
Abstract
Henoch-Schönlein purpura (HSP) is a common systemic vasculitis in children. High-mobility group protein box 1 (HMGB1) is an inflammatory cytokine involved in many autoimmune diseases. This study aimed to examine the expression of HMGB1 in HSP. Fifty-six children with HSP (HSP group) and 32 healthy children (Control group) were enrolled, and their clinic data were collected. Real-time polymerase chain reaction was used to detect mRNA levels of HMGB1, Toll-like receptor 2 (TLR2), TLR4, receptor of advanced glycation end products (RAGE), and nuclear factor-κB (NF-κB) in peripheral blood mononuclear cells (PBMCs). Enzyme-linked immunosorbent assay was used to detect serum levels of HMGB1, interleukin-6 (IL-6), IL-8, and tumor necrosis factor-α (TNF-α). The mRNA levels of HMGB1, TLR2, TLR4, and NF-κB in PBMCs were upregulated in HSP group with kidney injury compared with control group without kidney injury (P < 0.05). The serum levels of HMGB1, IL-6, IL-8, and TNF-α in HSP group with kidney injury were significantly higher than in control group without kidney injury (P < 0.05). There was correlation between serum HMGB1 and TLR2, TLR4, NF-κB, IL-6, IL-8, and TNF-α in HSP group (P < 0.05), and there was correlation between NF-κB and TLR2 and between NF-κB and TLR4 (P < 0.05). HMGB1 is upregulated in children with HSP and correlated with high serum levels of proinflammatory cytokines.
Introduction
H
High-mobility group protein box 1 (HMGB1), a new type of inflammatory cytokine, has been confirmed to participate in the development of inflammatory reaction. HMGB1 is involved in pathophysiological damage of autoimmune diseases and vascular inflammatory diseases.5–7 HMGB1 induces inflammation by combining with various receptors, particularly Toll-like receptor (TLR)2, TLR4, and advanced glycation end products (RAGE), to activate nuclear factor-κB (NF-κB) signaling pathway.7,8 It has been reported that TLR2 and TLR4 rather than RAGE play a significant role in HMGB1-induced activation of NF-κB.9,10
This study aimed to explore the role of HMGB1 in the pathogenesis of HSP in children by comparing mRNA levels of HMGB1, TLR2, TLR4, RAGE, and NF-κB in peripheral blood mononuclear cells (PBMCs) and serum levels of HMGB1, interleukin-6 (IL-6), IL-8, and tumor necrosis factor-α (TNF-α) in HSP children and control children.
Patients and Methods
Subjects
This study was approved by Ethics Committee of Soochow University, and informed consent was obtained from the parents of all participants. Fifty-six pediatric patients with HSP and 32 age- and gender-matched healthy children without any infectious and systematic diseases as the control group were enrolled in this study. The patients with HSP met the classification criteria for HSP 11 and the following inclusion criteria: for children with initial onset, the course was 3 days; children with no other associated medical problems; and children with no history of taking any corticosteroid or cytotoxic drugs.
General information of the subjects and clinical and laboratory data of patients were collected. Alanine aminotransferase (ALT), aspartate transaminase (AST), serum urea, creatinine, Ig, complement, C reaction protein (CRP), D-dimer determination (DD), lymphocyte subsets, urinary sediment, and 24-h urine protein quantitation were defined as clinical routine tests for every patient in the acute phase.
The criteria of hematuria: urine erythrocyte >3 per high-power field in a centrifuge specimen. The criteria of proteinuria: urinary protein >150 mg/24 h. All patients were followed up for 18 months, and physical examination and urine analysis were done during the follow-up.
Blood samples were collected from HSP children and healthy controls and then PBMCs were separated with density gradient centrifugation. Serums were stored at −80°C until they were used.
