and postintervention groups, respectively. Demographics between the two groups were similar (Table 3). Overall compliance with documentation of hourly asthma scoring in the postintervention period was 59%. There was a 4.9-h decrease in the mean transition time from continuous to intermittent bronchodilator use between the pre- and postintervention periods (31.9 versus 27.0, P = 0.033) (Table 4; Fig. 1). Neither the mean nor median PICU LOS was significantly changed between the two groups. Both the mean and median hospital LOS were significantly decreased in the postintervention group by 14.76 h (P = 0.011) and 16.68 h (P = 0.003), respectively.
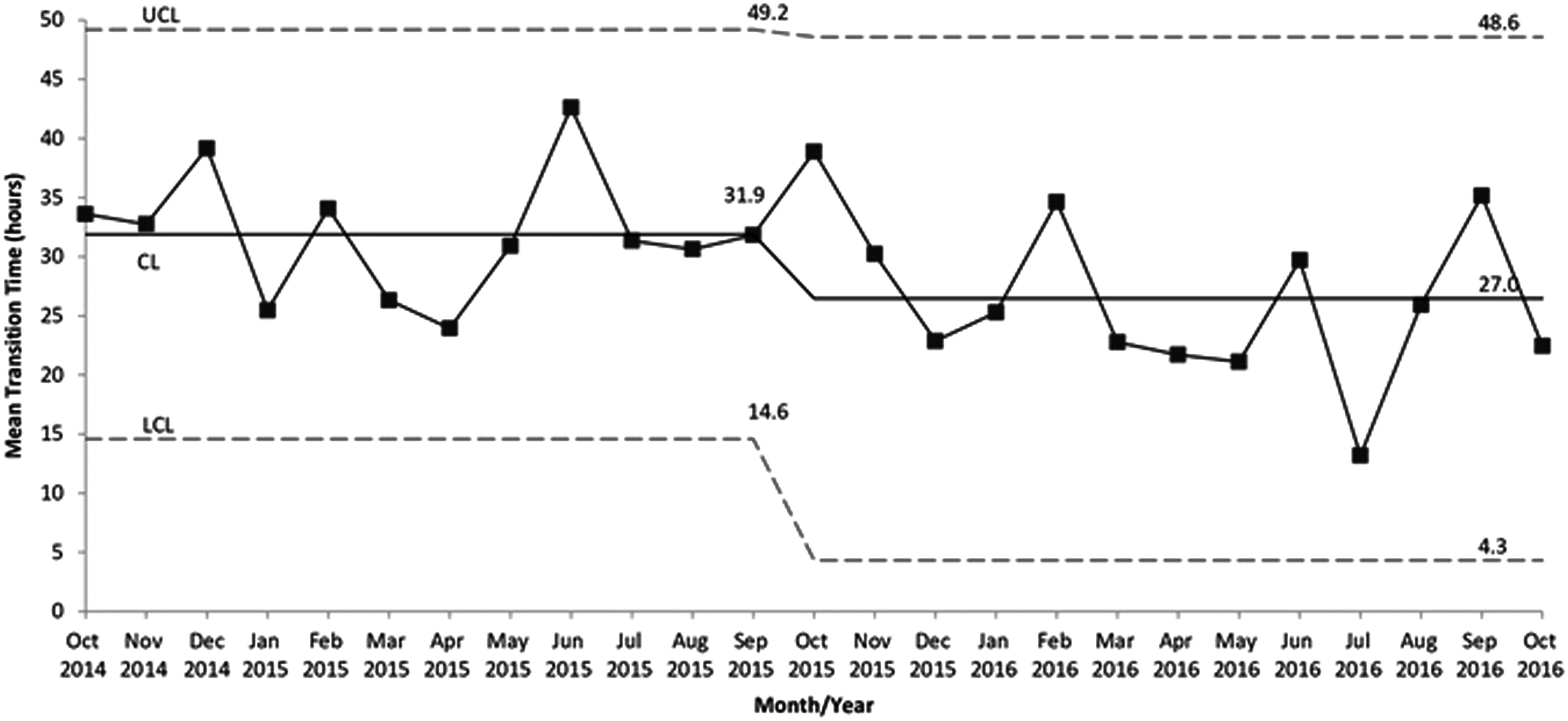
Run chart showing the mean reduction in inhaled bronchodilator therapy transition time following introduction of an asthma severity score-based treatment pathway in the pediatric intensive care unit. CL, center line; LCL, lower control limit; UCL, upper control limit.
SD, standard deviation.
LOS, length of stay; PICU, pediatric intensive care unit.
Frequency of corticosteroid use was 100% in both groups. The use of other asthma medication therapies, including terbutaline, ipratropium bromide, ketamine, and magnesium sulfate were not significantly different between the groups; however, the use of aminophylline was significantly higher in the postintervention group. With respect to complications associated with the intervention, there were no readmissions to the PICU in the postintervention group. Additionally, no patients in either group sustained a pneumothorax, cardiac arrest, or death. The use of BiPAP (Bi-level positive airway pressure ventilation) was significantly higher in the preintervention group compared with the postintervention group (42% versus 28%, P = 0.036).
