
Abstract
Background:
Preschool wheezing is common and many children experience exacerbations and are well in between. Raised blood eosinophils in older children are associated with exacerbation-prone wheeze, but there are currently no biomarkers to predict near-future exacerbations in preschoolers. There is evidence suggesting that eosinophils are acutely activated during an exacerbation using urinary markers, however, it is unknown whether blood eosinophil numbers fluctuate between the time of an exacerbation and stable disease.
Objective:
To investigate whether, in children with preschool wheeze, blood eosinophil numbers are different during an acute wheezing episode compared with periods of stable disease.
Methods:
Blood samples were taken from children aged 10 months to 6 years, presenting with acute, doctor-diagnosed wheeze, and tested for absolute leukocyte differential cell numbers. A repeat blood sample was obtained in a subset of children after full recovery.
Main Outcome Measure:
Difference between blood eosinophil counts during an acute wheezing episode and after recovery (stable disease) was also obtained.
Results:
Eighty-five children participated in this study, with 68 recruited during an acute wheezing episode (median absolute blood eosinophil numbers 0.10 × 109/L [range 0.00–2.41]) and 17 healthy controls. There was no significant difference in absolute blood eosinophil numbers between the acutely wheezy children when compared with the controls (median 0.17 × 109/L range 0.00–0.83). Absolute blood eosinophil numbers during stable disease were significantly greater (median 0.43 × 109/L; range 0.12 × 1.25 × 109/L) compared with periods of exacerbation (median 0.11 × 109/L range 0.01–1.10) in 20 children in whom paired blood samples were available. Absolute blood lymphocyte numbers were also higher during periods of stable disease, whereas absolute blood neutrophil numbers were higher during the exacerbation.
Conclusions:
Greater numbers of blood eosinophils are present during stable disease compared with the exacerbation state. This is an important consideration when planning future studies using blood eosinophils as a biomarker in wheezy preschool children.
Introduction
W
One important clinical difficulty when dealing with wheezy preschoolers is how to identify children with exacerbation-prone wheeze for a trial of preventer medication. Inhaled corticosteroids are the first line preventer treatment recommended by the British Thoracic Society/Scottish Intercollegiate Guideline Network and Global Initiative for Asthma guidelines.4,5 However, it is estimated that only approximately half of all young children respond to this treatment.6,7 In addition, there are concerns regarding potential side effects of this treatment specifically the reduction in growth velocity, 8 resulting in reluctant prescribing and adherence to this medication.
A major clinical advance would be the identification and validation of a widely available biomarker to identify children at high risk of recurrent severe exacerbations. To date, no such biomarkers have been described, but blood eosinophils have been shown to predict exacerbation frequency in school-age children and adults with asthma.9–11 In addition, eosinophilic asthma is predictive of corticosteroid responsive disease. 7 Elevated blood eosinophils12,13 have also been shown to be a risk factor for persistence of preschool wheeze into older childhood. Thus, blood eosinophils are a promising candidate to be studied as a potential biomarker of corticosteroid responsive disease in preschool children. However, little is known about fluctuation of blood eosinophil numbers, depending on whether the child is acutely wheezy or in a period of stable disease. This is an important issue to address, as this would affect the timing of blood sampling in future studies involving wheezy preschool children.
Therefore, our principal research aim was to investigate whether blood eosinophil counts (and neutrophil and lymphocyte counts) differed between an acute wheezing episode and after recovery in preschool children.
Materials and Methods
Participants
We report a prospective observational study. Between October 2014 and May 2015, children aged between 10 months and 6 years, treated in the children's emergency department at University Hospitals of Leicester NHS Trust (Leicester, United Kingdom) for an exacerbation of doctor-diagnosed wheeze, were eligible to participate if they had at least 1 previous parent-reported episode of wheezing. Children with a presumed clinical diagnosis of bronchiolitis or those with complex medical problems, including moderate to severe prematurity, were excluded. Children who had received oral corticosteroids for more than 24 h before potential recruitment were not approached due to the systemic corticosteroid effect on blood eosinophil numbers. 14
Parents were approached at the earliest opportunity after registering their child in the emergency department. Information was gathered regarding the child's wheezing history and currently prescribed asthma medications. In children where a clinically directed blood test was performed, an additional sample of blood was taken to measure absolute differential leukocyte numbers. In the remaining children, either a blood sample was drawn by venepuncture or finger prick, depending on parental preference.
