
Abstract
A 17-year-old male presented with subacute onset of cough, fever, dyspnea, and weight loss. He had no unusual exposures, but had been taking minocycline for 6 months for acne. His initial chest X-ray revealed patchy bilateral airspace consolidations. He was treated with azithromycin and then amoxicillin/clavulanate, but due to lack of improvement, he was prescribed ciprofloxacin and had a chest computed tomography (CT) that revealed bilateral multifocal consolidations with a predominant peripheral and subpleural distribution. He was then referred to pulmonology. Laboratory studies were significant for 8.0% eosinophilia and negative infectious workup. Initial plethysmography revealed a restrictive pattern (FEV1 55%, forced vital capacity [FVC] 48%, total lung capacity [TLC] 70%, residual volume [RV] 141%). Flexible bronchoscopy revealed normal anatomy and increased secretions at the right lower lobe. Bronchoalveolar lavage was significant for severe inflammation and elevated eosinophils of 22%. At this time, he already self-discontinued minocycline and was prescribed prednisone 20 mg twice a day (0.57 mg/kg per day) with rapid improvement in cough and dyspnea. He required about 5 months of slowly tapering steroids with a post-treatment chest CT revealing resolution of the multiple peripheral consolidations, and pulmonary function tests (PFTs) had normalized.
Introduction
E
Owing to the rarity of these diseases, nonspecific symptoms, and inconsistent peripheral eosinophilia, the diagnosis of EP may be delayed. Often, it is a combination of exposure history, characteristic computed tomography (CT) findings, BALF eosinophilia, and improvement after discontinuing the offending medication and/or response to steroids that led to the diagnosis of CEP.
We present a case of a 17-year-old male with acne who was taking minocycline and subsequently developed drug-induced eosinophilic pneumonia.
Case Report
A 17-year-old male with acne, environmental allergies, and a history of melanocytic nevus and spondylosis presented to pulmonary specialists with 1 month of cough, fever, headaches, dyspnea, fatigue, and weight loss (−3% total weight loss). There was no significant exposure or travel history. Initially he had been diagnosed with a left upper lobe pneumonia and was prescribed azithromycin by his primary physician, but due to persistence of symptoms, he was subsequently prescribed amoxicillin–clavulanate and had a repeat chest radiograph that showed bilateral peripheral upper lobe, posterior right lower lobe, and possibly superior bilateral lower lobe airspace consolidations consistent with nonspecific multifocal pneumonia (Fig. 1).

AP chest radiograph showing bilateral, nonsegmental, and relatively symmetric consolidations, with a predominantly peripheral and upper lobe distribution (arrows).
A few days after starting amoxicillin–clavulanate, he was brought to the emergency department after his dyspnea worsened and he developed chest pain. He was found to have low-grade fever and mild tachypnea without other respiratory physical examination findings. Chest radiograph showed slightly increased interstitial opacities thought to be consistent with atypical pneumonia. Laboratory findings (Table 1) were significant for absolute eosinophil count 0.5, absolute lymphocytes 1.7, ESR 47, CRP 5.1, and CO2 30.
CBC, complete blood count; CRP, C-reactive protein; CMP, comprehensive metabolic panel; ESR, erythrocyte sedimentation rate.