Real-time polymerase chain reaction
Total RNA from PBMCs was extracted by using TRIzol Reagent. cDNA synthesis was performed by reverse transcription kit (Thermo). Quantitative polymerase chain reaction (PCR) was performed by using SYBR Green I Kit (Thermo) on C1000 Thermal Cycle (Bio-Rad). The primer sequences were as follows: HMGB1 5′-GTTGCGAAGAAACTGGGAGAG-3′ (forward) and 5′-GCTTTTTTCAGCCTTGACAACTC-3′ (reverse); TLR2 5′-TTCCATGGCCTGTGGTATATG-3′ (forward) and 5′-CATCCCGCTCACTGTAAGAAAC-3′ (reverse); TLR4 5′-AGACCTGTCCCTGAACCCTATG-3′ (forward) and 5′-ACCAAACGATGGACTTCTAAACC-3′ (reverse); RAGE 5′-TCCAGGATGAGGGGATTTTC-3′ (forward) and 5′-GGGAACACCAGCCGTGAG-3′ (reverse); NF-κB 5′-AAAGGACCCTGAAGGTTGTGAC-3′ (forward) and 5′-TTCCTGTTGCATACGTTAGAGTGA-3′ (reverse); and GAPDH 5′-GGAGTCCACTGGCGTCTT-3′ (forward) and 5′-GAGTCCTTCCACGATACCAA-3′ (reverse). PCR conditions were as follows: 1 cycle of 95°C for 3 min for degeneration, then 39 cycles of 94°C for 30 s, 52.4°C–60°C for 30 s (52.4°C for RAGE, 58°C for HMGB1, 60°C for TLR2, TLR4 and NF-κB), 72°C for 1 min for PCR amplification, and 1 cycle of 72°C for 10 min for final extension.
Enzyme-linked immunosorbent assay
Serum levels of HMGB1, IL-6, IL-8, and TNF-α were examined by using specific ELISA kits (Elabscience Biotechnology, Wuhan, China) according to the instructions.
Statistical analysis
The data are expressed as the mean ± SD for continuous data and as percentages for categorical variables. Comparison between continuous variables was performed by using the independent t-test. Correlation analysis between parameters was processed by using Pearson correlation analysis. Significance was defined as P < 0.05. Statistical analysis was performed by using SPSS version 19.0 (SPSS, Inc., Chicago, IL).
Results
Patient characteristics
This study included 32 healthy controls and 56 HSP patients, and the comparison is listed in Table 1. All HSP patients had skin involvement, 20 patients (35.71%) had renal involvement, 27 patients (48.21%) had joint involvement at least in 1 joint, 22 patients (39.28%) had gastrointestinal involvement, and 13 patients (23.21%) had both joint involvement and gastrointestinal involvement.
C, complement; CD, cluster of differentiation; CRP, C reaction protein; DD, D-dimer determination; HSP, Henoch-Schönlein purpura; Ig, immunoglobulin.
Among 20 patients with renal involvement, 10 cases, 8 cases, and 2 cases had renal injury as isolated hematuria, hematuria with proteinuria, and isolated proteinuria, respectively. Of patients with isolated hematuria, 1 case had gross hematuria, the other cases had microscopic hematuria. The 24-h urine protein quantitation of patients with renal involvement was 1,059.20 ± 738.54 mg/24 h, which ranged from 168 to 2,612.4 mg/24 h.
All patients had normal blood pressure and normal levels of ALT, AST, serum urea, and creatinine. Forty cases (71.43%) of IgA, 21 cases (37.50%) of IgG, and 13 cases (23.21%) of IgM were more than serum normal range. The positive rate of CRP elevation was 41.07% (23/56). The positive rate of DD elevation was 73.21% (41/56). Six patients had C3 below the normal range. Ten patients had C4 below the normal range, and 13 patients had C4 above the normal range. Among the lymphocyte subsets, the average percentages of CD3−CD19+ lymphocytes and CD19+CD23+ lymphocytes were above the normal range. Patients with renal involvement had higher levels of CRP and DD, and lower IgG and CD3−CD (16+56+) nature killer cell than patients without renal involvement. No significant difference was found in the levels of IgA, IgM, C3, C4, average percentages of CD3+, CD3+CD4+, CD3+CD8+ lymphocyte subsets, and CD4+/CD8+ between the patients with and without renal involvement (Table 2).
