
Abstract
Background:
A number of studies have highlighted that prenatal adverse events can affect the offspring's health status. We evaluated whether pregnancy complications might affect the respiratory health of the offspring during infancy and childhood.
Methods:
In 2006, all the children (3–14 years, N = 3,907) living in the Viadana district (Mantua, Italy) were surveyed through a parental questionnaire about pregnancy complications (hypertensive disorders, febrile infections, gynecological infections) and early-life and current respiratory diseases. Hospital discharge records for respiratory diseases were obtained for a 6-year follow-up period (2007–2012). Association estimates were adjusted for maternal smoking during pregnancy, maternal age at delivery, type and term of delivery, and other potential confounders.
Results:
A total of 3,617 (93%) children were included in the analyses. Pregnancy complications were significantly associated with higher risk of respiratory diseases during infancy and childhood. In particular, children exposed to gynecological infections were more likely to have bronchitis [odds ratio (OR): 1.48, 95% confidence interval (95% CI): 1.04–2.10], pneumonia (OR: 2.05, 95% CI: 1.10–3.81), and wheezing (OR: 1.49, 95% CI: 1.00–2.23) at 0–2 years; to report asthma (OR: 3.57, 95% CI: 1.59–8.04) and cough/phlegm (OR: 2.68, 95% CI: 1.67–4.31) at the time of the survey; and to be hospitalized for respiratory diseases (hospitalization hazard ratio: 1.74, 95% CI: 1.02–2.97) in the 6-year follow-up. There was a significant association between febrile infections and wheezing in infancy, even in children whose mothers did not use paracetamol or antibiotics during pregnancy.
Conclusions:
This observational study suggests that pregnancy complications, especially gynecological infections, might affect the offspring's respiratory health throughout infancy and childhood.
Introduction
T
Pregnancy complications are health problems that arise during pregnancy and may harm the mother or her offspring. Infections and hypertensive disorders (eg, hypertension and preeclampsia) are common pregnancy complications that have been associated with poor birth outcomes. Despite their potential impact, a limited number of epidemiological studies have investigated the effects of maternal pregnancy complications on the development of respiratory diseases in the offspring during infancy and childhood, and the findings are sparse and sometimes inconsistent.
This study aims at assessing if fetal exposure to hypertensive disorders and febrile and gynecological infections are associated with worse respiratory health conditions in infancy and throughout childhood.
Materials and Methods
Study design and participants
In December 2006, we conducted a survey to investigate the respiratory health of the pediatric population in the Health District of Viadana (Lombardia, Italy), where several chipboard factories are located, to evaluate the impact of air pollution on resident children. 8 All the children (N = 3,907) aged 3–14 years who were enrolled in the school registers were included in this survey. Their families were asked to answer to a standardized questionnaire (freely available at: http://biometria.univr.it/viadanastudy) about the presence of current and past respiratory diseases, risk factors, and lifestyles. Besides its public health objectives, the data offered the opportunity to investigate the associations of adverse events during pregnancy, birth, and infancy with the risk of respiratory diseases.
Most of the questions were taken from internationally validated questionnaires, as previously described. 7 Hospital discharge records for all the children were obtained from the local health unit for the period between January 1, 2007, and December 31, 2012 (6 years), and linked to the questionnaire survey data. 9 A total of 3,854 questionnaires (98.6%) were filled in and returned.
The study protocol was approved by the local ethics committee.
Respiratory outcomes
Respiratory outcomes at 0–2 years
The occurrence of doctor-diagnosed respiratory diseases during the first 2 years of a child's life was assessed through an affirmative answer to one of the options to the following questions: “Has a doctor ever said that your child had one or more of the following conditions during his/her first 2 years of life? (a) bronchitis (b) pneumonia or bronchopneumonia.” Moreover, the occurrence of (c) wheezing in infancy was assessed in case of affirmative answer to: “Has your child ever had wheezing or whistling in his/her chest at any time in the past?” plus reporting that it had happened for the first time when the child was 2 years old or younger.