He was prescribed albuterol inhaler. Saturations were >95% at all outpatient and emergency department encounters. Owing to worsening symptoms and elevated ESR and CRP, he was referred to infectious diseases who recommended starting ciprofloxacin 500 mg twice a day for 10 days, infectious disease serologies (Table 2), antinuclear antibodies (ANA), repeat complete blood count (CBC) that showed eosinophilia of 0.8 with mild neutrophilia, and chest CT with contrast, which was performed ∼3 weeks after initial presentation. Chest CT showed “predominantly peripheral and subpleural multifocal consolidations involving both the lungs, largest measuring 9.5 × 1.3 cm within the lateral right upper lobe subpleural region.” (Fig. 2)
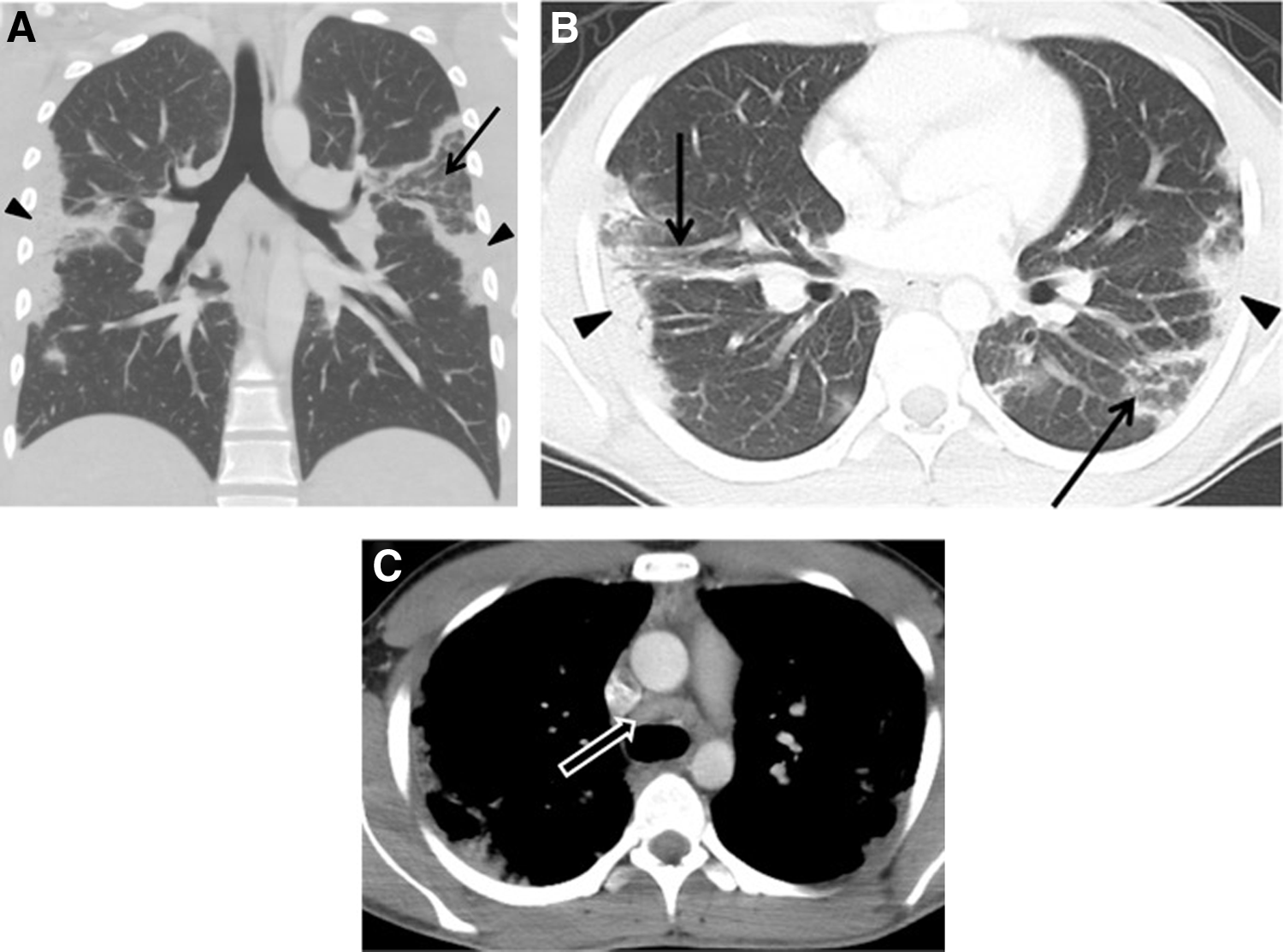
Coronal
BALF, bronchoalveolar fluid; PCR, polymerase chain reaction.
Owing to positive ANA and consideration of minocycline-induced lupus variant, he was referred to rheumatology. Further rheumatologic workup was overall negative and results are shown in Table 2.
