
Abstract
Primary spontaneous pneumothorax (PSP) in pediatric patients is less common than in adults. Tall, thin adolescent males are most commonly affected. While clinical guidelines exist for the adult population, evidence-based recommendations for management of this condition by major respiratory and pediatric societies are lacking. Apparent causes of spontaneous pneumothorax are usually not easily recognized, leading to erroneous classification. Secondary causes must be evaluated carefully before the term PSP is used, as pneumothorax may be a presenting sign for a number of different disorders. Childhood asthma, for example, may be associated with severe hyperinflation, even despite normal spirometry in some situations, which can lead to air leak syndromes, including both pneumothorax and/or pneumomediastinum. In this report, we seek to present a concise review of the current literature, review our own institutional experience with the management of pediatric PSP, and provide insight into the role that asthma may play in pediatric secondary spontaneous pneumothorax.
Introduction
P
SSP occurs as sequelae to an underlying lung pathology, such as chronic obstructive pulmonary disease (COPD) 1 (more common in adults), cystic fibrosis, 2 neoplasm, 3 necrotizing pneumonia, and undiagnosed or poorly controlled asthma.4,5 Consideration should also be given to connective tissue disorders, including Marfan syndrome, Ehlers–Danlos syndrome, and Loeys–Dietz syndrome.6,7 While diagnosis of these syndromes is beyond the scope of this article, it is imperative that patients be referred appropriately to genetic specialists for evaluation and work-up when suspected, as these conditions can have significant multiorgan implications. In young children, pleuropulmonary blastomas can also be a rare neoplastic cause of pneumothorax, which can have a poor prognosis, particularly if the diagnosis is delayed.3,8 Congenital lung lesions, such as congenital pulmonary airway malformations, have also been reported to result in spontaneous pneumothoraces. 9 Other rare diseases have been associated with blebs, bullae, or cysts leading to pneumothoraces, including Langerhans cell histiocytosis (eosinophilic granuloma), 10 Birt–Hogg–Dubé syndrome, 11 folliculin gene mutations, 12 and alpha-1 antitrypsin deficiency. 13 In the proper context, infectious diseases such as tuberculosis or Pneumocystis carinii pneumonia may result in SSP. 14 PSP occurs in patients with no identifiable underlying pathology and should be considered a diagnosis of exclusion. Therefore, diagnosing PSP, especially at first occurrence, requires a thorough investigation to exclude predisposing causes. In addition, SSPs often carry a poorer prognosis and have more complications secondary to the underlying lung pathology. Therefore, many advocate their management should be more aggressive than those with PSP. 15
The exact etiology of PSP remains incompletely elucidated and may be multifactorial in many patients. Most PSPs have their initial onset during rest, although symptoms can start during activity as well. 16 Significant changes in atmospheric pressure and even exposure to loud music may exacerbate underlying predisposing factors, leading to a PSP. 17 The most common prevailing theory is that patients have pre-existing blebs and bullae which rupture, creating a connection allowing air to pass into the pleural space.18,19 However, blebs and bullae can be difficult to detect on standard chest radiography and have been found in up to 20% of healthy adult subjects. Furthermore, blebs and bullae appear less commonly in children. One series reported their presence in only about 28% of children with PSP. 20 In adults, underlying pleural abnormalities such as blebs and bullae are identified much more frequently14,21 and high-resolution computed tomography (HRCT) has shown these to occur in up to 80% of PSP patients. 22 Despite lack of direct evidence, porosity of the pleura has also been implicated in the etiology of PSP and may contribute to air leaks leading to reoccurrence.14,19,22
Epidemiology
In the adult population, there is an estimated incidence of spontaneous pneumothorax of 7.4–18 cases/per 100,000 per year among men, and between 1.2 and 6 cases/per 100,000 among women. 23 The disorder occurs less commonly in children and while there historically has been a paucity of data in pediatrics, 24 there does appear to be a predisposition to male adolescents,25,26 especially in those with low BMI. 27 One study used a large multisite hospital database to calculate an overall incidence of 3.41 cases/year per 100,000 children under the age of 18 in 2006. This was increased from 2.68 cases/year per 100,000 in 1997. The authors speculate this change could be partially due to increased asthma prevalence over the same time period. 28 The average age of presentation in the pediatric population is estimated to be 14–16 years15,16,26,28,29 with a significant difference between males and females, with an average ratio of 4.2:1.15,28
Periods of accelerated growth before and during puberty may be risk factors, as rapid increases in chest height and width have been associated with PSP. 30 Chest wall configuration has also been implicated as a potential risk factor as male patients who had a history of PSP had a flatter anteroposterior diameter and a more laterally narrow and craniocaudally taller thorax than age- and sex-matched controls. 31
Our Experience
Similar demographics were seen at our urban, academic institution. Approval from our local Institutional Review Board was obtained to retrospectively review records from our site. From March 2013 to March 2017, there were a total of 108 encounters (Emergency Department visits or inpatient admissions) for 61 unique patients 1–18 years of age with a confirmed diagnosis of PSP. Seventy seven percent of the patients were male with an average age at first presentation of 14.7 years. Around 73.8% of the patients were between the ages of 14 and 18 with 60.6% being males between 15 and 17 years of age. The proportion of patients under 10 years of age was 8.1%, a ratio comparable to other studies with rates between 0% and 15%.26–28
In addition to these patients, we followed a unique series of three patients with spontaneous pneumothorax with severe undiagnosed hyperinflation as a possible etiology based on each child having a markedly elevated residual volume, despite otherwise normal spirometry. The first patient (A) presented at 14 years of age, the second patient (B) at 17 years of age, and the third patient (C) at 7 years of age. All three were managed with supplemental oxygen ranging from 50% to 100%. Pulmonary function tests were performed within 10 days of the pneumothorax (Table 1).