Current respiratory diseases
The following current respiratory conditions were also considered:
1. Asthma, in case of affirmative answer to: “Has your child ever had asthma?” plus one among: “Has your child had an attack of asthma in the last 12 months?” or “In the last 12 months, has your child used medicines for the wheezing in his/her chest or for asthma (tablets, inhalers, aerosols, or other remedies)?” 2. Allergic rhinitis, in case of affirmative answers to: “Has your child ever had any nasal allergies (including hay fever)?” plus “Does your child still have this nasal allergy?” 3. Cough or phlegm, in case of affirmative answer to: “Does your child cough/bring up any phlegm on most days (4 or more days a week) without common colds or flu?”
Hospitalizations for respiratory diseases
Hospitalizations were coded according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Both primary and secondary discharge diagnoses for diseases of the respiratory system (ICD-9-CM codes: 460–519) were considered to define hospitalization events (Supplementary Fig. S1; Supplementary materials are available online at www.liebertpub.com/ped). The hospitalization rates were obtained by dividing the number of the children with at least one discharge diagnosis for respiratory diseases by the total person-years at risk. For each child, the person-years at risk were computed as the time from the beginning of the follow-up (January 1, 2007) to the day of the first hospitalization for respiratory diseases (if any), the date of cancellation from the local health unit register (if the child had moved outside the local health unit), or the end of the follow-up (December 31, 2012), whichever came first. 9
Pregnancy complications
Information about the occurrence of the following complications during pregnancy was retrospectively collected through the parental questionnaire:
• Hypertensive disorders, that is, high blood pressure (hypertension) for which the mother had to take medicines (yes/no), or preeclampsia (yes/no). • Febrile infections, that is, episodes of fever due to infections (yes/no). • Gynecological infections, that is, gynecological infections for which the mother had to take medicines (yes/no).
Statistical analyses
Categorical variables were summarized with percentage, and differences between groups were tested by chi-squared tests. The associations of each of the three pregnancy complications with respiratory diseases at 0–2 years and current respiratory symptoms were estimated by odds ratios (ORs) with 95% confidence interval (95% CI), obtained using logistic regression models. The associations between hospitalization rates and each of the pregnancy complications were estimated by hospitalization hazard ratios with 95% CI, obtained by using Cox proportional hazard regression models. The proportional hazard assumption was tested for each covariate included in the model.
To test the stability of the associations between maternal pregnancy complications and respiratory health in the offspring, three sets of adjustment variables were considered in the analyses:
Model I. Child's sex, age, person who filled in the questionnaire (mother only/both parents; father only/others) and family's characteristics, that is, parental smoking habits (at least one parent who smokes), nationality (foreign if both parents were born abroad), parental school education level (the highest degree reached among the two parents) as a proxy of socioeconomic status, and familiar history of asthma. Model II. Variables in Model I plus maternal smoking during pregnancy, maternal age at delivery, duration of breastfeeding, and birth characteristics, that is, cesarean-section birth, term of delivery (preterm if the child was born >3 weeks before the due date), and low birthweight (<2.5 kg). Model III. Variables in Model II plus maternal use of antibiotics or paracetamol during pregnancy.
Subjects with missing values on a covariate were deleted listwise from the models.
Two sensitivity analyses were performed: first, we repeated all the analyses on the subset of children younger than the median age (8 years old) to evaluate whether a poor recall of events that occurred during pregnancy might have affected our findings; second, we estimated the associations between febrile infections and respiratory outcomes in the subset of mothers who did not use paracetamol or antibiotics during pregnancy, to investigate a population where confounding and mediation effects by the use of these drugs could be ruled out.
Statistical analyses were performed with STATA 14.2.
Results
Inclusion of subjects in the analysis and missing data
A total of 3,617 children (92.7% of the eligible sample), for whom information on key questions was available (ie, age and sex of the child, person who filled in the questionnaire, and at least one maternal pregnancy complication), were included in the study. A small proportion of subjects did not answer the questions on pregnancy complications, ranging from 0.6% in hypertensive disorders to 2.0% in gynecological infections. The proportion of subjects with missing data in current asthma, rhinitis, or cough/phlegm was about 1.3%–1.4%. The proportion of missing values was higher for respiratory outcomes at 0–2 years, with 8%, 20%, and 11% for wheezing, pneumonia, and bronchitis, respectively.
