
Abstract
Background:
Most studies on the effects of environmental factors on exercise-induced bronchoconstriction (EIB) in children have been carried out under indoor conditions. The purpose of this study was to compare the occurrence of EIB in cold and warm seasons in school children under natural exposure to climatic conditions at school.
Methods:
A total of 213 nonasthmatic schoolchildren, aged 15 17 years, were studied. Collection of spirometry data was performed in winter and summer during two years before and immediately after administration of the YO-YO intermittent test. The diagnosis of EIB was defined as a first-second forced expiratory volume (FEV1) decrease from a baseline of 10% or more with exercise. Daily air temperature and humidity data were recorded during the same periods.
Results:
The occurrence of EIB differed according to the season (In 2015, 51.2% in winter and 19.7% in summer, P < 0.001. In 2016, 36.8% in winter and 14.6% in summer, P < 0.001). In school children who participated in both years, 39.58% (57 of 144) had EIB in at least one winter. In 2015, 19% of participants reported exercise-induced symptoms in the winter season but only 1.4% reported symptoms in summer. In 2016, there were no reported respiratory symptoms. EIB is significantly correlated with air temperature and humidity (In 2015: r = −0.640 and r = −0.694, respectively; P < 0.01; In 2016: r = −0.461, P < 0.01 and r = −0.667, P < 0.01).
Conclusion:
Our study shows that seasonal variability affects the occurrence of EIB in healthy school children. The occurrence of EIB is associated with environmental temperatures and humidity.
Introduction
A
The study was carried out on healthy Tunisian school children engaged in common school-sport conditions and following a form of exercise challenge test, the Yo-Yo intermittent recovery test level 1 (Yo-Yo IRTL1), 13 combined with spirometry.
Materials and Methods
Study population
Two hundred thirty teenagers enrolled at Borj Louzir High School, Ariana, Tunisia, were screened to be included in the study. Seventeen were excluded: five had asthma, two were using a medical treatment that can interfere with the assessment of the pulmonary function, six were active smokers, and four performed high-level sports activities. Two hundred thirteen school children (sex ratio = 1.01; age: 16.2 ± 0.7 years; body mass: 60.2 ± 10.0 kg; height: 169.6 ± 9.4 cm; BMI: 20.9 ± 3.0 kg/m2)were included in the first part of the study carried out in 2015. The second part of the study, carried out the following year, involved only schoolchildren who did not report symptoms during the first-year challenge tests.
The participants and their parents were fully informed of the aims and the protocol of the study and signed an informed consent form.
The research protocol was conducted in accordance with the Declaration of Helsinki and was approved by the local ethical committee of Abderrahman Mami University Hospital, Ariana, Tunisia.
Study design
Before the start of the study, the participants were familiarized with the Yo-Yo IRTL1 and spirometry tests. The anthropometric and spirometric measurements of all participants were performed by the same investigator. Symptoms reported by the participants during and/or after exercise were recorded by the supervising physician.
The study was carried out during cold (January) and warm (June) periods in 2015. During each period, spirometric measurements were taken before and after the Yo-Yo IRTL1 at multiple time points. The participants who presented with exercise-induced symptoms were referred to the pulmonology departments for consultation. To check the reccurrence of the variation of EIB during the different seasons, the participants who remained in the same school and did not report symptoms were invited to the next-year challenge tests for two seasons.
The test sessions were performed in the morning during the same hours (8:30 and 11:30 am) to avoid the effect of circadian rhythm on measured variables. 14 On the day of the test, participants with acute throat or nasal symptoms were rescheduled for a later date at least seven days after complete recovery.
During the testing days, data on weather conditions were obtained from the National Institute of Meteorology. The values of temperature and relative humidity (mean ± SD) are reported in Table 1.
Significant difference in comparisons between winter and summer data (P < 0.001).
RH, relative humidity; T, temperature.
