
Abstract
Exercise-induced bronchoconstriction (EIB) is a key clinical problem for asthmatic children. Exercise challenge tests, used to confirm EIB, are time consuming and require patient cooperation. The aim of this study was to investigate the diagnostic values of fractional exhaled nitric oxide (FeNO), impulse oscillometry (IOS), and plethysmography for prediction of EIB in children with well-controlled asthma. Fifty-nine children with allergic asthma aged 6–18 years were included in the study. FeNO was measured and all patients underwent spirometry, IOS, and plethysmography. An exercise challenge test was performed to assess EIB. EIB was confirmed with an exercise challenge test in 20 (33.9%) patients. Baseline FeNO levels were significantly higher in the group with EIB (P = 0.003). Resistance at 5 Hz (R5) and frequency dependence of resistance (R5–R20) in IOS and total specific airway resistance (SRtot), residual volume (RV), and the ratio of RV to total lung capacity in plethysmography were significantly higher in the group with EIB. In the logistic regression analysis, the higher baseline FeNO, R5–R20, and SRtot values were found to be significantly related to EIB [Odds ratios (OR):1.35 and P = 0.046, OR:1.80, and P = 0.016, and OR:1.10, P = 0.035, respectively]. To differentiate asthmatic children with EIB from those without EIB, the optimal cutoff point for FeNO was 28 ppb [negative predictive value (NPV):86% and positive predictive value (PPV):52%]. An SRtot level lower than 207.6% (NPV:96% and PPV:54%) can be used to exclude EIB. R5–R20 values higher than 15.5% (NPV: 81% and PPV:71%) were associated with EIB in asthmatic children. Baseline SRtot in plethysmography provided the best sensitivity, whereas the baseline R5–R20 in IOS offered the best specificity for EIB. This study suggested that FeNO, IOS, and plethysmography are valuable tools for the assessment of EIB in children with controlled asthma and EIB is strongly correlated to small airway disease markers.
Introduction
E
Airway inflammation is associated with airflow limitation and AHR. The assessment of the association between airway inflammation and EIB is useful for the management of asthma. 2 Measurement of fractional exhaled nitric oxide (FeNO) is a non-invasive marker of eosinophilic airway inflammation. Previous studies have reported a significant relationship between increased FeNO levels and EIB in asthmatics.3–5
Impulse oscillometry (IOS) is a lung function test that evaluates airway limitation during tidal breathing and can be easily applied to even young children, as it only requires passive cooperation. 6 IOS is reported to be a more sensitive technique than spirometry for detecting subtle changes in lung function.7,8 It can be used for clinical diagnostic testing of patients with airway obstruction and AHR. 9
Total specific airway resistance (SRtot), measured by plethysmography, provides more sensitive measurements of airway obstruction. It was introduced as an alternative technique to assess lung function in asthmatic children. 10 It is noninvasive, easy to perform and can also be used for detecting AHR. 11
The aim of this study was to investigate the diagnostic value of IOS and plethysmography for the prediction of EIB in children with well-controlled asthma.
Methods and Materials
Study population
This study was conducted at the Pediatric Allergy and Immunology Department, Mersin University Hospital, Turkey, between January 2016 and June 2016. Children with allergic asthma aged 6–18 years were enrolled. The patients had intermittent and mild-to-moderate, persistent asthma and were all sensitized to house dust mites. They had well-controlled asthma that was defined as the absence of daytime symptoms, nocturnal symptoms, limitation of activities, and need for rescue treatment in the previous month with normal lung function [forced expiratory volume in 1 s (FEV1) % ≥80 predicted and ratio of FEV1 to forced vital capacity (FVC) (FEV1/FVC) ≥80% by spirometry]. 12 Regular medications were recorded for all patients. Children who had suffered from a respiratory tract infection in the previous 2 weeks, asthma attack, and a history of systemic steroid usage in the past month and who were not cooperative during lung function testing were excluded from the study.
The study was approved by the Institutional Ethical Committee, Mersin University, and all patients supplied written, informed consent before taking part in the study.
Study protocol
FeNO levels were first measured, and lung function was then evaluated by using IOS, spirometry, and plethysmography before exercise. AHR was assessed by a spirometric exercise challenge test after basal respiratory functions were evaluated.