Association of pregnancy complications with birth characteristics
The characteristics of the children included in the study are listed in Table 1. In total, 7.7% (n = 278), 3.9% (n = 139), and 6.2% (n = 219) of the pregnancies, respectively, were complicated by hypertensive disorders, febrile infections, and gynecological infections, while 86.5% (N = 3,055) were not affected by any of these complications (Supplementary Fig. S2). The children who were exposed in utero to maternal hypertensive disorders were at significantly higher risk of preterm birth, low birthweight, cesarean-section birth, and early breastfeeding cessation. Moreover, mothers who suffered from pregnancy complications, and in particular those who had febrile and gynecological infections, were more likely to use paracetamol and antibiotics during pregnancy (Table 2). The age at delivery and the smoking habits during pregnancy were similar between mothers who did versus did not experience pregnancy complications during their pregnancy.
P values were calculated using logistic regression models, adjusting for sex, age, and person who filled in the questionnaire.
P < 0.05; **P < 0.01; ***P < 0.001.
N is smaller than 3,617 because of missing values.
Association of pregnancy complications with respiratory diseases in infancy and in childhood
The occurrence of doctor-diagnosed bronchitis, pneumonia, and wheezing at the age of 0–2 years was reported for 42.8%, 4.8%, and 16.0% of the children, respectively; the prevalence was higher in children born to mothers who had experienced complications during pregnancy with respect to the other mothers (Table 3). Rhinitis and cough/phlegm were reported in 6.9% and 6.6% of the children, respectively. Current asthma was present in 2.3% of the children aged 6 years or older. The prevalence of asthma and cough/phlegm was higher in the children born to mothers who had had gynecological infections during pregnancy; the prevalence of cough/phlegm was also more frequent in children exposed in utero to febrile infections, while rhinitis was not significantly associated with any of the considered pregnancy complications.
Differences between groups were tested by chi-squared test.
P < 0.05; **P < 0.01; ***P < 0.001.
N is smaller than 3,617 because of missing values.
The analysis on asthma is restricted to children aged ≥6 years.
After adjusting for potential confounders (Model II), the children exposed in utero to maternal hypertensive disorders had more than twofold higher risk of having had pneumonia in infancy compared with nonexposed children (OR: 2.21; P = 0.005). The children born to mothers who experienced gynecological infections were at higher risk of having had bronchitis, pneumonia, and wheezing at 0–2 years (OR: 1.81, 2.31, 1.70, respectively; all P < 0.005) (Fig. 1). The association estimates were not substantially affected by adjustment for perinatal events and maternal use of medicines during pregnancy (Model III). The children exposed to febrile infections in utero had twofold higher risk of having wheezing, compared with children who were not exposed (OR: 2.07; P = 0.001). Noticeably, this association was even stronger in children whose mothers had not used paracetamol or antibiotics during pregnancy (ORs between 3 and 4; P < 0.001) (Supplementary Table S1).