C, complement; CD, cluster of differentiation; CRP, C reaction protein; DD, D-dimer determination; HSP, Henoch-Schönlein purpura; Ig, immunoglobulin.
mRNA levels of HMGB1, TLR2, TLR4, RAGE, and NF-κB
As shown in Fig. 1, mRNA levels of HMGB1, TLR2, TLR4, and NF-κB in PBMCs were significantly higher in patients with HSP than in healthy controls. No significant difference in expression of RAGE mRNA was found between HSP patients and healthy controls.

mRNA levels of HMGB1, TLR2, TLR4, RAGE, and NF-κB in children with HSP and healthy controls.
As shown in Fig. 2, mRNA levels of HMGB1, TLR2, TLR4, and NF-κB in PBMCs were significantly higher in patients with renal involvement than in those without renal involvement. No significant difference in expression of RAGE mRNA was found between HSP patients with and without renal involvement. No significant difference of the above indexes was observed between HSP children with or without gastrointestinal symptoms and joint symptoms (data not shown).

mRNA levels of HMGB1, TLR2, TLR4, RAGE, and NF-κB in children with HSP having renal damage and those without renal damage.
Serum levels of HMGB1, IL-6, IL-8 and TNF-α
Compared with healthy controls, significantly increased serum levels of HMGB1, IL-6, IL-8, and TNF-α were observed in patients with HSP (Fig. 3). Compared with HSP patients without renal involvement, significantly enhanced serum levels of HMGB1, IL-6, IL-8, and TNF-α were observed in HSP patients with renal involvement (Fig. 4). There was no significant difference between children with HSP with or without gastrointestinal symptoms and joint symptoms (data not shown).
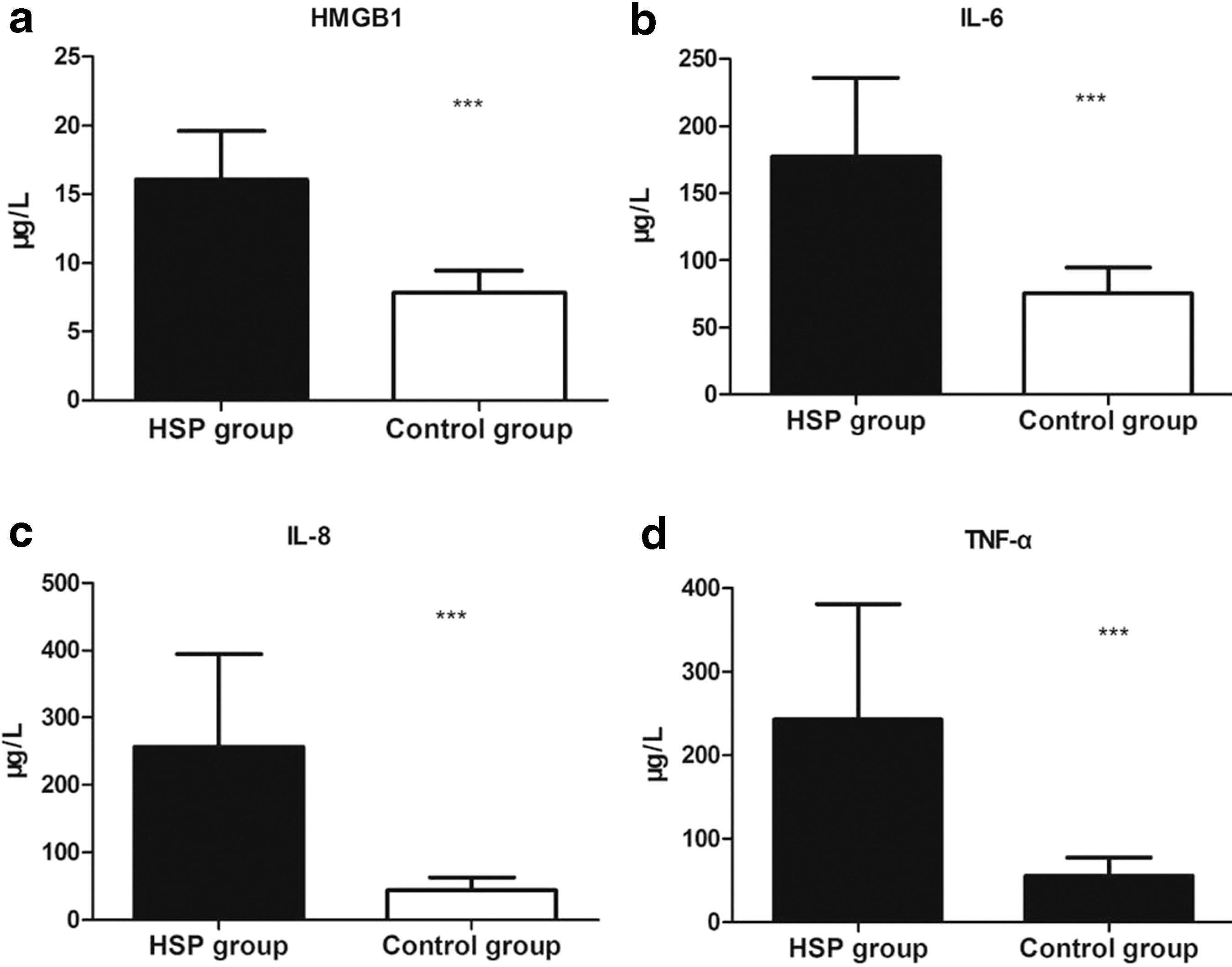
Serum levels of HMGB1, IL-6, IL-8, and TNF-α in children with HSP and healthy controls.
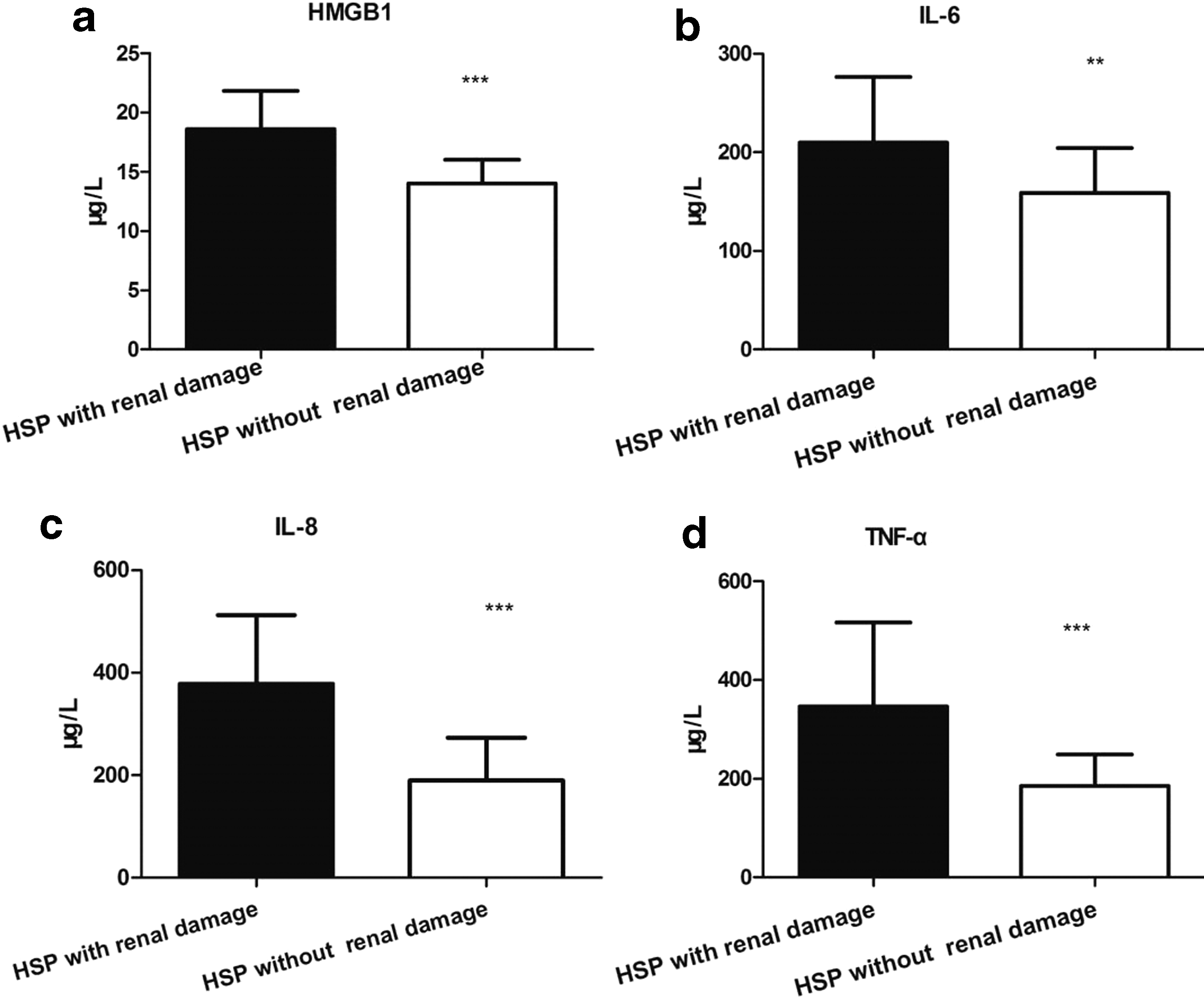
Serum levels of HMGB1, IL-6, IL-8, and TNF-α in children with HSP having renal damage and those without renal damage.
Correlation analysis
Correlation analysis showed a significant positive correlation between serum HMGB1 and TLR2, serum HMGB1 and TLR4, serum HMGB1 and NF-κB, serum HMGB1 and IL-6, serum HMGB1 and IL-8, as well as serum HMGB1 and TNF-α (Table 3). There was a significant positive correlation between NF-κB and TLR2 as well as between NF-κB and TLR4 (r = 0.518, P < 0.001; r = 0.273, P = 0.042, respectively).
IL, interleukin; NF, nuclear factor; TLR, Toll-like receptor; TNF-α, tumor necrosis factor-α.
Discussion
HMGB1 is a nonhistone nuclear protein present in almost all cell types. HMGB1 can be released into the extracellular space. Extracellular HMGB1 plays important role in inflammatory response and immune stimulation by combining various receptors. HMGB1 can activate antigen presenting cells, enhance adaptive immune response, participate in the differentiation, maturation, and activation of T and B lymphocytes, and serve as a key component in the development of many noninfectious inflammatory diseases and tumor.12,13 Studies have confirmed that HMGB1 can activate mononuclear macrophages, neutrophil cells, and other inflammatory cells and promote massive release of many inflammatory factors such as monocyte chemotaxis factor-1, IL-1, IL-6, and IL-8.14,15 Many inflammatory mediators such as CRP, TNF-α, and IL-1 in turn promote monocytes, macrophages, and neutrophils to produce and secrete HMGB1.16–18 Therefore, such a vicious circle triggers cascade inflammation reaction.
We observed that patients with HSP had high proportion of elevated levels of IgA, CRP, and DD and elevated average percentages of CD3−CD19+ lymphocytes and CD19+CD23+ lymphocytes. Meanwhile, patients with HSP having renal involvement had higher levels of CRP and DD and lower IgG and CD3−CD (16+56+) natural killer cell. These data suggest that HSP patients, especially patients with renal involvement, have inflammation, hypercoagulability, and dysfunction of humoral and cellular immune. These findings are consistent with pathological changes in HSP patients.