Parents were asked for permission to approach them again for a repeat sample once their child had completely recovered from the acute wheezing episode no earlier than 4 weeks following discharge from hospital. All blood samples were taken in accordance with the infection control policies at our hospital and the assistance of a play specialist was sought to minimize distress to the children wherever possible. Data on subsequent wheezing episodes and unscheduled healthcare visits due to wheeze were also collected either at the follow-up visits in hospital or via the telephone at times and dates agreed with the parents.
Control participants who had no previously documented or parent-reported wheezing episodes or significant comorbidities were recruited from preoperative assessment clinics before routine ear, nose, and throat surgery. Blood samples were taken in the anaesthetic room during induction of anesthesia from the indwelling intravenous cannula placed by the anesthetist. The Research Ethics Committee (Nottingham, United Kingdom) approved all aspects of this study (NRES reference 09/H043/92). Parents or legal guardians provided informed, written consent. The study design is summarized in Fig. 1.
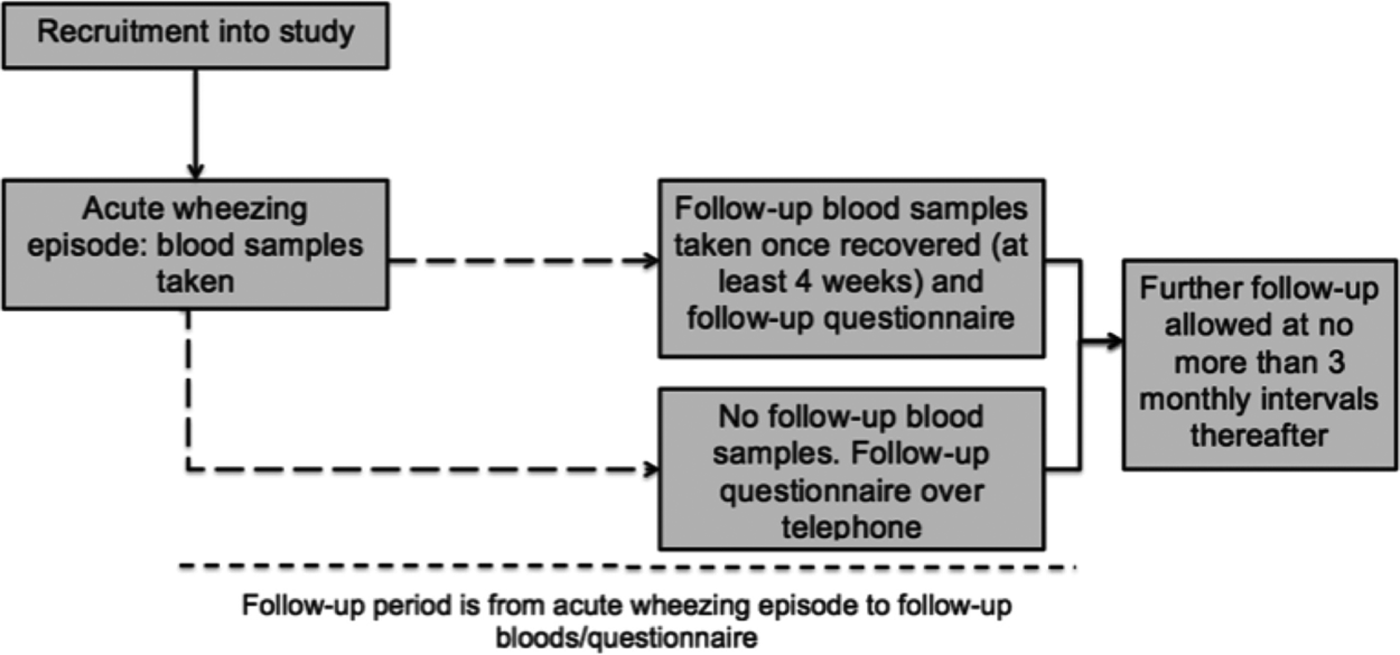
Study design.