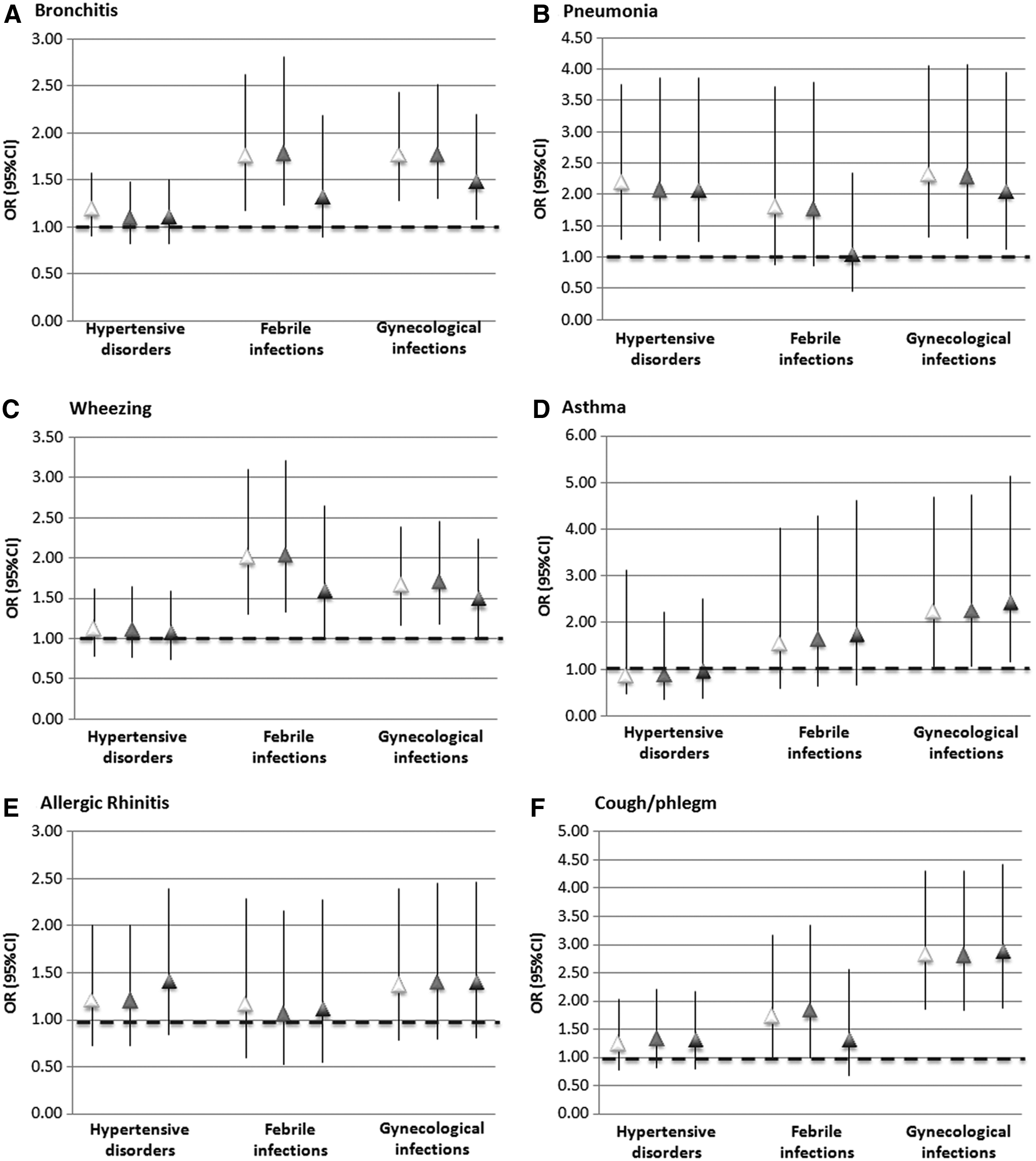
Associations (OR with 95% CI) of fetal exposure to pregnancy complications with
The children who had been exposed to maternal gynecological infections had significantly greater risk of having current asthma (OR: 2.25; P = 0.03) and cough/phlegm (OR: 2.81; P < 0.001) (Fig. 1). Children exposed in utero to febrile infections had a higher risk of having cough/phlegm in childhood compared with children who were not (Model II, OR: 1.83; P = 0.05), but this association shifted to the null when controlling for maternal use of paracetamol and antibiotics in pregnancy (Model III). In utero exposure to hypertensive disorders was not associated with any of the considered respiratory diseases in childhood.
Association of pregnancy complications with hospitalization rates for respiratory diseases in childhood
During the 6-year follow-up, 222 children (6.1%) were hospitalized for respiratory diseases, and the hospitalization rate for respiratory diseases was 10.8 per 1,000 person-years. Children who had been exposed to maternal gynecological infections in utero had a hospitalization rate of 18.1 per 1,000 person-years, which was significantly higher compared with nonexposed children (Table 4). After adjusting for potential confounders (Model II), the risk of being hospitalized for respiratory diseases was significantly higher (hospitalization hazard ratio: 1.69; P = 0.03) in the children exposed to maternal gynecological infections during pregnancy compared with the nonexposed children (Fig. 2). Hypertensive disorders and febrile infections were not significantly associated with hospitalizations for respiratory diseases.