Lung Volumes of Three Children with Spontaneous Pneumothorax
Patients A and B demonstrated increased lung volumes as evidenced by elevated total lung capacity. Additionally, there is evidence suggestive of air trapping as both functional residual capacity as well as residual volume are significantly elevated.
All three patients had a history of childhood asthma. Follow-up ranged from 6 to 17 months. All patients were treated with aggressive asthma regimens of bronchodilators, anticholinergics, and inhaled corticosteroids. No patient required surgical or chemical pleurodesis. We speculate that PSP developed secondary to severe unrecognized hyperinflation, which may be related to untreated asthma. Therefore, appropriate treatment of asthma may eliminate the recurrence of pneumothorax and obviate the need for surgical intervention. 32
It appears from the clinical data and the response to asthma therapy that our patients had air trapping and hyperinflation, most likely due to distal airway obstruction. The fact that all had normal spirometric values is somewhat puzzling, making the diagnosis of asthma and COPD uncertain based on current accepted guidelines and criteria. The most commonly used spirometric and bronchoprovocation measurements that define asthma and COPD assess the large airway function, but small airway dysfunction is always present in patients with asthma and chronic obstructive lung disease. Common spirometric tests, such as the forced mid-expiratory flow (FEF25–75), traditionally thought to reflect small airway function, are highly variable and have poor sensitivity. Advances in lung function testing show that this parameter does not provide adequate measure in lung diseases where small airway dysfunction predominates.
Based on our data, we speculate that small airway disease and hyperinflation lead to uncoupling of the airway–parenchymal interdependence. Inflammation of the distal airways results in a separation of these two compartments. With edema or inflammatory exudates in the peribronchial space, the peribronchial pressure becomes less negative and the elastic load pulling the airway open will decrease. Furthermore, when the parenchymal attachments are exposed to repeated stress, they break down and their effectiveness of holding the airways open diminishes. This leads to over distension and rupture of the alveolar sacs.33,34
Diagnosis
Typically, PSP can be clinically suspected based solely on history and physical examination. Classic symptoms include acute onset of chest pain with or without significant shortness of breath. The pain can range from minimal to severe with a sharp and stabbing quality that progresses to a steady ache. It tends to be pleuritic with worsening on deep inspiration and is most often localized to the affected side. Pain will often subside spontaneously, even if the pneumothorax remains and this can lead to delayed presentation and diagnosis. 23 In a large, retrospective cohort of pediatric patients, chest pain was the most common presenting symptom (87% of patients) with shortness of breath present in 43%. Cough was seen in only 5% of patients. 16
Commonly encountered physical exam findings include ipsilateral diminished breath sounds, hyperresonant percussion, dyspnea, decreased vocal fremitus, decreased chest wall movement, and tachycardia. These findings are more often observed in patients with larger pneumothoraces, whereas those with smaller lesions may have no obvious physical examination findings.
The diagnosis of pneumothorax is confirmed by upright posterior–anterior (PA) chest radiography. Lateral or lateral decubitus views may be useful in detecting small pneumothoraces not visible on PA films. 35 Figure 1 demonstrates a large pneumothorax easily visible, whereas Fig. 2 shows a small apical pneumothorax which is more subtle. The value of expiratory versus inspiratory chest radiographs remains unclear. However, there does appear to be more utility in inspiratory films in confirmation on initial presentation.36,37 Studies have also shown a higher sensitivity and specificity in diagnosis using ultrasonography compared with radiography,38–40 although ultrasound accuracy is dependent upon the skill of the operator.40,41 This limits its utility as a first-line diagnostic tool, especially in the pediatric setting.