FeNO measurement
FeNO measurement was performed with an NIOX MINO® (Aerocrine AB, Sweden) system according to the American Thoracic Society's (ATS) guidelines before performing spirometry, because forced expiration can decrease FeNO. 13 The children waited for 1 h in the same room where the measurement took place to prevent exposure to extrinsic factors. Participants were instructed to exhale to residual volume (RV). A mouthpiece was then inserted and they were asked to inhale to total lung capacity (TLC) and then to exhale for 10 s at a constant flow rate of 50 mL/sn.
Pulmonary function tests
Spirometry
Spirometry was performed by using a Master Screen spirometry system (JaegerCO, Germany) according to ATS guidelines. 14 The values of FEV1, FEV1 change in percent predicted (FEV1%chg), FVC, the ratio FEV1/FVC, and maximum mid-expiratory flow [MMEF; also known as forced expiratory flow rate (FEF25–75) measured between expired volumes of 25% and 75% of the vital capacity during a forced expiration] were recorded. 15 Bronchodilator response was evaluated by the percent change in FEV1 after 200 mcg of inhaled salbutamol with a metered dose inhaler. Zapletal reference values were used for spirometric indices. 16
Impulse oscillometry
IOS during tidal breathing was performed in compliance with the European Respiratory Society/ATS (ERS/ATS) guidelines 17 by using the MasterScreen system (JaegerCO, Germany). The IOS parameters obtained at the end of the application were resistances at 5–20 Hz (R5, R20), reactance at 5 Hz (X5), area of reactance (AX), and R5–R20 (resistance at 5 Hz minus resistance at 20 Hz). The difference between the absolute values obtained before and after salbutamol inhalation (Δ) was divided by the absolute values before salbutamol, and the result was multiplied by 100. Commercially available predicted values for IOS parameters were based primarily on height according to normal reference values as recommended by the manufacturer.
Plethysmography
Static lung volumes and airway resistance were assessed by whole-body plethysmography according to ATS guidelines. 18 Total specific airway resistance (SRtot), TLC, RV, and the ratio of RV to TLC were recorded and the results were expressed as a percent predicted for age, sex, and height. The reference equations for plethysmography were based on normal reference values as recommended by the manufacturer.
Exercise challenge
Subjects performed an exercise challenge test. In brief, first a basal FEV1 was obtained. Then, they rode a bicycle ergometer (cycle ergometer, 928G3 Monark Exercise AB, Sweden) for 4–6 min until they reached a heart rate of between 80% and 90% of the maximum predicted (220—age in years) in a temperature and humidity controlled environment according to ATS recommendations. 19 Spirometry was repeated 5, 10, 15, 20, and 30 min post-exercise. EIB was defined as a fall in FEV1 of at least 10%.
Statistical analysis
Descriptive analysis was performed by using median (25–75p) values for variables not normally distributed and means ± standard deviations for normally distributed variables. Independent-sample t-tests or Mann-Whitney U tests were used for a comparison of the 2 groups based on the distribution pattern of the variables. The chi-square test was used for categorical endpoints. Logistic regression analysis was used to evaluate associated factors for EIB. For variables with large measurement units, a regression coefficient was calculated by multiplying by 10 to examine the increase in risk when there was a change of 10 units instead of 1 unit. 20 Odds ratios (ORs) with 95% confidence intervals were estimated. Receiver operator characteristic (ROC) curve analysis was performed to determine the cut-off value for FeNO and pulmonary indices to predict EIB. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were analyzed. A P value of less than 0.05 was considered statistically significant.