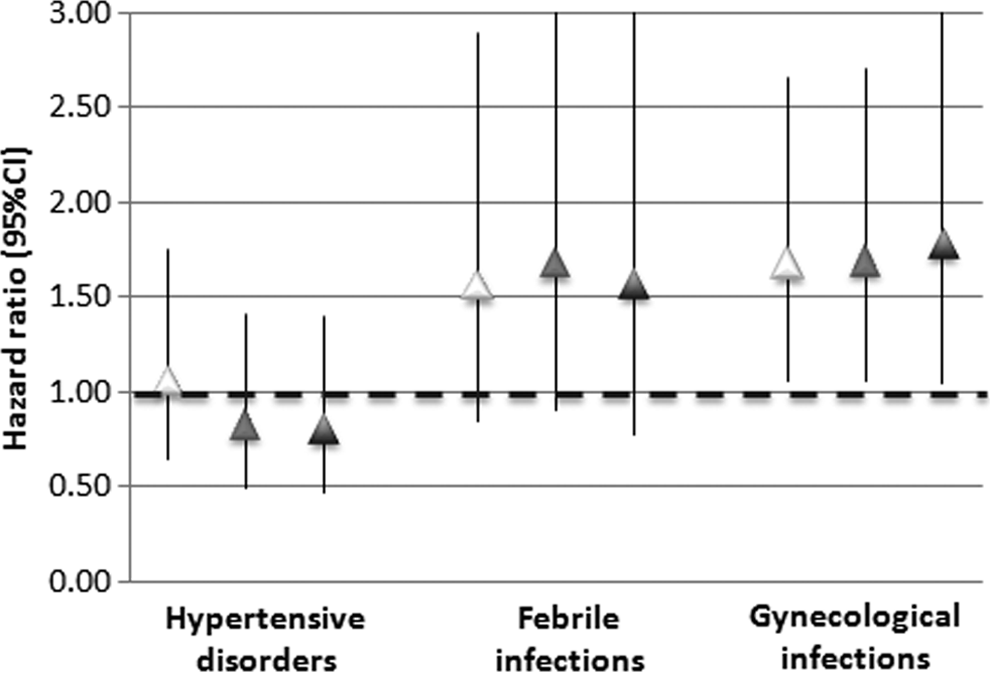
Associations (hospitalization hazard ratio with 95% CI) of fetal exposure to pregnancy complications with the rates of hospitalization in the 6-year follow-up. Model I (white triangles) is adjusted for children's and their families' characteristics; Model II (gray triangles) is adjusted for variables in Model I, plus birth characteristics and duration of breastfeeding; Model III (black triangles) is adjusted for variables in Model II, plus maternal use of paracetamol and antibiotics in pregnancy. The proportion of subjects with complete information who were included in the models ranged from 91% in Model I, to 88% and 85% in Models II and III, respectively. 95% CI, 95% confidence interval.
95% CI, 95% confidence interval.
The sensitivity analyses on the subset of children aged 8 years and younger confirmed the main analyses (Supplementary Table S2).
Discussion
This study investigated if in utero exposures to maternal hypertensive disorders and febrile and gynecological infections during pregnancy affected the respiratory health in infancy and childhood. The outcomes considered are indicators of multiple aspects of the respiratory health of the offspring throughout different ages of development, ranging from early-life conditions (ie, pneumonia, bronchitis, and wheezing) assessed retrospectively, to the presence of asthma, rhinitis, and chronic cough in school age reported at the time of baseline investigation, to the occurrence of hospital admissions for respiratory diseases, which were assessed prospectively using administrative hospital discharge records.