Procedures
Spirometry
Spirometry was carried out using a portable spirometer equipped with a pneumotachograph and requiring no calibration (Spiro-usb™; Care Fusion UK 232 Ltd., Basingstoke, UK). This spirometer has an accuracy of ±3% (ATS recommendations-standardizations of Spirometry 1994 update for flows and volumes) with a resolution of 10 mL volume 0.03 L/s flow.
The participant was comfortably seated while wearing nose clips and was asked to take in a full breath, a maximum inspiration, and then a forced expiration as hard and as fast as possible (making sure the lips sealed the mouthpiece). At each time point, the participant performed the test three times. The best first-second forced expiratory volume (FEV1) value of the three measurements was recorded. 15 The result was expressed in liters. Tunisian reference values were used to calculate the percentage of spirometric parameters. 16
FEV1 was measured at rest, immediately after stopping the exercise, and then 5, 10, and 15 min later.
The participants were diagnosed with EIB if any of the post-exercise FEV1 values was at least 10% lower compared to the pre-exercise FEV1 measurement. This level of decrease was chosen according to the recommendations of the American Thoracic Society. 17
Each participant received a careful postexercise physical examination to record signs and symptoms such as cough and shortness of breath. Children who exhibited asthma symptoms during or after the exercise were treated with 400 mcg of inhaled salbutamol and were reexamined before they returned to class.
Exercise performance
Before the Yo-Yo test, all participants participated in a warm-up period consisting of five min of jogging. All testing sessions were performed outdoors on the high school field.
The Yo-Yo IRTL1 was conducted according to the method of Krustrup et al. 13
The test consisted of 20-m shuttle runs performed at progressively increased speed until exhaustion. Between each running bout, the participant had a 10-s active recovery period consisting of 2 × 5 m of jogging. The velocity was adjusted according to the audio cues of the Yo-Yo test recorded on a CD player with no obstructions. Participants were strongly encouraged verbally throughout the trial.
The first time a participant could not reach the front line in time, the student was given a warning. The second time that the student was unable to keep pace with the audio signals, the test was stopped.
The total distance covered during the Yo-Yo IRTL1, including the last incomplete shuttle, was considered as the test score. During the Yo-Yo test, the participant was equipped with portable heart rate monitor (Polar S610; Oy, Kempele, Finland) to record the heart rate (HR) at intervals of five s. Each participant was requested to run during the exercise challenge test without exceeding 85%–90% of the maximum estimated HR (HRmaxTheo = 220−age). 18
Statistical analysis
Statistical tests were processed using STATISTICA Software (StatSoft, France). For qualitative variables, the absolute frequency and percentage were determined. For quantitative variables, the central trend, position, and dispersion were estimated using the mean and standard deviationSD. Respiratory symptom results were expressed as numbers of findings and percentages of participants. Differences between the means of continuous variables were analyzed using Students t-test or analysis of variance. McNemar's test for paired data was used to compare the frequencies between seasons. The correlation between EIB and climatic factors (temperature and relative humidity) was assessed using Pearson's correlation coefficient (r). The level of statistical significance was set at P < 0.05. Confidence intervals were calculated at the 95% level.
Results
In 2015, all of the 213 participants completed the spirometric and the running test. Variable distributions were normal.
There were significant differences in temperature and relative humidity between winter and summer (Table 1).
The FEV1 value decreased significantly after exercise at all measurements (0, 5, 10, and 15 min after exercise) in both seasons (P < 0.01) (Fig. 1).