Results
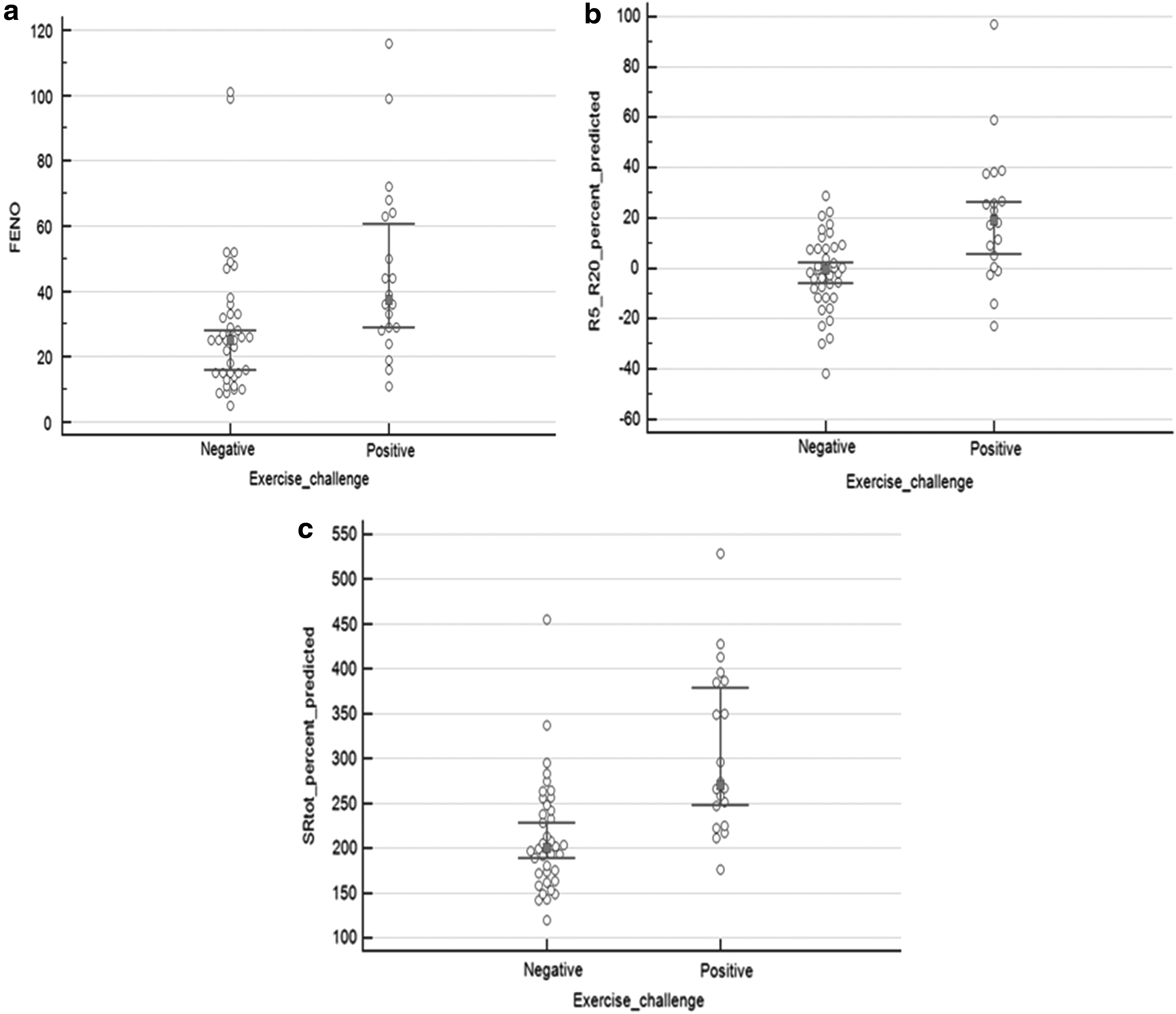
A total of 59 children aged 6–18 years participated in the study. The median age was 11.0 (9.0–14.0). Thirty-nine (66.1%) of the patients were male. Forty (67.8%) of the patients were using inhaled corticosteroids (ICS). EIB was confirmed with exercise challenge in 20 (33.9%) patients. There was no significant difference between patients with and without EIB in terms of age, gender, body mass index (BMI), ICS usage, serum eosinophil count, and serum IgE levels. However, FeNO levels were significantly higher in the group with the positive exercise challenge test (P = 0.003) (Table 1 and Fig. 1a). The clinical and demographic characteristics of the patients are shown in Table 1.
BMI, body mass index; FeNO, fractional exhaled nitric oxide; ICS, inhaled corticosteroids.
P values in bold are statistically significant.
Comparison of pulmonary function tests for patients with negative and positive exercise challenge test
The values of FEV1% predicted (P = 0.006), FEV1/FVC% predicted (P < 0.001), and MMEF% predicted (P < 0.001) were significantly lower in the group with positive exercise challenge than those with negative exercise challenge (Table 2). FEV1%chg predicted (P = 0.010), resistance at 5 Hz (R5% predicted) (P = 0.003), resistance at 5 Hz minus resistance at 20 Hz (R5–R20% predicted) (P < 0.001) (Fig. 1b), total specific airway resistance (SRtot% predicted) (P < 0.001) (Fig. 1c), RV% (predicted) (P = 0.044), and the ratio of RV/TLC% (predicted) (P = 0.049) levels were significantly higher in children with EIB than those without EIB (Table 2). No significant difference was found between the groups in terms of FVC% predicted (P = 0.017), ΔR5% predicted (P = 0.603), resistance at 20 Hz (R20% predicted) (P = 0.321), reactance at 5 Hz (X5) (P = 0.575), area of reactance (AX) (P = 0.206), ΔAX (P = 0.987), and TLC% (predicted) (P = 0.493) levels.