Laboratory testing
Blood samples were processed in our hematology laboratory or by a near patient testing full blood count analyzer (Sysmex xs800i: Sysmex Europe GmbH, Norderstedt, Germany) in our emergency department. This equipment uses fluorescent flow cytometry to determine a leukocyte differential cell count. 15 The device is checked, calibrated, and quality controlled daily by our hematology laboratory personnel.
Exacerbation frequency
An exacerbation was defined as an episode, in which the child had become acutely wheezy or breathless necessitating the use of regular reliever medication. The episode needed to last at least 24 h to exclude events of exercise-induced wheeze or breathlessness only.
Information on exacerbations was collected prospectively in the following way: families were contacted by telephone no earlier than 4 weeks after recruitment to confirm willingness for the child to undergo repeat blood sampling. Information regarding exacerbations was gathered over the telephone in those not returning for a repeat blood sample. The ethical approval for this study required that a period of at least 3 months elapsed between telephone follow-ups thereafter. We also cross-checked for attendances to our hospital with wheezing on relevant hospital databases.
We compared the occurrences of near-future exacerbations between children with absolute blood eosinophil numbers ≥0.3 × 109/L and <0.3 × 109/L as 2 recent studies suggested that this cutpoint predicted exacerbation prone asthma in older children and adults.9,10
Statistical analyses
The analyses were performed using Statistical Package for Social Sciences version 22 (SPSS, Inc., Chicago) and GraphPad Prism version 6.04 (GraphPad Software, Inc., CA). Absolute blood eosinophil, neutrophil, and lymphocyte numbers were not normally distributed, therefore, nonparametric statistical tests were used. The Mann–Whitney U-test was used to investigate differences in absolute blood leukocyte differential cell numbers between the groups, and the Wilcoxon signed-rank test was used to probe for differences in paired data. Significance was assessed at the 0.05 level.
Results
Participants
During the study period, 181 families of children fulfilling the inclusion criteria for acute preschool wheeze were approached, of which 74 agreed to participate and an adequate blood volume was obtained from 68 children, 36 by venepuncture and 32 by finger-prick sampling. We found no significant differences in absolute blood eosinophil or neutrophil numbers between children with acute wheeze who had or who had not received systemic corticosteroids before their blood sample being drawn (data not shown). The consort recruitment diagram is shown in Fig. 2. Seventeen control children were also recruited. The demographic and clinical characteristics of the children who participated in the study are shown in Table 1. Twenty families agreed to repeat blood sampling when the child was recovered and well.