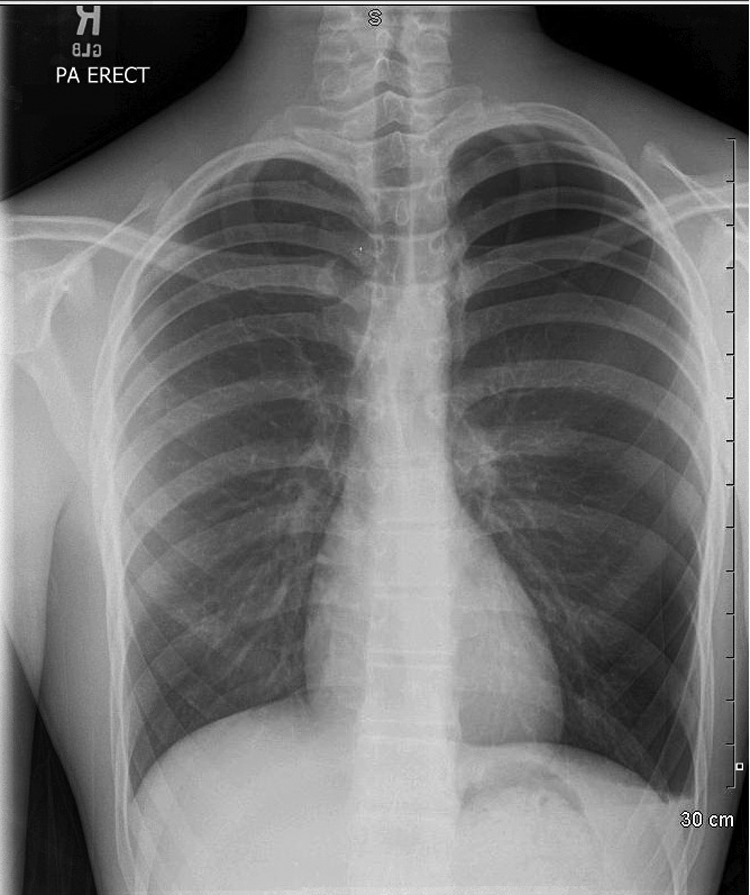
Large left-sided pneumothorax on posteroanterior chest radiograph in a 15-year-old male with asthma and a 5-day history of intermittent stabbing left-sided chest pain and associated dyspnea. A small pleural effusion is also present. He underwent chest tube placement upon presentation and wedge resection of apical blebs with talc pleurodesis on hospital day 4. Extensive evaluation for other underlying causes was unrevealing.

Small apical right-sided pneumothorax (arrows) on posteroanterior chest radiograph in a 16-year-old otherwise healthy male with sudden onset severe chest pain and associated dyspnea. He was initially treated with oxygen therapy but eventually required chest tube placement after recurrence.
Chest CT scans are often used as an adjunct diagnostic method when there is high clinical suspicion and conventional radiography is equivocal. There remains no consensus, however, on exact indications for utilization of CT. Chest CT can identify small pneumothoraces not detected on chest radiography and is useful for revealing apical blebs, which may be missed by a standard chest radiograph. Rates of bleb detection with standard chest CT and confirmed with surgery is not uniform and ranges from 36% to 59%20,42 but improves significantly with use of HRCT. HRCT has been reported to have a sensitivity for detecting blebs and bullae between 94% and 97%. 43 The clinical significance of apical blebs is unclear with some studies suggesting presence of apical blebs as a risk factor for recurrence44,45 while others contend that the findings of blebs are not predictive 46 and do not require surgical intervention. 47 In addition to blebs and bullae, other findings on HRCT which may be found in patients with PSP include pleural thickening, subpleural consolidation, or linear opacities in the pulmonary apex of patients. 48 The decision to obtain a CT scan should involve the opinion of the consulting pediatric surgeon to help determine how the findings will affect the need for either conservative or surgical management versus the increased exposure to radiation, which is always a consideration in pediatric patients.