Discussion
This is the first study to assess the clinical outcomes after the introduction of a severity-tiered treatment pathway for children admitted to the PICU with status asthmaticus. The implementation of a modified asthma severity scoring tool along with a severity-tiered approach to therapy resulted in a reduction in transition time from continuous to intermittent inhaled bronchodilator therapy and a significant reduction in total hospital LOS. These results are consistent with prior protocolized inpatient asthma pathways, which have been shown to reduce duration of bronchodilator use.5,7,9
Although not statistically significant, the average PICU LOS decreased by nearly 5 h in the postintervention group. Extrapolated to the entire postintervention cohort of 124 patients, the overall reduction in PICU LOS equates to 20 fewer PICU days and approximately 86 hospital days saved. Given the high cost of PICU hospital care tied directly to PICU LOS, any meaningful reduction in PICU or hospital LOS can result in reduced cost of care as well as improved hospital throughput.
As expected, 100% of patients in the pre- and postintervention groups received steroids given that steroid administration for pediatric patients with status asthmaticus is considered the standard of care therapy. There were no significant differences seen in other adjunct medication use between the two groups, except for aminophylline. The increase in methylxanthene use in the postintervention group may have been the result of ease of ordering the medication and associated laboratory evaluations as part of the initial order set. However, it is also possible that the increase in aminophylline use reflected a change in clinical practice given the publication of newer data suggesting benefits of methylxanthene use in certain high-risk pediatric patients with refractory asthma. 23 It is notable that the relative frequency of use of specific medication therapy in this study is consistent with recently published data. 24
There were no significant clinical complications observed in either group, and there were no readmissions to the PICU in the postintervention group. This suggests that although patients transitioned sooner, there was no unintended consequence of transitioning before the patients were clinically ready. Additionally, there was no significant difference in PICU LOS between the two groups; however, hospital LOS was significantly reduced. The lack of PICU LOS reduction may have been reflective of a general hospital throughput issue with lack of available inpatient floor beds given that the total hospital LOS was significantly reduced. Additionally, patients who achieved a de-escalation of therapy in the middle of the night are generally not transferred to a general floor bed despite clinical readiness, but rather are transferred in the early morning hours to reduce family disruption caused by middle-of-the-night transfers. The PICU LOS may have been shorter if all children were transferred immediately after clinical readiness was established; however, this is generally not the case and there is inherently some time lag observed to maintain family satisfaction.
The postintervention group had a lower percentage of patients requiring escalation to BiPAP, which may suggest that the use of asthma severity score along with the tiered therapy in the PICU may have averted the need for escalation to noninvasive ventilation with BiPAP. The reduction in BiPAP utilization can result in lower resource utilization from the standpoint of PICU LOS alone. Given that patients who require noninvasive ventilation with BiPAP are not candidates for floor care, the total cost of care and PICU LOS of those requiring noninvasive ventilation will likely be higher. In this study, there was a reduction in noninvasive ventilation use in the postintervention group; however, the study was not designed to determine a causal relationship.
There are several limitations of this study. First, these data represent findings from a single urban academic medical center PICU. However, it is unlikely that the structure and processes of the PICU at the University of Chicago are inherently different compared with other academic medical centers. Additionally, it is possible that the patients in our cohort were in some way uniquely different compared with others. Given the location of the University of Chicago medical campus and the fact that the clear majority of patients cared for in the PICU are from medically underserved communities, it is likely that this population represents the most severe and highest-risk cohort of patients with asthma. As such, the improvements observed in this study may not be as significant in a cohort of patients with less severe illness. However, given the availability of national guidelines for the stepwise therapy for patients admitted with asthma exacerbations, it is likely that these improvements would be replicated in a different PICU. Finally, there was no immediate improvement observed in transition time immediately after implementation of the severity-tiered pathway and scoring system. Once the EMR order set was available, there was a significant reduction in transition time from continuous to intermittent bronchodilator use.
The lack of an electronic order for hourly asthma severity scoring before the implementation of the order set likely contributed to the lack of immediate improvement. The pathway requires asthma scores to cue clinicians to escalate or de-escalate therapy. Without consistent hourly asthma severity scores, there is no objective marker of readiness to transition. As such, until the physical order to perform hourly asthma scores was available, there was no observed improvement. It is unclear whether the order for hourly asthma scoring, or whether the organization of the pathway medication therapies into a single order set was the key driver of improvement. It is worth noting, however, that the medication therapies were organized according to severity tier in the order set, which facilitated ease of ordering and pathway compliance. The order set, combined with the severity scoring and stepwise therapy pathway, likely resulted in clinicians having higher vigilance to the need for assessment of a patient's readiness to transition.
Conclusions
A severity-based stepwise treatment pathway for pediatric patients admitted to the PICU with status asthmaticus can be successfully implemented using an interdisciplinary team of clinicians. Objective assessment of asthma severity allowed clinicians to deliver individualized high-quality care within a structured framework resulting in a reduction of the time required to transition from continuous to intermittent inhaled bronchodilator use. As a result, the overall hospital LOS was significantly reduced.
Footnotes
Acknowledgments
The authors thank the pediatric intensive care unit (PICU) nursing and respiratory teams for their assistance with education and roll-out; Drs. Mark Abe and L. Brenda Giles for their thoughtful critique of the clinical pathway; Dr. Michael Howell for his support with data analytics.
Author Disclosure Statement
No competing financial interests exist.