The values were presented as mean ± standard deviation. The other values were presented as median (25–75p).
FEV, forced expiratory volume; FVC, forced vital capacity; TLC, total lung capacity; MMEF, maximum mid-expiratory flow.
P values in bold are statistically significant.
Logistic regression and ROC curve of factors that are related to positive exercise challenge test
Higher FeNO, R5–R20% predicted, and SRtot% predicted values were found to be significantly related to EIB in the logistic regression analysis (aOR:1.35, P = 0.046, aOR:1.80, P = 0.016, and aOR:1.10, P = 0.035, respectively) independent of age, sex, BMI, ICS usage, and serum eosinophil count (Table 3). Each 10% increase in FeNO, SRtot, and R5–R20 predicts a 1.35-, 1.10-, and 1.80-fold increase in the risk of EIB, respectively.
P values in bold are statistically significant.
In the ROC curve analysis, FeNO levels lower than 28 ppb were found to be significantly related to the absence of EIB (AUC: 0.737, P < 0.001, sensitivity: 75%, specificity: 66.7%, NPV: 86%, and PPV:%52%) in children with controlled asthma (Fig. 2a). Twenty-four of the 28 children with FeNO levels lower than 28 ppb had no EIB, indicating an NPV of 86%.

An SRtot level lower than 207.6% was found to be significantly related to the absence of EIB (AUC: 0.828, P < 0.001, sensitivity: 95%, specificity: 61.5%, NPV: 96%, and PPV: 54%) in children with controlled asthma (Fig. 2b). Twenty-three of the 24 children with SRtot levels lower than 207.6% had no EIB, indicating a high sensitivity and NPV of 95% and 96%, respectively.
An R5–R20 level higher than 15.5% was found to be significantly related to the risk of EIB (AUC: 0.786, P < 0.001, sensitivity: 60%, specificity: 89.7%, NPV: 81% and PPV: 71%) in children with controlled asthma (Fig. 2c). Twelve of the 17 children with R5–R20 levels higher than 15.5% had EIB, indicating a specificity and PPV of 89.7% and 71%, respectively.
Discussion
EIB is a common feature of asthma but can also occur without asthma. The assessment of EIB is used for both the diagnosis and follow-up of asthma.21,22 However, exercise challenge tests take a long time and require special equipment such as a treadmill or bicycle ergometer and a temperature and humidity controlled environment that are not easily available. Thus, a reliable and more practical screening test would be a feasible tool for the prediction of EIB in children.
In this study, EIB was confirmed in 20 (33.9%) patients despite the fact that they had well-controlled asthma and 65% of them were using ICSs. R5% and R5–R20% levels in IOS, SRtot%, RV%, and RV/TLC% levels in plethysmography, and FeNO values were significantly higher in asthmatic children with positive exercise challenge. In the logistic regression analysis, the higher FeNO, R5–R20% predicted, and SRtot% predicted values were found to be significantly related to EIB. SRtot levels lower than 207.6% helped to exclude EIB with a high NPV of 96%. It was also possible to rule out the presence of EIB with FeNO values lower than 28 ppb and R5–R20 levels lower than 15.5% with high reliability (NPV 86% and 81%, respectively). On the other hand, an R5–R20 level higher than 15.5% helped to predict EIB with a specificity of 89.7% and a PPV of 71%.