Hypertensive disorders and infant pneumonia in the offspring
Hypertensive disorders, including gestational hypertension, are not uncommon during pregnancy. 10 Severe gestational hypertension and preeclampsia are often treated with preterm cesarean section, and are associated with prematurity, low birthweight, and early breastfeeding cessation. In the United States, hypertension has been reported in 8% of women in reproductive age, and about half of these took antihypertensive drugs. 11 In our sample, we found a similar prevalence of hypertensive disorders during pregnancy.
Our results indicate that in utero exposure to maternal hypertensive disorders doubled the risk of pneumonia in infancy: this association was not mediated by preterm or low birthweight (Supplementary Table S3), and it was independent from other perinatal events (eg, cesarean section or duration of breastfeeding). However, hypertensive disorders were not associated with asthma or other respiratory disorders or hospitalizations at school age suggesting that, despite their impact on perinatal outcomes, it is unlikely that any potential effect on respiratory health persists beyond infancy.
Other studies, including the Oslo Birth Cohort Study and Avon Longitudinal Study of Parents and Children, reported no or weak associations of hypertensive disorders with childhood asthma incidence or hospitalizations.12–19
Since expecting mothers who suffer from preeclampsia have cytokine profiles favoring a Th1 phenotype, it is possible that exposure to hypertensive disorders might protect the offspring from the development of allergic diseases. 20
Maternal febrile infections and respiratory health in the offspring
Children born to mothers who had suffered from febrile infections during pregnancy (3.8% in our study) were at greater risk of wheezing at 0–2 years.
Paracetamol and antibiotics are commonly prescribed for febrile diseases in expectant mothers. Several authors have reported a positive association of exposure to these drugs in utero and infancy with the occurrence of wheezing and asthma in childhood.19,21–24 However, the causality of this association is still under debate and it has been attributed by some authors to “confounding by indication,” that is, respiratory infections may prompt drug prescription and, at the same time, predispose to the onset of respiratory diseases later in life.25,26 In our analysis, the association between fetal exposure to febrile infections and wheezing shifts toward the null when controlling for maternal use of paracetamol and antibiotics during pregnancy in Model III. This may be explained by the collinearity between the occurrence of infections with fever and the use of these medicines. However, the fact that the association between maternal febrile infections and wheezing in the offspring was confirmed in children who had not been exposed to these drugs during pregnancy suggests that febrile infections have, at least in part, an independent effect on the offspring's respiratory health that is not mediated by paracetamol or antibiotics.
There is no clear mechanism through which in utero exposure to febrile infections might translate into adverse respiratory health effects in childhood. Toxins from the infectious agent might also act indirectly through maternal mediators of inflammation, which can pass through the placenta to the amniotic fluid and be absorbed in immune-reactive forms by the fetus. 27 Exposure to high levels of proinflammatory cytokines following maternal infections might deregulate the programming of the lung function and the immune system.
Gynecological infections and respiratory health in infancy and childhood
Nearly 90% of gynecological infections reported by mothers during pregnancy are caused by Candida, while Trichomonas, Chlamydia, and Herpes accounted for about 1% to 2% of reported cases each. 21 Children born to mothers who reported gynecological infections in pregnancy had a significantly greater risk of having wheezing, bronchitis, and pneumonia in infancy (+70%, +80%, +130%, respectively), a greater frequency of asthma and cough/phlegm at school age (+125% and +180%, respectively), and +70% greater risk of hospitalization for respiratory diseases, compared with children whose mothers did not report gynecological infections in pregnancy. All these associations were independent from the use of medicines during pregnancy and birth characteristics.
Other studies reported that exposure to gynecological infections is significantly associated with wheezing, asthma, and atopic dermatitis in childhood,21,28–30 suggesting that it might have a role in the pathogenesis of respiratory and atopic diseases.
A potential mechanism for this association is that exposure to altered vaginal microflora might negatively affect the development of the gut microbiota in the offspring. In fact, according to the microflora hypothesis of allergic diseases, 31 the endogenous microbiota plays an important role in the shaping of the immune system and the development of immune tolerance in newborns.