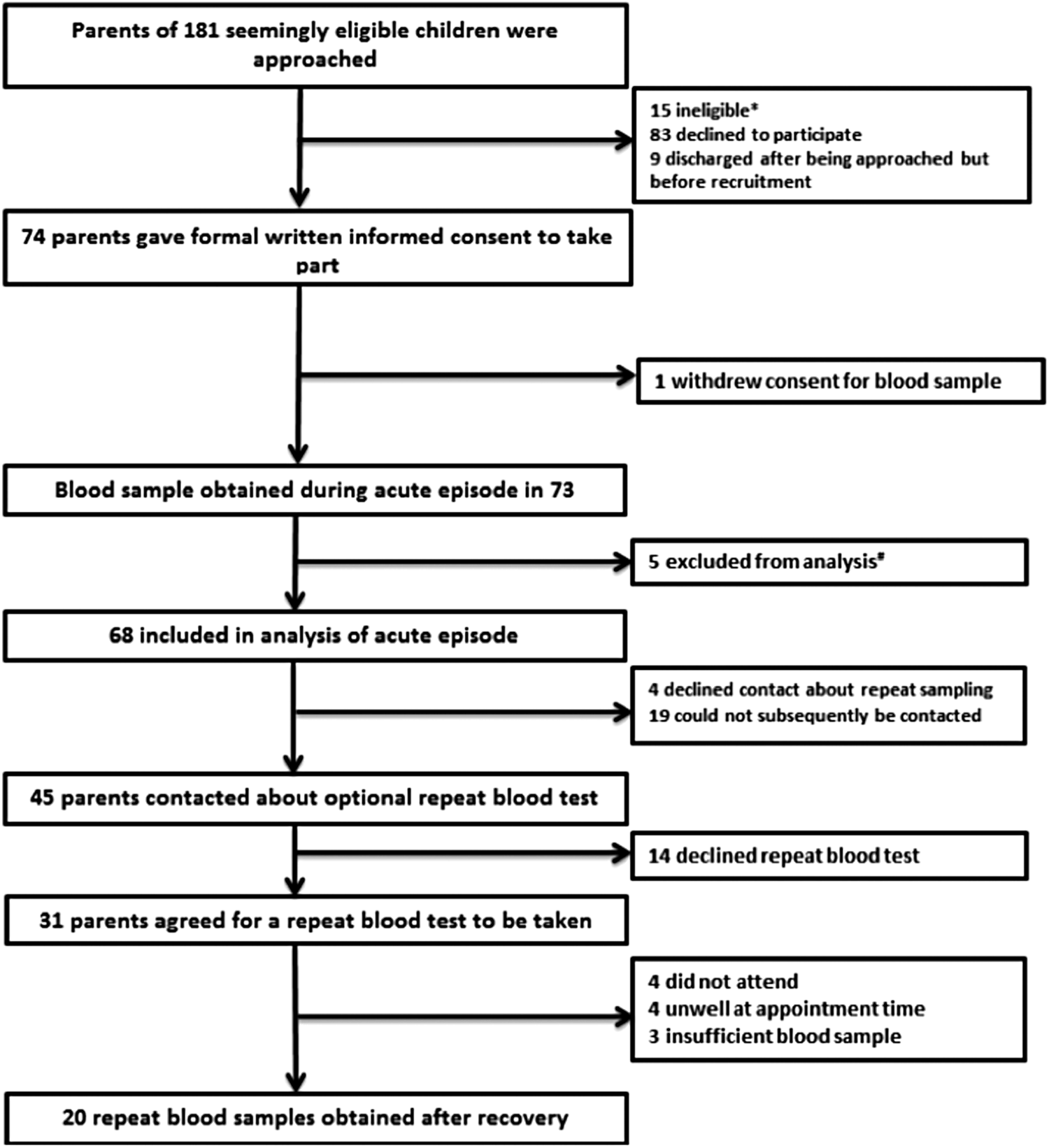
Recruitment algorithm. *receiving systemic steroids >24 hours (n = 7), wheeze not confirmed by clinician (n = 6), parents did not speak English (n = 2); #insufficient sample obtained for FBC analysis.
N = number of samples available. All data are presented as median (range) unless otherwise specified.
Atopic status determined by parental report of doctor-diagnosed eczema or allergic rhinitis.
BTS, British Thoracic Society; TBE, total blood eosinophil; TBL, total blood lymphocyte; TBN, total blood neutrophil.
Comparison of absolute blood leukocyte differential cell numbers between acute and stable disease
Paired samples were available for 20 children. During stable disease, absolute blood eosinophil and lymphocyte numbers were significantly higher compared to the time of the exacerbation. In contrast, absolute blood neutrophil numbers were significantly lower during stable disease (Table 2 and Fig. 3).