With an abnormal chest CT and continued symptoms, he was referred to pulmonology. The patient had self-discontinued minocycline 2 days before his first visit. Initial plethysmography revealed total lung capacity (TLC) 70% predicted, residual volume (RV) 141%, FEV1 55%, forced vital capacity (FVC) 48%, and no bronchodilator response. Diffusing capacity of the lung for carbon monoxide (DLCO) was 78% (99% after correction for alveolar volume). Owing to suspicion of eosinophilic pneumonia based on laboratory and chest CT findings, bronchoscopy was performed, which revealed normal anatomy and opaque bubbly secretions in the right lower lobe. BALF had 22% eosinophils, 44% neutrophils, 12% macrophages, 22% lymphocytes, and cytology showed acute inflammation with frequent eosinophils identified. Significant laboratory results included BAL bacterial culture with normal flora, negative AFB and silver stains, and negative acid fast bacilli (AFB) fungal cultures. Repeat CBC revealed absolute eosinophilia to be 0.7 TH/uL.
Considering his clinical course, peripheral eosinophilia, and BAL eosinophilia, he was diagnosed with CEP, likely minocycline induced. Prednisone 20 mg BID (weight 67.5 kg = 0.59 mg/kg per day) was initiated and he felt improved energy within a week, although his acne worsened. Follow-up after 3 weeks of prednisone showed improved FEV1 to 86% and FVC to 74%. FeNO was 13 ppb. Owing to clinical and pulmonary function test (PFT) improvement, the steroids were tapered to 10 mg for 2 weeks (20 mg daily for 1 week, then 10 mg daily for 5 days) but he developed muscle aches, chills, and lethargy after weaning to 10 mg daily. Steroids were then increased to 20 mg BID for 3 days with improvement in fatigue and aches. He then completed a slower steroid taper of 10 mg BID × 1 week, 10 mg daily × 4 weeks (prolonged course due to increased fatigue and aches when he was tapered to 5 mg daily), then prednisone dose decreased by 1 mg every 1–2 weeks as tolerated. Approximately 14 weeks after steroid initiation, his repeat FEV1 was 90%, and FVC was 78%. Repeat chest CT with contrast showed “interval resolution of the multiple peripheral consolidations, borderline bronchiectasis, with central bronchi about the same size as adjacent pulmonary arteries” (Fig. 3). Repeat CBC was normal with 0% eosinophils and ANA decreased from 1:640 to 1:160. He was advised to avoid all tetracyclines in the future.
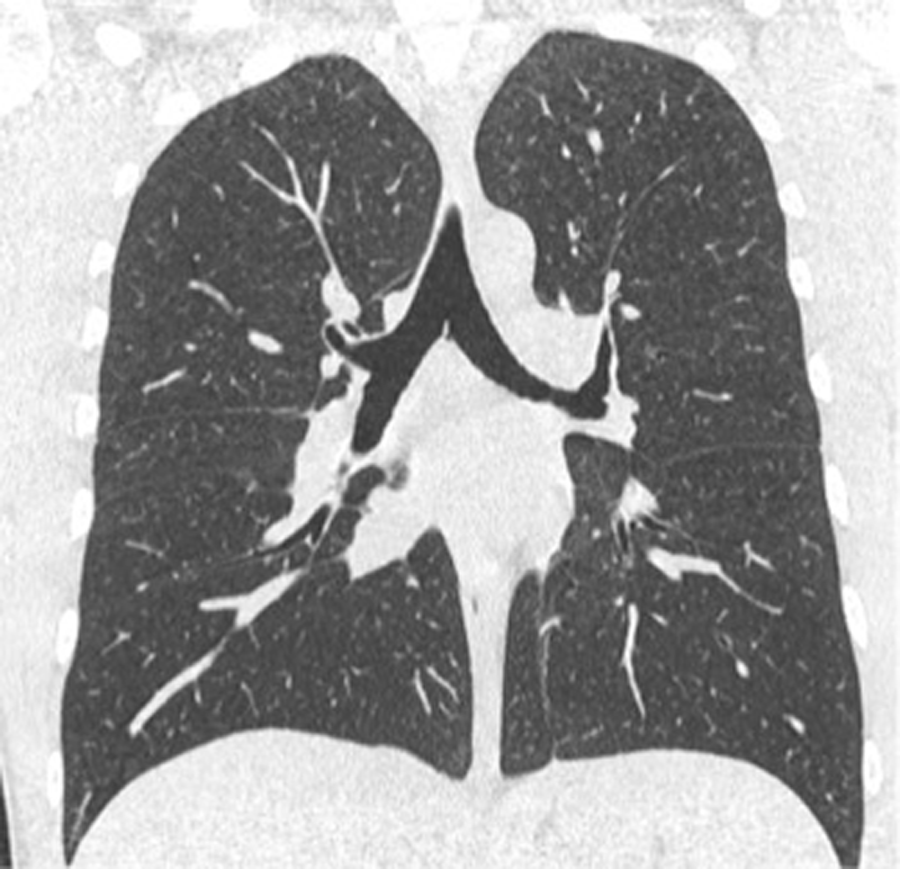
Coronal and axial images (without contrast) showing a normal chest CT after resolution of symptoms. CT, computed tomography.
