
Abstract
Pediatric recurrent wheezing is a common disorder with potential asthma risk; however, its diagnosis much relies on physician's subjective evaluation. Hence, efficient noninvasive biomarkers are in great need. In this retrospective study, blood routine test was analyzed in 143 wheezing children and 137 control individuals, and various cell types were discriminated and counted. Total IgE in plasma was detected using enzyme-linked immunosorbent assay. Receiver operating characteristic curve was plotted and area under curve (AUC) was calculated to evaluate the clinical potential of both indexes for diagnosing pediatric recurrent wheezing. The theoretical cutoff values for both indexes were also calculated using a Youden index. The results showed that neutrophil significantly increased in wheezing children, whereas lymphocyte decreased sharply. Total IgE, neutrophil–lymphocyte ratio (NLR) and platelet–lymphocyte ratio (PLR) were significantly elevated in wheezing patients. Besides, NLR and PLR were found unchanged in different genders. The results showed that NLR (AUC = 0.647) and PLR (AUC = 0.628) were able to discriminate recurrent wheezing. Cutoff for NLR was 0.98 (Youden index 24.8%) and cutoff for PLR was 116.4 (Youden index 19.4%). The mentioned evidence supported NLR and PLR as potential diagnostic indexes for pediatric recurrent wheezing.
Introduction
T
Our group has been working on biomarker development for pediatric recurrent wheezing. Previously, we have reported that extracellular miR-21 and miR-26a are increased in wheezing children and can serve as plasma biomarkers for recurrent wheezing. 4 These increased miRNAs are further confirmed in pulmonary inflammation animals. However, such molecular biology tests including isolation of extracellular RNAs and reverse transcription-quantitative polymerase chain reaction (RT-qPCR) are not widely available in clinical daily practice of children hospitals. Hence, we are more interested in developing some objective indexes derived from routine clinical practice. More importantly, as an ideal disease biomarker, output data of individual pediatric patient should be displayed as absolute digitals instead of relative expression against control group, which we developed before.
Ratio of leukocyte differential counts in peripheral blood has been used to derive simple index, such as the neutrophil–lymphocyte ratio (NLR) and the platelet–lymphocyte ratio (PLR). As a diagnosis index, NLR was initially proposed by Goodman in suspected appendicitis, 5 and widely used as a disease marker. For instance, higher NLR was found positively correlated with atrial septal aneurysm, 6 also NLR was considered better predictors of bacteremia than routine parameters such as C-reactive protein (CRP) level, white blood cell (WBC) count and neutrophil count. 7 NLR in humans (or heterophil–lymphocyte ratio in birds, reptiles, and some amphibians, or neutrophilic granulocyte–lymphocyte ratio in fish and some other amphibians) is extensively accepted as a sensor in peripheral, circulating blood for physiological stress in free-living vertebrates. 8 NLR is also recommended as indicators of systemic inflammation. Both NLR and PLR have been shown to have prognostic value in various cancer 9 and cardiovascular diseases. 10 Particularly in respiratory diseases such as acute pulmonary embolism, 11 this kind of ratio is proven to be indicative. NLR obtained at the initial diagnostic stage is a useful marker to discriminate patients with pulmonary tuberculosis from patients with bacterial community-acquired pneumonia in an intermediated TB-burden country. 12 Admission NLR at the emergency department predicts severity and outcome of community-acquired pneumonia with a higher prognostic accuracy as compared with traditional infection markers such as neutrophil count, whole blood cell count, lymphocyte count, and CRP level. 13 NLR and PLR have gradually become a new addition to the long list of these inflammatory markers.
However, so far little is known whether ratio of leukocyte differential counts in peripheral blood could become an index for discrimination of pediatric recurrent wheezing. But the local inflammatory events were formally indicated before, and the literature reported that the percentage of lymphocyte count decreased whereas percentage of neutrophils increased in bronchoalveolar lavage fluid (BALF) from symptomatic asthma children compared with paucisymptomatic children. 14 Hence, we intend to evaluate whether NLR and PLR can help diagnosis for pediatric wheezing. Owing to the important role of recurrent wheezing as subjective characteristic for pediatric asthma diagnosis, the search for a sound biomarker in pediatric recurrent wheezing can even further help physicians with a better practice for pediatric asthma discrimination in future, hence is of much clinical priority.