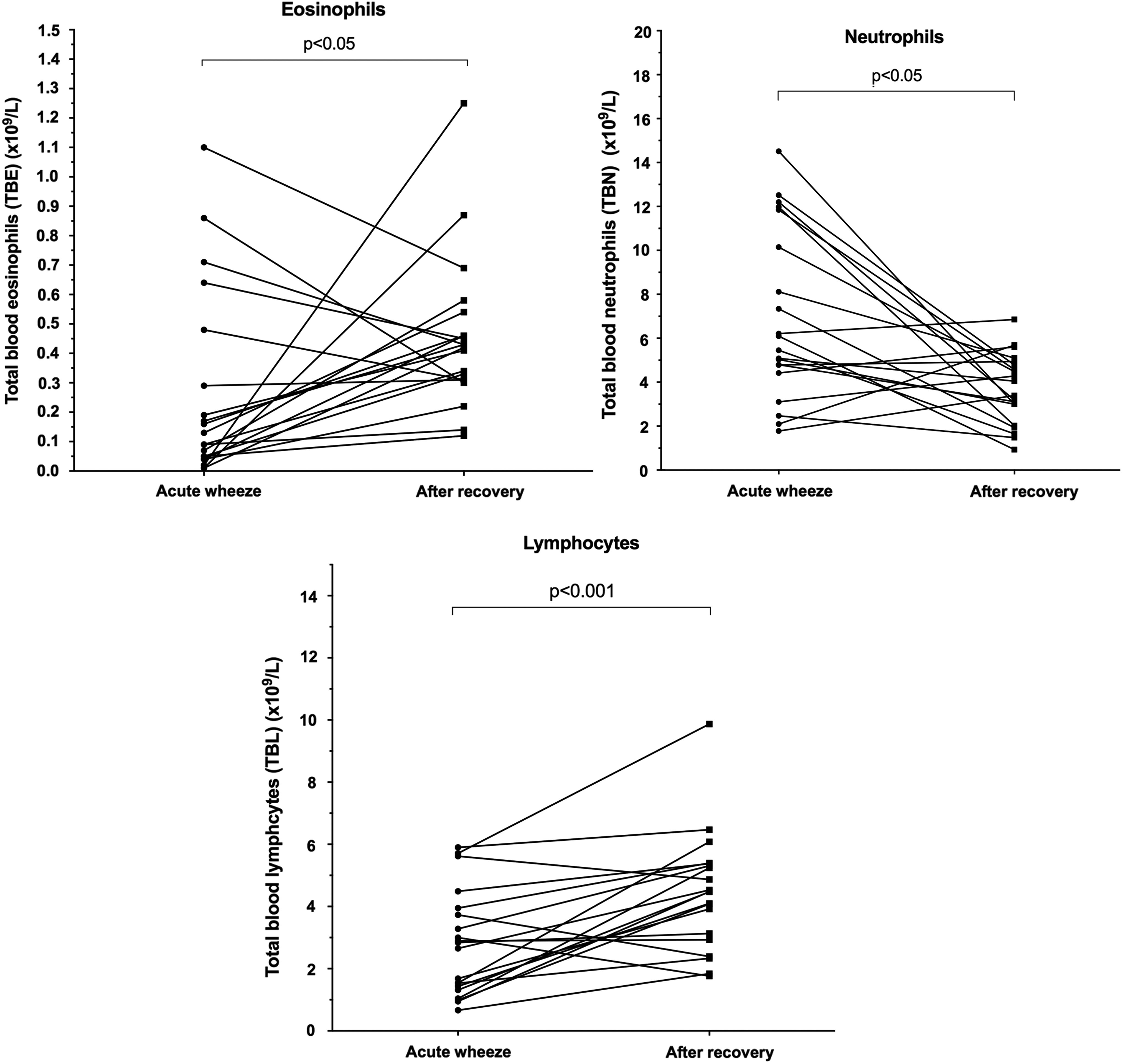
Absolute blood leukocyte counts during acute wheeze and following recovery for 20 children.
Data displayed as median (range).
TBE, total blood eosinophils; TBL, total blood lymphocytes; TBN, total blood neutrophils.
Blood eosinophil numbers and near-future exacerbations
Follow-up data on subsequent exacerbations were available for 35 children, which included the 20 who returned for a repeat blood sample. Follow-up data were not available in 33 children (4 had declined further contact at recruitment and 29 were not contactable for follow-up). The median follow-up time for these 35 children was 13 weeks (range 7–30 weeks). We found no significant association between blood eosinophil numbers measured during the acute exacerbation and subsequent episodes of parent-reported wheezing or unscheduled healthcare visits.