The exercise challenge test is an indirect bronchial provocation test considered to be correlated better with clinical asthma than direct challenge tests.21,23 Because of its greater relation to airway inflammation and greater responsiveness to anti-inflammatory treatments, the indirect challenge could be the challenges of choice as a guide for evaluating and monitoring asthma. 21 Therefore, markers of airway inflammation can be useful for predicting EIB.2,24
FeNO, a non-invasive marker of eosinophilic airway inflammation, has become a reliable tool for the management of asthma in children.25,26 It has been demonstrated that airway inflammation and AHR persists in most patients with well-controlled asthma despite the fact that their condition is controlled.27,28 In this study, although all the patients had controlled asthma, 33.9% had a positive exercise provocation test. In this regard, FeNO is of particular value as a marker to predict AHR in children with well-controlled asthma.5,26 We found that FeNO levels were significantly higher in asthmatic children with EIB than without, which indicated the contribution of eosinophilic inflammation to EIB. Previous studies have investigated the predictive value of FeNO for diagnosing EIB.24,29,30 Lex et al. showed that no child in their study with normal pre-exercise FeNO (<25 ppb) had an abnormal exercise challenge result. 4 In this study, an FeNO level lower than 28 ppb was found to be reliable for ruling out the presence of EIB, with an NPV of 86% among asthmatic children who otherwise had a controlled disease.
Plethysmography is one of the most commonly used methods for measuring airway resistance in asthmatic children. 31 It was introduced as an alternative technique to assess lung function because it is easy to perform and non-invasive. Also, there is good evidence that body plethysmography has higher sensitivity than spirometry for detecting AHR.32,33 The comparison of spirometry and plethysmography during bronchial challenges showed that up to 20% of subjects demonstrated a positive response for specific airway resistance (sRaw) without sufficient response in FEV1. 33 SRtot, which is an effort-independent parameter measured by a plethysmograph, is a very sensitive index for diagnosis of peripheral airway obstruction.31,33,34 We found that SRtot levels were significantly higher in asthmatic children with EIB than without, and this suggested the involvement of peripheral airway obstruction in EIB. In addition, SRtot levels lower than 207.6% helped to exclude EIB with a high sensitivity of 95% and NPV of 96%. In cases of SRtot levels less than 207.6%, exercise challenge tests are unnecessary in children with controlled asthma. Further, RV and RV/TLC, which reflect air trapping, were also higher in the group with EIB. Plethysmographic assessment of lung volumes provides a sensitive measure of air trapping and lung hyperinflation. RV and RV/TLC are important measures of small airway dysfunction and can be raised before the onset of abnormal spirometry in asthma.35–37
IOS is a simple and non-invasive technique that measures respiratory resistance and reactance at different oscillation frequencies during spontaneous tidal breathing. 9 R5–R20, a measure of frequency dependence of resistance, reflects resistance in small airways. 38 The association of AHR and small airway function is of great importance in asthmatic children. 39 In addition, small airway dysfunction is considered a prominent feature in clinical entities such as EIB. 40 In this regard, the increased sensitivity of IOS is promising for the assessment of AHR as well as for small airway function in asthmatics.11,39,41 Consistent with these data, we found that R5–R20 levels were significantly higher in asthmatic children with EIB than without, and this suggests the involvement of small airway dysfunction in EIB. In addition, R5–R20 levels lower than 15.5% can help to exclude EIB, with an NPV of 81%. On the other hand, 71% of the children with R5–R20 levels higher than 15.5% had EIB, indicating specificity and PPVs of 89.7% and 71%, respectively.
The major limitation of this study was its small sample size. The strength of this study was its demonstration of the association between FeNO, baseline SRtot and R5–R20, and EIB in children with controlled asthma. These surrogate tests are easy to perform and time efficient; therefore, they are of great utility for the assessment of EIB in asthmatic children. In addition, because the prevalence of EIB in our study population was consistent with previous publications,19,42–44 PPVs and NPVs of the surrogate tests (FeNO, IOS, and plethysmography) identified in this study can be applied to most children with controlled asthma.
Conclusions and Clinical Implications
In conclusion, baseline SRtot in plethysmography yielded greater sensitivity whereas baseline R5–R20 in IOS offered greater specificity in relation to EIB. In addition, this study suggested that FeNO, IOS, and plethysmography are valuable tools for the assessment of EIB in asthmatic children even when the disease is under control and EIB is strongly correlated to small airway disease markers.
Institution at Which the Work Was Performed
The work was performed at the Pediatric Allergy and Immunology Department of Mersin University, Faculty of Medicine.
Footnotes
Authors' Contribution
T.A. and A.U. recruited the subjects. T.A. wrote the first draft of the article. S.B.B. and S.K. took part in the critical revision of the article. S.K. designed the whole study, completed writing, and supervised the project. All authors agreed on the final version of the article.
Author Disclosure Statement
No competing financial interests exist.