Materials and Methods
Subjects
In this study, the laboratory results of 143 wheezing patients and 137 control individuals were retrospectively enrolled. These patients were recruited during their hospital commitment in the Department of Respiratory Medicine of Xi'an Children Hospital. Both groups were <12 years old during recruitment. Balance of patients' age distribution was analyzed and there was no difference of patients' ages between the 2 groups (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/ped). Demographic and clinical characteristics of control and study population are shown in Table 1.
Age range was displayed as median (IQRs, Q1–Q3).
IQRs, interquartile ranges.
Since both pediatric asthma and recurrent wheezing in practice were commonly complicated with LRI, the control group in this study consisted of children suffering from bronchopneumonia or bronchitis only. The study group was specifically diagnosed with pediatric wheezing and also had clinical manifestations of bronchopneumonia or bronchitis, defined as “wheezing+LRI” group. Wheezing with more than 3 episodes was considered as recurrent wheezing in our study. All subjects were without congenital heart diseases, intestinal infection, upper respiratory diseases, complications with liver or kidney injury or Kawasaki disease, and any type of malignancy. Children with wheezing caused by abnormal airway development, airway foreign body, tumor, and respiratory tuberculosis were excluded. The children were also known to neither have any allergy attack nor medications within 6 months before the collection of samples.
The research involving human subjects is in accordance with the Declaration of Helsinki (revised in 2013) and was approved by the Xi'an Children Hospital and Xi'an Jiaotong University Ethics Committee. Written informed consents were obtained from parents as well as guardians of the participants.
Blood collection and differential cell count
Blood at volume of 2 mL was collected using citrate-containing vacuum blood drawing tubes, and was further centrifuged at 1,800 g for 20 min at 4°C to obtain plasma. Plasma was divided into 200 μL aliquots and stored immediately at −80°C. Differential cell count was performed using a fully automatic 5-classify blood cell analyzer (SYSMEX 800i, Japan). Total leukocyte cell counts, absolute counts of differential leukocytes including lymphocytes, eosinophils, and neutrophils, and platelets counts were automated in each individual.
Enzyme-linked immunosorbent assay
Human total IgE was detected by an enzyme-linked immunosorbent assay kit following manufacturer's instruction (Bethyl Laboratory). In brief, plasma samples were captured by a coating antibody, blocked by buffered BSA solution, and further bound with detecting antibody conjugated with horseradish peroxidase. Chromogenic 3, 3′, 5, 5′-tetramethylbenzidine substrate was added for development, which was stopped by sulfuric acid and finally detected at 450 nm by a microspectroreader (Thermo). Series diluted standard protein of human total IgE was used for the 4-parameter standard curve. Both the test samples and standard protein were prepared in duplicates. A mean of absolute concentration of total IgE from each plasma sample was hence calculated.
Statistics
Data are presented as means ± standard deviation. According to specific situation, differences between 2 groups were analyzed by Student's t-test or Mann–Whitney test. The ability of biomarkers to discriminate patients from control individuals was assessed by receiver operating characteristic (ROC) curves. Area under curve (AUC) was estimated to evaluate the predictive power. Statistically value of P < 0.05 was considered significantly different except in balance test in which P > 0.10 was considered to be a balanced age distribution between 2 groups. Statistical calculations were performed with SPSS software (version 13.0).
Description of some of the methods is reproduced from our previous work. 4
Results
Differential leukocytes in peripheral blood from children with recurrent wheezing
Total leukocyte cell counts, absolute and relative counts of differential leukocytes including lymphocytes, neutrophils, and eosinophils, and platelets were automated in our study. The results showed that there was no difference in total number of leukocytes, eosinophils, and platelets in peripheral blood from wheezing children. However, the absolute and relative counts of neutrophils significantly increased in wheezing children. In the meantime, the absolute and relative counts of lymphocytes decreased sharply (Fig. 1).