However, stable disease absolute blood eosinophil numbers were significantly associated with both, parent-reported near-future exacerbations and unscheduled healthcare visits (Fig. 4). Children with blood eosinophils ≥0.3 × 109/L during stable disease were significantly more likely to experience a near-future exacerbation compared to those with counts <0.3 × 109/L. Twelve of the 17 children (71%) with blood eosinophils ≥0.3 × 109/L had a subsequent exacerbation, whereas no child with counts <0.3 × 109/L experienced a wheezy episode (P < 0.05, chi-square).
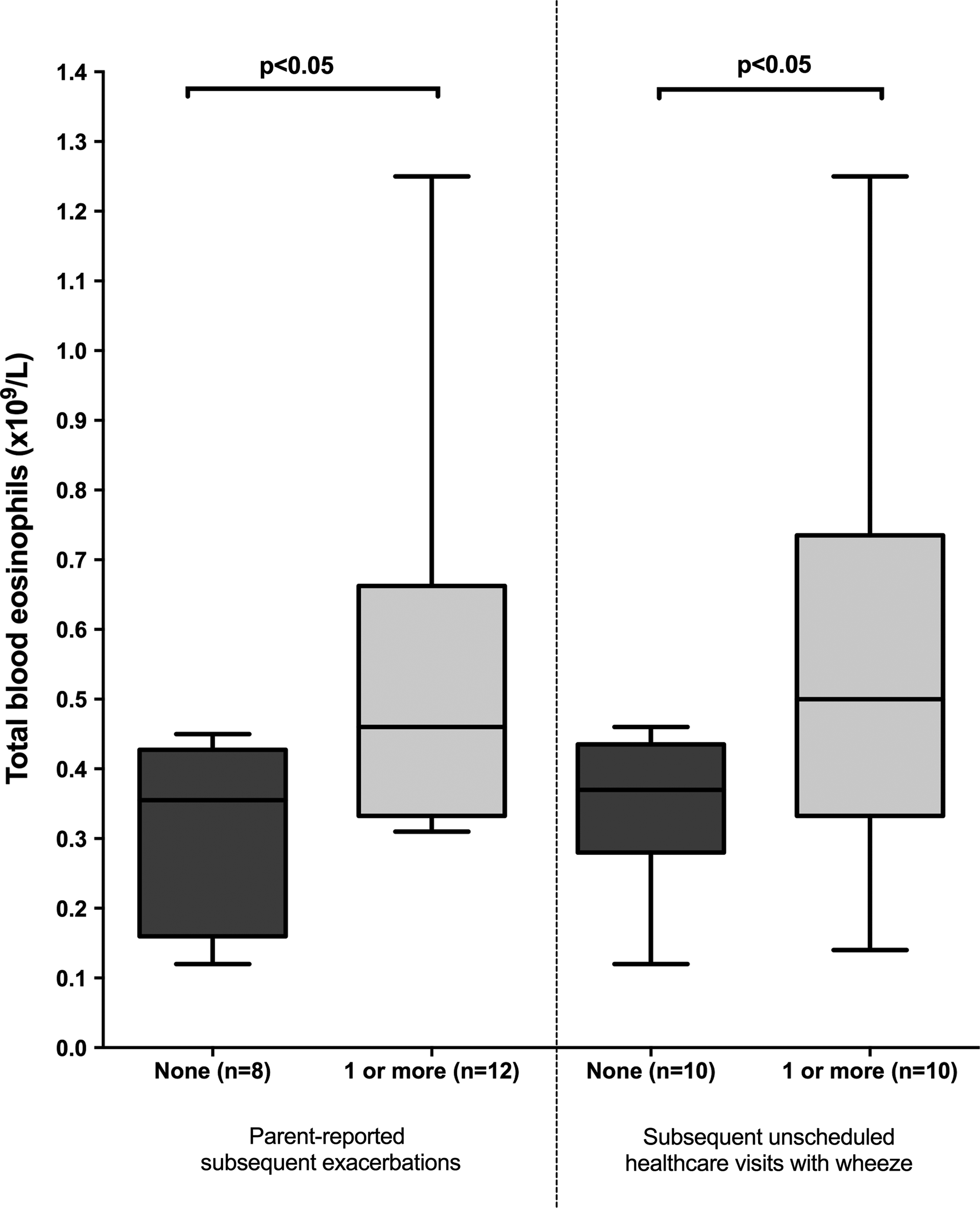
Stable blood eosinophil counts and near-future exacerbations.