Discussion
Drug-induced eosinophilic pneumonia has been mainly described with NSAIDs and antibiotics, including minocycline.6,7 To our knowledge, this is the first study documenting minocycline-induced eosinophilic pneumonia in a pediatric patient. In addition, our patient is a young male without history of asthma, unlike the typical demographics of eosinophilic pneumonia.
Eosinophilic pneumonias are a rare group of diseases in the pediatric population. CEP is more common in women in their mid-40s and half have a history of asthma. Less than 6% of patients with CEP are <20 years old.8,9 Duration of symptoms range from transient to chronic and outcomes include total resolution of symptoms without relapse to rare cases of life-threatening situations, requiring mechanical ventilation.10–12 Clinical findings include dyspnea, cough, fever, night sweats, and weight loss. Patients often have peripheral eosinophilia and/or BALF eosinophilia. Chest radiograph and chest CT reveal peripheral parenchymal infiltrates that are usually bilateral but can be unilateral, often in a photographic negative pattern of pulmonary edema known as “reverse pulmonary edema.” Uncommonly, pleural effusions may be present. 13 PFTs can be obstructive, normal, or restrictive. 14 Although our patient's FeNO was normal, Park et al. described a positive correlation between FeNO and peripheral eosinophilia in patients with CEP. 15 The mainstay of drug-induced eosinophilic pneumonia treatment is withdrawal of the offending agent and systemic corticosteroids. Reintroduction of the offending agent may cause a resurgence in pulmonary symptoms. 16 No consensus exists on steroid dosing although typical regimens include starting prednisone between 0.5 and 1 mg/kg per day (range of 0.3–3 mg/kg) for a total course of weeks to several months. 17 Blood eosinophilia and chest X-ray often normalize within 1 week and symptoms improve soon after starting steroids. 18
In addition to drug-induced eosinophilic pneumonia, parasitic infections can also be a cause of CEP. A careful travel and exposure history is important and testing for ova and parasites in BALF or stool should be included in the workup. Alternative options for relapse therapy include anti-IgE treatment with omalizumab (for patients with elevated IgE 19 ) and low-dose cyclosporine.20,21 Omalizumab has been suggested to induce apoptosis of peripheral eosionophils.22–24
Significant differences exist between adult CEP and pediatric CEP. Although adult CEP usually involves higher BAL eosinophilia (>40%), a pediatric series found median BAL eosinophilia of 28% (20%–44%), suggesting that a lower threshold may be more appropriate for pediatric diagnoses. Adults tend to require a longer total course of therapy (∼14 months) than children (4–6 months). Relapse is more common in adults, although this may be influenced by the low prevalence of CEP in children. Adult studies have shown that asthma is a common development after CEP. One follow-up study found that only 11% of pediatric patients with CEP developed asthma and 13% had persistent obstructive pattern without bronchodilator response.1,8
Conclusion
Eosinophilic pneumonia should be considered in patients with respiratory symptoms not responsive to typical medical interventions. CEP can be induced by certain medications, so a thorough history is crucial. Although chest CT, flexible bronchoscopy, and BAL are not routinely indicated for patients with respiratory symptoms, they should be considered in the patient with chronic symptoms who continue to be ill despite more common medical therapies. Although criteria exist for the diagnosis of AEP and CEP in adults, a standard set of criteria for pediatric EP does not currently exist. Establishing diagnostic criteria and guidelines for CEP would be useful in determining differential diagnoses and therapy, both for acute and chronic management.
Footnotes
Author Disclosure Statement
No competing financial interests exist.