Differential leukocyte count in peripheral blood from wheezing children. Counts of total leukocyte
NLR and PLR in peripheral blood from children with recurrent wheezing
Total IgE, a well-accepted index for pediatric recurrent wheezing, was found significantly enhanced (P < 0.0001) in the wheezing children of our study (Supplementary Fig. S2). In addition, the absolute NLR and PLR were calculated in this study (Fig. 2A, B). The results showed that NLR and PLR significantly increased in wheezing children compared with control group. Besides, there was no difference between male and female individuals in this study, which suggested that the NLR and PLR kept stable in different genders and hence was possible to serve as disease biomarkers (Fig. 3).

Neutrophil–lymphocyte ratio and PLR as disease biomarker in peripheral blood from wheezing children.
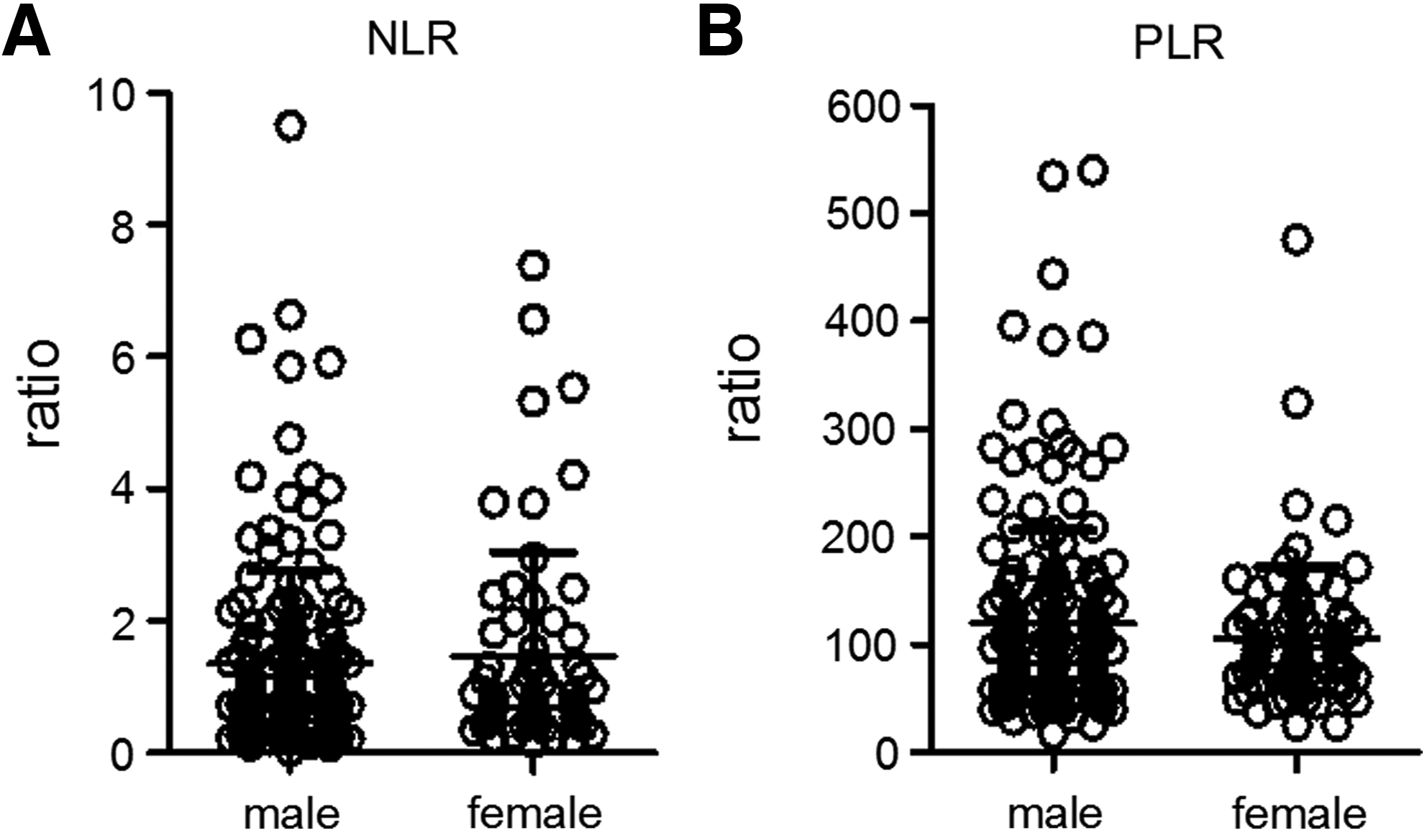
NLR and PLR in different genders. NLR
Evaluation of NLR and PLR in patients' blood for recurrent wheezing diagnosis
ROC analysis was performed for these 2 indexes (Fig. 2C), and AUC was calculated. The results showed that both NLR (AUC = 0.647, 95% confidence interval 0.582–0.711) and PLR (AUC = 0.628, 95% confidence interval 0.563–0.693) can serve as sound biomarkers for recurrent wheezing discrimination, and were of potential clinical significance (both P < 0.001).