Discussion
To our knowledge, this is the first study to systematically investigate whether numbers of blood eosinophils, and numbers of other blood leukocytes, differ between episodes of acute wheeze and periods of stable disease. The key finding of our study is that absolute blood leukocyte differential cell numbers are different during the time of an acute exacerbation compared with periods of stable disease in children with preschool wheeze. In particular, we found that blood eosinophil numbers were significantly higher during stable disease. This was also the case for blood lymphocytes. In contrast, blood neutrophil numbers were greater during an exacerbation. We found no difference in blood eosinophil numbers between acutely wheezy and control children. Interestingly, a study conducted in infants with bronchiolitis also reported greater blood eosinophil numbers after recovery from bronchiolitis. 16
Study strengths and limitations
Performing studies in young children that involve blood sampling are challenging by their very nature. During a patient and public involvement initiative before study initiation, approximately half the participating parents expressed a preference for a finger-prick blood sample rather than venepuncture, and this choice was incorporated into the ethics protocol. Despite this arrangement, obtaining follow-up blood samples when the children were clinically well was more difficult. It is perhaps not surprising that parents were reluctant to allow their children to undergo blood sampling at a time when they were well. Despite this limitation, a relatively large number of children with acute preschool wheeze were recruited and we obtained paired samples in 20 children. This allowed us to compare blood leukocyte differential cell numbers obtained during an exacerbation with those seen during stable disease. Our data are further strengthened by the relatively large control group recruited into this study.
The reasons for the difference in blood leukocyte differential cell numbers, particularly eosinophils, between exacerbation and stable disease are unclear. Using urinary markers, 1 previous study reported that eosinophil activation subsides after recovery from an acute exacerbation, 17 however, blood eosinophils were measured during the acute episode only in these children, limiting comparisons with our study.
We are aware that circulating blood eosinophils follow a circadian rhythm, with higher levels after midnight and in the early morning hours. 18 None of the children recruited in our study had blood samples taken during the night, and blood eosinophil counts in the majority of children studied were obtained between 0900 and 2100 h.
In older children and adults with allergic asthma, there is evidence of systemic eosinophilic inflammation, and blood eosinophils are recruited into the lung compartment. Eosinophil biology is largely under the influence of interleukin-5 (IL-5), released from primed pulmonary CD4+ T-helper 2 cells, a crucial mediator for eosinophil development, recruitment, and activation.19,20
A rise in eosinophil and neutrophil numbers in sputum during an asthma exacerbation has previously been reported in children.21,22 After recovery, sputum eosinophil and neutrophil numbers fall again. 21 Furthermore, in atopic individuals, there is evidence of a surge in the number of eosinophil–basophil colony-forming units during an acute exacerbation, which is orchestrated by IL-5, with numbers falling during recovery. 19 Activated eosinophils release an array of inflammatory mediators, including eosinophil cationic protein, eosinophil protein X, eosinophil peroxidase, and major basic protein, which are all capable of damaging respiratory epithelium with resultant airways hyperresponsiveness. 23
In preschoolers, studies investigating the cellular composition of bronchoalveolar lavage fluid have shown a mixed neutrophilic and eosinophilic inflammatory process.24–27 Furthermore, established eosinophilic airway inflammation has been demonstrated by means of endobronchial biopsy in preschool children with severe wheezing. 28 However, these studies involve children with severe disease justifying invasive clinical investigation and as such may not be representative of the majority of children with preschool wheeze.