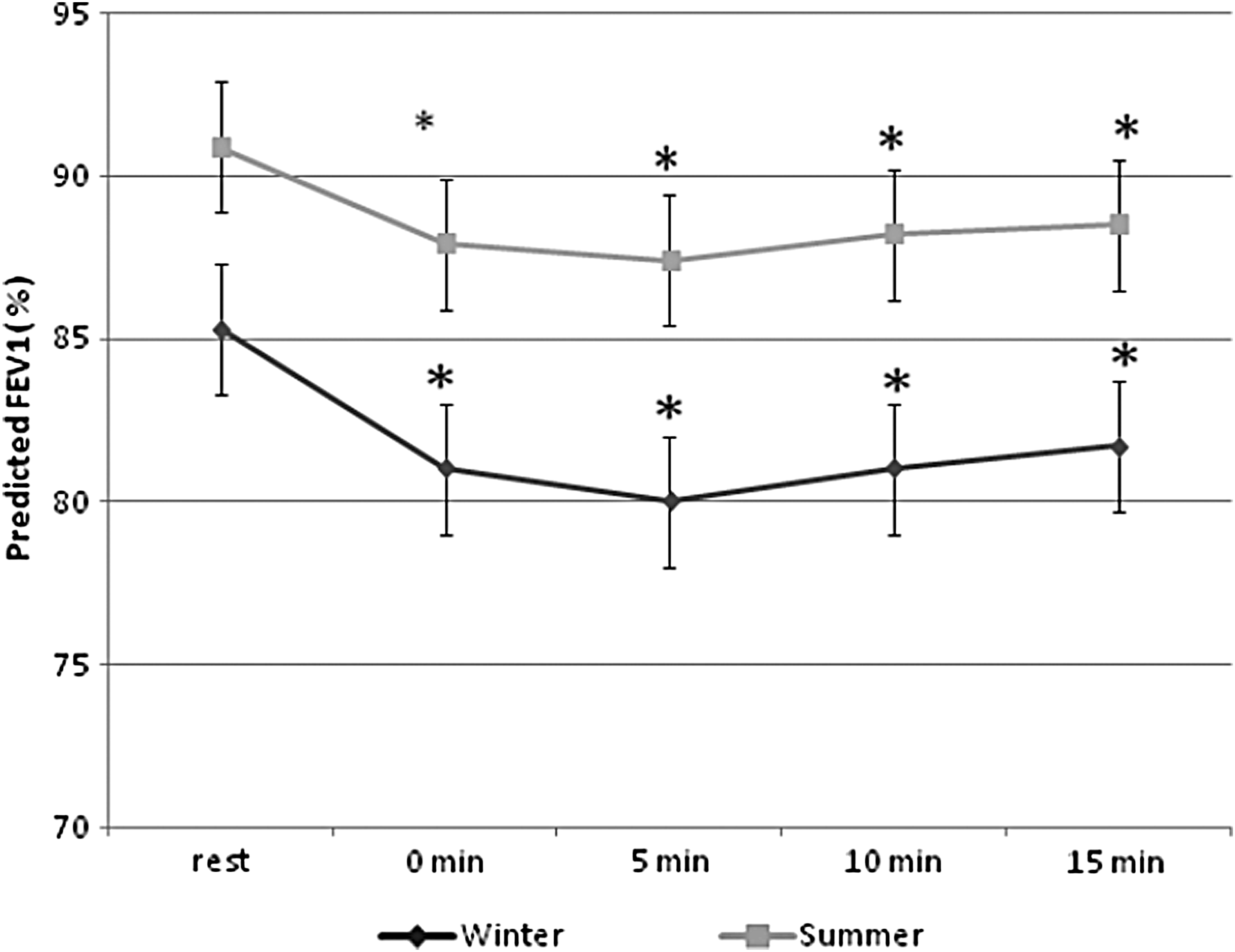
Predicted FEV1 (mean) before and after exercise in winter and summer periods. *Significant difference between FEV1 at rest and FEV1 post-exercise at all data points (P < 0.01). FEV1, first-second forced expiratory volume.
EIB was detected in 51.2% of participants (109 of 213) in winter and in 19.7% (42 of 213) in summer (P < 0.001) (Table 2). EIB was experienced similarly by both females and males (51.4% vs. 48.6% in winter, P = 0.367 and 50% vs. 50% in summer, P = 0.812, respectively).
Mean ± SD.
Number (%).
Significant difference in comparison between winter and summer data (P < 0.001 and P < 0.01, respectively).
EIB, exercise-induced bronchoconstriction; FEV1, 1st second forced expiratory volume; SD, standard deviation.
Among participants who had EIB in winter, 67.9% did not have a significant decrease in postexercise FEV1 in summer (P < 0.001). Among participants who had EIB in summer, 6.7% did not have a significant drop in FEV1 in winter (P < 0.001).