The theoretical cutoff value of NLR and PLR for wheezing diagnosis
The theoretical cutoff value for both indexes could be calculated using a Youden index, which was defined as the percentage of specificity plus sensitivity minus 1, and the calculated cutoff values with the largest Youden index are shown in Table 2. Cutoff for NLR was 0.98 (sensitivity 68.6%, specificity 56.2%, Youden index 24.8%) and cutoff for PLR was 116.4 (sensitivity 47.1%, specificity 72.3%, Youden index 19.4%). However, these cutoff values only represented the theoretical condition, without concerning the priority that the physicians might pay in clinical practice. As the cutoff value increased, the specificity increased and sensitivity decreased. Once any 1 of the 3 parameters was settled, the other 2 could be easily found in ROC plot. Physicians could choose optimal cutoff values for each index according to their own priority in sensitivity and specificity.
NLR, neutrophil–lymphocyte ratio; PLR, platelet–lymphocyte ratio.
Discussion
In this work, we evaluated the NLR and PLR indexes in recurrent wheezing, but did not further study the mechanism underlying the altered NLR and PLR during recurrent wheezing. Concerning immune cell trafficking, there is a possible explanation for increased NLR in peripheral blood here. In previous reports, during infection or exacerbations of airways, tissue neutrophils were found increased and released from these compartments into the blood stream. Lymphocytes also traffick out of circulating blood to compartments such as the skin, spleen, and lymph nodes, where they can be more useful during immune response, for example, the activated (due to antigenic stimulus) memory T cells are recruited to the lung from the blood system and act as effector cells for local inflammation. 15
Ideal diagnosis marker is stable despite patients' gender, age, and medicine history. In normal young children, researchers found no age-related differences in the differential count of BALF macrophages and lymphocytes in 55 children aged between 3 and 16 years. 16 Others also found no age-associated change in the differential count and concentration of airway leukocytes in 33 normal children aged between 2 and 17 years. 17 However, there are still some factors that should be taken into consideration before performing NLR test for disease diagnosis. For example, it was reported that NLR was significantly altered in population suffering from sleep apnea 18 (although this disorder is much more popular in middle-aged adults rather than children) and chronic tonsillitis. 19 NLR might also vary to some extent in different ages and body mass index. 20 In addition, equipment dependence should also be considered because NLR and PLR as the calculated ratio largely depends on the cell counting process offered by the automatic cell counter.
NLR and PLR are objective ratios calculated using absolute count of neutrophils or platelets to lymphocytes. Their superiority over other traditional indexes includes the fact that it is less likely to be influenced by various physiological conditions such as dehydration and exercise, which may easily affect absolute count of differential leukocyte cells. Moreover, NLR as an integrated reflection of 2 distinctive yet complementary immune pathways is more predictive than either parameter alone. 21
NLR and PLR are easy to integrate in daily clinical practice and without extra costs, hence we consider this a very ideal index for diagnosis. The measure of this index is simple, reliable, and can be clinically incorporated into current staging algorithms. Here, these indexes were surprisingly elevated in blood of pediatric asthma patients with no other possible causes of chronic pulmonary disease. We evaluated NLR and PLR to be sound objective indexes for diagnosis of recurrent wheezing. Since NLR and PLR detection is very convenient using automatic equipment, we strongly recommend the physicians pay attention to this index from now on. Moreover, to further increase the sensitivity and specificity for diagnosis, the possible use of a combination of NLR and PLR with some other lower airway inflammation biomarkers such as fractional exhaled nitric oxide or others is highly encouraged.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (grant Nos. 81401289 and 31601033), Postdoctoral Science Foundation of China (2015 M580858), and Shaanxi Health Research Project (grant No. 2014D48).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.