Management
The fundamental goals of treatment are two-fold: total re-expansion of the lung with removal of air from the intrapleural space and recurrence prevention. There are no definitive guidelines for the management of pediatric PSP. Several guidelines, which vary in their approach, exist for adult populations, from which pediatric management is often extrapolated. Guidelines or consensus statements for adult management have been released by the British Thoracic Society (BTS) in 2010 49 and the American College of Chest Physicians (ACCP) in 2001. 50 The European Respiratory Society (ERS) released a task force statement in 2015, which summarized the current literature and proposed key questions for future research but did not make specific management recommendations. 51
Variations in definitions regarding the size of a pneumothorax and management recommendations have led to confusion and wide variations in practice. 52 BTS guidelines define a large pneumothorax as having a viable rim of air greater than 2 cm between the chest wall and lung margin. ACCP criteria specify a 3 cm or greater distance from the apex to the chest wall apex. Likewise, while both societies recommend conservative management for small lesions in stable patients, BTS guidelines suggest needle aspiration as first-line management in large pneumothoraces or in unstable patients, whereas ACCP guidelines go directly to intercostal chest drain placement. Some of the practice differences can be partly explained by preferential differences between medical and surgical specialties53; however, with these variations there remains no overarching consensus. To complicate the landscape, the guidelines focus almost entirely on the adult population, leaving no expert group consensus or guidelines regarding management of spontaneous primary pneumothorax in the pediatric population.
Medical management
Recently, conservative management of PSP has gained popularity due to the changing notion that evidence of intrapleural air does not necessarily require surgical corrective intervention. The BTS outlines its management algorithm around the presence of symptoms, specifically breathlessness, as opposed to the size of pneumothorax. Both the BTS and ACCP recommend that small, asymptomatic pneumothoraces can be managed conservatively and often as an outpatient.49,50 However, the ACCP's recommendations become more aggressive with larger pneumothoraces, with “very good consensus” that large pneumothoraces should undergo re-expansion procedures (with intercostal chest drain placement as first-line therapy) and be managed as an inpatient.
Initial management of PSP patients with small lesions, who are clinically stable and without any evidence for cardiopulmonary compromise, is noninvasive and consists primarily of observation with full cardiorespiratory monitoring and administration of 100% high-flow oxygen typically through nonrebreather face mask. This can increase the resolution rate of PSP 54 and enhance absorption of gases from the extrapleural space. This is accomplished by reducing the partial pressure of nitrogen in the alveolus creating a diffusion gradient that allows for nitrogen to “wash out” of the pleural space, speeding resolution of the pneumothorax. Clinical staff should be educated on rationale for use of supplemental oxygen in this setting and that premature discontinuation may hinder resolution. Chest radiography should be repeated about 12 h after initiation of therapy. If the patient worsens either clinically or radiographically, surgical intervention is indicated. The role of strictly conservative management with close outpatient follow-up, advocated in small, stable lesions in adults by both BTS and ACCP guidelines, is unclear in pediatric patients. For adults, ACCP guidelines suggest observation for 3–6 h in the Emergency Department with follow-up in 12–24 h. These guidelines are based on the assumption that patients have immediate access to an emergency department if symptoms were to arise or worsen. This can often complicate the management plan in the pediatric population as pediatric emergency departments are not as widely distributed as those serving adult patients. Special consideration should be given to pediatric patients with PSP as no specific outcome predictors have been established in this population.
Invasive management
The ACCP and BTS agree that symptomatic adult patients cannot be treated solely with conservative management. There are three nonoperative, yet nonetheless invasive, options: (1) needle aspiration, (2) pigtail (usually 8 French) tube thoracostomy/pleural catheter placed by Seldinger technique, and (3) direct placement of tube thoracostomy through chest incision (any size tube). BTS guidelines outline needle aspiration as the first-line intervention for those requiring procedural management, whereas the ACCP prefers pleural catheter or thoracostomy tube placement. In adults, there is continued controversy regarding needle aspiration compared with chest tube placement with similar immediate success results but shorter hospital stay duration for needle aspiration.55–57 However, some studies have shown that needle aspiration in children, especially in larger pneumothoraces, is ineffective. 58
An additional consideration is patient tolerance. Older, cooperative, and not-overly-anxious children tolerate needle aspiration and even pigtail thoracostomy placement fairly well, but other children may require sedation (or even general anesthetic) for these procedures. Open tube thoracostomy, while performed routinely for adults while awake, is painful even while sedated, and may not be appropriate for the anxious teenager. These larger thoracostomy tubes are often placed for higher-risk patients, such as recurrence of pneumothorax, suspicion of air leak, underlying lung disease, etc.
Needle aspiration is a one-shot attempt at resolution of pneumothorax. If there is insufficient evacuation or reaccumulation of pneumothorax, then tube thoracostomy must be placed. The pigtail and larger tube thoracostomies have the advantage of connection to negative pressure devices (ie., Pleur-evac, Thora-Seal), actively evacuating the pneumothorax, and/or controlling any air leak. In our experience, the small, 8 French pigtail catheter is excellent for evacuation of pneumothorax, but poor at controlling air leak if present. Air leak usually requires a large-caliber thoracostomy tube to evacuate the extrapleural air as fast as or faster than it exits the lung.