There was a correlation between EIB and air temperature (r = −0.640, P < 0.01) and humidity (r = −0.694, P < 0.01).
Forty participants (19%) presented with respiratory symptoms (cough: 60%, dyspnea: 22.5%, dyspnea and cough: 17.5%) during or after exercise in the winter season, but only three (1.4%) reported cough in summer (P = 0.032).
In 2016, 144 children (71 boys and 73 girls) participated in the study (age: 17.1 ± 0.7 years; body mass: 60.6 ± 11.1 kg; height: 169.6 ± 9.2 cm; BMI: 21 ± 3.43 mean ± SD). Forty participants who presented with exercise-induced symptoms in 2015 were excluded. The others (n = 29) changed institutions. The higher prevalence of EIB in winter compared with summer in 2015 was also noted in 2016. So, EIB was observed in 36.8% (53 of 144) of teenagers in winter and in 14.6% of teenagers (21 of 144) in summer (P < 0.001) (Table 3). EIB was experienced similarly by both females and males (50.9% vs. 49.1% in winter, P = 0.764 and 57.1% vs. 42.9% in summer, P = 0.522, respectively). Among children who had EIB in winter, 73.6% did not have a significant decrease in post-exercise FEV1 in summer (P < 0.001). Among participants who had EIB in summer, 4.9% did not have a significant drop in FEV1 in winter (P < 0.001). Similar to the first experimental period, EIB was significantly correlated with ambient temperature (r = −0.461, P < 0.01) and with relative humidity (r = −0.667, P < 0.01). None of the participants reported exercise-induced symptoms during both seasons.
Mean ± SD.
Participants who developed EIB (%).
Significant difference in comparison between winter and summer data (P < 0.001 and P < 0.05) respectively.
EIB, exercise-induced bronchoconstriction; FEV1, 1st second forced expiratory volume; SD, standard deviation.
In school children who participated in both years, 39.58% (57 of 144) had EIB in at least one winter. The prevalence of EIB was significantly higher in winter than in summer in school children who participated in both years (In 2015: 39.58% vs. 10.41%, P < 0.001; in 2016: 36.80% vs. 14.58%, P < 0.001).
The running test scores differed according to season (In 2015: 640 ± 366 m in winter and 660 ± 373 m in summer, P < 0.001; In 2016: 654 ± 386 m in winter and 685 ± 388 m in summer, P < 0.001).
No significant differences were observed in test scores between participants with and without EIB (Table 4). There was no significant difference in test scores between school children with exercise-induced symptoms (Symptom+) and without exercise-induced symptoms (Symptom−) [In winter: Symptom+: 582 ± 284 m, Symptom−: 653 ± 381 m (P = 0.264); in summer: Symptom+: 373 ± 161 m, Symptom−: 666 ± 374 m (P = 0.178)].
EIB(+), participants who developed exercise-induced bronchoconstriction.
EIB(−), participants with no observed exercise-induced bronchoconstriction.
Discussion
The results of our study showed that the prevalence of EIB was significantly higher in winter than in summer in school children who participated in both years (In 2015: 39.58% vs. 10.41%, P < 0.001; in 2016: 36.80% vs. 14.58%, P < 0.001). Low air temperature and low humidity were associated with EIB in school children.
The results of our study showed a high prevalence of EIB during the two seasons in 2015. The same results were noted in 2016 which showed the reccurrence of the above findings.
EIB is a phenomenon of transient airway narrowing that occurs during or after physical exertion and generally resolves spontaneously. 19 The etiology of EIB stems from breathing relatively dry and cold air during exercise which causes the airway to narrow by osmotic and thermal consequences of evaporative water loss from the airway surface.20,21 Dehydration of small airways stimulates the release of inflammatory mediators, such as histamine and cysteinyl leukotrienes, which lead to bronchial constriction. 22 Hence, a positive response to the exercise challenge test is believed to reflect active airway inflammation and bronchial hyperresponsiveness.23,24
The estimated prevalence of EIB was higher in our study population than in athletes and in the general Tunisian population.25–27 Many studies have been conducted to determine the prevalence of EIB in schoolchildren and adolescents, but there were marked differences among these studies probably because of methodological considerations. In studies conducted in outdoor conditions, the prevalence of EIB ranged from 9.2% to 19.2%.28–34 Lødrup et al. 35 reported an EIB prevalence of 8.6% when 616 children were exercise-tested in a laboratory setting. This wide variation between the studies is probably due to different types of training and training environments.