The microbiota colonizing the infant after birth originates mainly from the mother. Despite an initial microbiome being already present at birth, 32 there is evidence that microflora of the maternal cervical and vaginal tract have a crucial role for the physiological establishment of the offspring's microbiome.32,33
Our results support the hypothesis that the transfer of pathogenic vaginal microbiota may impair the physiological microbial colonization, either in the airways or in the gut, and affect the children's susceptibility to develop allergic and respiratory diseases.2,34–36
Comparison across models with different adjustment sets
The median proportion of subjects with complete information for all the covariates ranged from 89% to 83% in Models I and III, respectively. For all the analyses done (except for Model III for the analyses on febrile infections that was previously commented on), there was a good consistency of the associations for the crude and the adjusted analyses (Models I, II, and III), which suggests that missing data did not bias our analyses. On the contrary, similar association estimates and confidence intervals across the different adjusted models also indicate that collinearity between exposures and covariates, if any, only influenced to a minor extent our analyses.
Limits and strengths
One of the limitations of this study is that the data were not originally collected to investigate the association of respiratory diseases with pregnancy complications. For this reason, we had no data to assess the type and causes of febrile and gynecological infections, the medication used to treat them, as well as the severity and time of onset of hypertensive disorders. Moreover, information on pregnancy complications and respiratory diseases was collected retrospectively or cross sectionally using a parental self-administered questionnaire, and clinical and laboratory data were not available. This could raise issues of recall bias, especially for what concerns perinatal events and diseases reported at 0–2 years. It is possible that mothers whose children experienced problems during early life might more precisely remember events that occurred during pregnancy. On the other hand, pregnancy events and infant diseases have a great impact on both the expectant mothers and their families, and are thus likely to be accurately recalled. 37 Moreover, the sensitivity analyses restricted to children younger than 8 years were consistent with the main analyses. Nonetheless, we acknowledge that our analyses cannot ignore recall bias as a possible explanation of our study findings.
Compared to parent-reported respiratory diseases and symptoms, data on hospitalizations were derived from hospital discharge records and they referred to a prospective 6-year follow-up period, and are thus a more objective proxy of children's susceptibility to develop severe respiratory conditions.
Strengths of this study are the inclusion of a large number of individuals, the great participation of the children's families to this survey, which had an outstanding response rate, and that the analyses were controlled for several confounders and potential perinatal and familiar risk factors for respiratory diseases. Nonetheless, there is still the possibility that the associations found are due to a common cause to both pregnancy complications and offspring's respiratory diseases, such as poverty or social status of the household. These factors might, for example, influence nutritional and living conditions of both the mother during pregnancy and the child during life. Even if our models were adjusted for several indicators of socioeconomical status (eg, parental academic achievement, smoking habits, nationality), we cannot entirely rule out residual confounding.
Conclusions
The current study supports the hypothesis that in utero exposures to pregnancy complications affect the respiratory health of the offspring in infancy and childhood, and that they might interfere with perinatal development of the respiratory and immune systems through different biological mechanisms. Pregnancy gynecological infections necessitating medication were associated with severe respiratory disease requiring hospitalization. The consistency among the effects of this complication on a wide range of respiratory outcomes in the offspring, from early infancy to childhood, supports its clinical relevance. Prospective birth cohort studies shall be performed to confirm these findings and clarify the mechanisms underlying these associations.
Footnotes
Acknowledgments
The Viadana survey was funded by the Local Health Unit of Mantua and by the Province of Mantua (Italy). The sponsors had no involvement in (1) the study design; (2) collection, analysis, and interpretation of the data; (3) the writing of the report; and (4) the decision of publication. All the analyses were performed at the University of Verona. We wish to dedicate this work to Prof Roberto de Marco, who prematurely passed away in 2015. We miss his brilliant scientific thinking and his extraordinary leadership.
Authors' Contributions
This is a secondary analysis of data from the Viadana study, which was conceived, planned, and carried out by Professor Roberto de Marco, P.R., A.M., and V.P. G.P. conceived the hypothesis for the present study, planned and performed the statistical analyses, and drafted the first version of the manuscript. All the authors critically reviewed the manuscript with important intellectual content.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.