If needle aspiration is effective at alleviating symptoms, and full or nearly full evacuation of the pneumothorax is achieved, then the patient may qualify for discharge, with close follow-up by plain film chest radiograph. Of course, this may not be prudent if the child's social situation or transportation availability is not acceptable. If the child is still symptomatic, or requires negative pressure to evacuate the pneumothorax, then he or she should be admitted to the hospital and observed. Hospital management of PSP with chest tube and negative pressure device is widely variable among practitioners, but usually requires serial plain film x-rays, a variable amount of time on suction, and then either water seal trial or simply removal of the thoracostomy tube. Collapse of the lung on water seal, or persistent air leak despite suction, may warrant several days of therapy to remedy. The ACCP recommends up to 4 days before abandoning simple tube thoracostomy and consideration of surgical therapy.
Surgical management
Video-Assisted Thoracoscopic Surgery (VATS) or open thoracotomy procedures are usually reserved for ineffective attempt at chest drainage, recurrent pneumothorax, bilateral pneumothoraces, or persistent air leak. Surgical goals include full expansion of the lung, control of air leak, and prevention of recurrence. Recurrence of pneumothorax in the PSP population is often due to blebs. Blebectomy is the treatment of choice, and is usually performed by nonanatomic (ie., not complete lobectomy) stapling and removal of the blebs/bullae from the apex of the lung.
Most pediatric and thoracic surgeons add a pleurodesis or pleurectomy procedure to the blebectomy to minimize recurrence rates. If there are no blebs/bullae present, then pleurodesis or pleurectomy alone is the procedure of choice. Pleurodesis is the intentional creation of adhesions between the chest wall and the lung. This is achieved mechanically by abrading the chest wall (parietal pleura), or chemically by instillation of an inflammatory substance, such as talc, tetracycline, minocycline, and doxycycline. Pleurectomy involves removal of the parietal pleura. There is relative agreement that mechanical pleurodesis and pleurectomy are more successful in preventing recurrent pneumothorax than chemical means. One advantage of chemical pleurodesis is that it can be performed without surgical intervention, through an indwelling thoracostomy tube. One distinct disadvantage of chemical pleurodesis is that it is even more painful than mechanical pleurodesis. Both mechanical and chemical pleurodesis techniques can be combined, as we often do at our institution, particularly for patients at high risk for recurrence.
Long-Term Outcomes
Recurrence rates for PSP have been reported to be as high as 50% in untreated adults, with recurrence rates in conservatively managed pediatric patients being reported between 40% and 60%.15,26,59,60 Rate of recurrence after VATS alone in pediatric patients was about 50% in one series. 61 In adults, recurrence rates after definitive treatment with blebectomy and pleurectomy have been reported to be less than 2%, 15 whereas in one series of pediatric patients, those undergoing blebectomy and mechanical pleurodesis had a rate of recurrence of 14% (vs. 45% in the nonoperative group). 59
In addition to monitoring for signs and symptoms of recurrence, patients and their families should be counseled on long-term risk management strategies to help prevent further episodes. Any method of smoking, including tobacco and marijuana, should be strictly avoided. Air travel is absolutely contraindicated in patients with an unresolved pneumothorax, and BTS guidelines on air travel suggest that a clear reduction in recurrence risk does not occur until 1 year after the initial event in the absence of definitive surgical management. 62 Likewise, BTS guidelines state that diving should be permanently avoided after a pneumothorax unless definitive, bilateral surgical intervention with pleurectomy is performed and a chest CT and lung function are both normal postoperatively. 49
Conclusions
While PSP in the pediatric population is less common than in adults, there is a strong adolescent male predominance, which is seen in the available literature and consistent with the demographics of our institution. Despite its relative frequency in pediatric practices, evidence-based guidelines for management of PSP are still lacking. While nonoperative management may predominate in stable children with an initial, small pneumothorax, recurrence rates are often high and invasive management often required. A thorough investigation should be done to exclude both common and uncommon contributing lung pathology. More research is needed to develop pediatric-specific guidelines on both initial and long-term management.
Footnotes
Author Disclosure Statement
The following authors disclose that they have no financial interests or other conflicts of interest in the subject of this article: Jacob Kaslow, MD, Scott Bickel, MD, Chad Wiesenauer, MD, Nemr Eid, MD, and Ronald Morton, MD.