Thus, our results combined with the preexisting knowledge that eosinophils are acutely activated during exacerbations of preschool wheeze, and knowledge of eosinophil biology during an exacerbation suggests that eosinophils are recruited into the lung compartment from the peripheral blood during an episode of acute wheezing. Further research is, however, required to test this hypothesis in the future.
Obtaining sputum in children with an exacerbation of preschool wheeze would be difficult. The induction of sputum, a less invasive method, has been demonstrated to be feasible in stable preschool children, 29 however, this technique would not be suitable for a child with an acute exacerbation.
Another interesting observation during our study was that a blood eosinophil count ≥0.3 × 109/L during stable disease predicted near-future acute exacerbations. Approximately 2 out of 3 children with this feature experienced at least 1 severe exacerbation within the next 7 months of the episode, during which they were recruited. No child with blood eosinophil counts <0.3 × 109/L during stable disease experienced an exacerbation during the follow-up period.
It is also of note that higher blood eosinophil counts were associated with an increased risk of exacerbations with all 8 children, with blood eosinophils during stable disease >0.45 × 109/L, experiencing an exacerbation in the follow-up period. It needs to be stressed that due to the relatively modest number of paired samples, these results need to be interpreted with caution.
The biomarker “blood eosinophils” has emerged as a potentially attractive candidate in preschool wheeze given its use as a marker of disease activity in asthma in older children and adults. Three large, recent epidemiological studies involving children aged 6 years and older and adults with asthma have shown that raised blood eosinophils are associated with exacerbation-prone asthma.9–11 Malinovschi et al. reviewed the laboratory markers of more than 12,000 individuals with asthma aged 6–80 years and found that peripheral blood eosinophils of more than 3% are independently associated with emergency healthcare visits for acute asthma. 10 This finding has been confirmed by a separate study reviewing data from 3,162 subjects with asthma from the National Health and Nutrition Examination Survey, an annual cross-sectional survey of the U.S. general population, where the authors found that the presence of absolute blood eosinophil numbers ≥0.3 × 109/L was associated with an increased frequency of acute asthma attacks in respondents, particularly in children. 9
In addition, a recently reported large pragmatic study conducted in primary care in the United Kingdom found that blood eosinophils >0.4 × 109/L, obtained during routine clinical reviews in over 100,000 patients aged 12–80 years with asthma, were associated with a significantly greater exacerbation frequency. 30
To date, there are no data of children with preschool wheeze relating blood eosinophils to near-future exacerbations.
We also found a significantly greater systemic neutrophilic inflammation during acute wheeze compared to recovery and stable disease. Sputum neutrophilic inflammation is a feature of asthma exacerbations. This is associated with elevated concentrations of neutrophil elastase in the airways.31–33 Neutrophils and their secreted inflammatory mediators, including neutrophil elastase, are thought to contribute to the pathobiology of acute asthma. Interestingly, asthma exacerbations triggered by respiratory viruses are associated with greater numbers of sputum neutrophils and increased concentrations of neutrophil elastase. 34 We know that the majority of episodes of acute wheeze in preschoolers are triggered by respiratory virus infection,35,36 and this may have contributed to the systemic neutrophilic inflammation that we observed. Numbers of blood neutrophils during an asthma exacerbation are, however, rarely reported, and to our knowledge, there are no published data comparing blood neutrophil numbers during acute exacerbation and following recovery in children with preschool wheeze. We did not, however, test the children in this study for the presence of respiratory viruses, and we were not able to study sputum.
Conclusions
Our study compared paired blood leukocyte differential cell numbers obtained from preschool children with acute exacerbations of wheeze and during disease stability when children were well. We found that blood eosinophil and lymphocyte numbers were significantly higher during stable disease. In contrast, systemic neutrophilic inflammation was observed during an exacerbation. This has not been reported before, and these findings, particularly with respect to blood eosinophils, have important implications when analyzing and designing studies using this biomarker in children with preschool wheeze.
Footnotes
Author Disclosure Statement
No competing financial interests exist.