In our study, we did not find any gender differences in the estimated prevalence of EIB.
Similar results have been reported in other studies.23,25,29 In contrast, De Baets et al. 36 , as well as Busquets et al. 37 , reported a higher prevalence of EIB among girls (13% and 8.5%, respectively) than among boys (9% and 6.4%, respectively) with a statistically significant difference.
In the present study, we assessed EIB in natural climatic conditions at school. The assessment of EIB under outdoor conditions may explain the high prevalence of this disorder in our study compared with those reported in the literature. Environmental factors and, in particular, climate change could play an important role. In literature, few studies, usually focusing on the population of athletes,38–41 have evaluated the effect of climatic factors on EIB. To the best of our knowledge, the present study is the only one which assesses the effect of environmental factors on the occurrence of EIB among schoolchildren in Tunisia. It has been demonstrated that the mechanisms of EIB are related to significantly increased ventilation during exercise, which causes increased heat and water loss through respiration. Therefore cooling the airways is considered as one of the most important mechanisms in the occurrence of EIB. 42 Thus, the incidence of EIB is more detectable in winter athletes. Several studies conducted on asthmatic subjects and athletes have shown that pulmonary function and EIB were influenced by changes in temperature regardless of relative humidity.43–45 These studies confirmed that considerable hyperpnea at low temperatures causes a detectable airway obstruction. However, these findings do not correlate with Stelmach et al., who reported no significant association between air temperature and EIB in a population of school children. 28
In our research, we also observed that a predictor for the development of EIB was lower humidity. Similar findings have been reported in other studies.46–49 Thus, in these studies, humid air has been reported to reduce EIB. The reduced loss of water from the airways is probably the main reason for the protective effect on EIB in a humid environment.46,48,50 Bar-Or et al. 48 suggested that EIB is more likely to occur in dry air (25% relative humidity and about 25°C–26°C) than in humid air (90% relative humidity and 25°C–26°C), possibly due to heat loss at the airway mucosa caused by evaporation. Kallings et al. 50 also reported that cold, dry air provoked more bronchoconstriction than room-temperature humid air (60% relative humidity). In contrast, Zainudin et al. 51 reported no significant relationship between different humidity levels (41%–90% relative humidity) and EIB in Malaysian school children, 7–12 years. However, in other studies, the authors found that exposure to higher humidity increases the risk of bronchoconstriction.28,52
The findings of our research should be considered despite some limitations. In the present study, we evaluated the effect of environmental temperature and relative humidity on the EIB. However, variation in the EIB cannot be totally explained by such climatic conditions. Thus, allergen exposure, barometric pressure, and air pollution can also play an important role.25–27 In addition, exposure to allergens or contaminants in the inhaled air may have marked seasonal variation. 1 Viral respiratory infections, more frequent in winter, could also play an important role; viruses can have lingering effects for several weeks or longer. Perhaps some of the reactivity in winter could be explained by this. Second, our study population included only urban school children, and thus, our finding may not be applicable to those from rural areas.
Conclusion
Our study showed that EIB is common in school children, and its occurrence varies with the seasons. These seasonal variations are related to climatic factors such as air temperature and humidity.
Footnotes
Acknowledgments
The authors would like to thank all participants for their maximal effort and cooperation. Y.H. participated in the analysis and drafted the manuscript; H.K. and C.H. designed the study and helped to draft the manuscript; N.S. and H.G. provided critical comments on the manuscript.
Disclaimer
The authors received no funding in the form of grants or other on behalf of this research. This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.