In this study, we found that levels of HMGB1 mRNA in PBMCs and serum HMGB1 were both increased in children with HSP compared with healthy controls. Meanwhile, we examined the potential role of HMGB1 in HSP children with different clinical features. Our results showed that HMGB mRNA and serum levels were significantly elevated in HSP children with renal involvement compared with those without renal involvement, but no significant difference was observed between HSP children with or without gastrointestinal symptoms and joint symptoms. These findings suggest that HMGB1 could be involved in the pathogenesis of HSP, and patients with higher level HMGB1 are more likely to have renal damage than those with lower level HMGB1. Our results are similar to a previous study, which showed that serum HMGB1 levels were significantly higher in patients with HSP nephritis (HSPN) than in healthy controls, and the specificity of HMGB1 as a diagnostic indicator for HSPN was 71.1%. 19
A variety of cytokines such as TNF-a, IL-2, IL-4, IL-6, IL-8, and vascular endothelial growth factor may participate in the pathogenesis of HSP.20,21 Our study found that serum IL-6, IL-8, and TNF-α levels were elevated in HSP patients compared with healthy controls, and HSP patients with renal damage had significantly higher serum IL-6, IL-8, and TNF-α levels than those without renal damage. Correlation analysis showed that serum HMGB1 level was positively correlated to IL-6, IL-8, and TNF-α levels. Our data are consistent with previous results showing that HMGB1 participated in the pathogenesis of HSP by inducing the production of IL-6 and TNF-α. 22
Accumulating evidence shows that HMGB1 binding to TLR2 and TLR4 induces predominantly downstream NF-κB signaling pathway activation, and activated NF-κB plays a critical role in inflammatory response, endothelial dysfunction, and tumorigenesis by triggering the synthesis of proinflammatory cytokines and chemokines.23,24 Donadio et al. found that children with HSP had significantly increased expression of TLR4 mRNA and a borderline increased expression of TLR2 mRNA, but had no difference in TLR3 and TLR9 mRNAs in the PBMCs of HSP. 25 In this study, we found that mRNA expression of TLR2, TLR4, and NF-κB was upregulated in children with HSP. Moreover, HMGB1 and TLR2, TLR4, and NF-κB showed positive correlation. However, we did not find overexpression of RAGE mRNA in HSP patients and HSP patients with renal involvement. HMGB1 plays an important pathological role in many diseases by combining different receptors in different cell types.7,8 Therefore, it is possible that RAGE may not be the major receptor of HMGB1 that participates in HSP and renal impairment associated with HSP, and HMGB1 induces the inflammatory response in HSP probably by binding TLR2/TLR4 to trigger NF-κB signaling.
TLR2 and TLR4 are expressed in renal tissue and participate in renal diseases partly by interacting with HMGB1 such as glomerulonephritis, transplant rejection, and acute/chronic kidney injury.26–29 Expression levels of TLR2 and TLR4 mRNAs in PBMCs were upregulated in patients with HSP and HSPN, indicating that activated TLR2 and TLR4 possibly mediate the pathogenesis of HSP. 18 Our study indicated that HSP children with renal damage had significantly higher mRNA expression of TLR2, TLR4, and NF-κB than those without renal damage. Based on these data, we speculate that HMGB1-TLR2/TLR4-NF-κB pathway may be involved in renal damage in HSP. Interestingly, a recent study reported that chemokine monocyte chemoattractant protein-1 was elevated in children with HSP and could help evaluate the severity of renal damage. 30
Several limitations of this study should be pointed out. First, this is an observation study, and we did not investigate the mechanism, by which HMGB1 may promote HSP. Second, this is a small sample size and single-center study. Further large-size and multicenter studies are needed to confirm our conclusion. Despite these limitations, our results demonstrate that HSP patients with kidney injury have increased mRNA levels of TLR2, TLR4, and NF-κB and suggest that HMGB1 is involved in inflammatory response and kidney damage in HSP.
Footnotes
Acknowledgments
We thank Hao Li, PhD for technical help and Ting Ye, MS for technical help and writing assistance. We thank all patients and healthy subjects.
Author Disclosure Statement
No competing financial interests exist.