
Abstract
Background:
Recurrent wheeze (RW) is frequent in preschool children. Wheezing phenotypes, asthma predictive index (API), and modified API (mAPI) have been described for clinical purposes. Our aim was to examine whether inflammatory markers including serum angiopoietin (Ang)-1, Ang-2, and periostin levels differ according to wheezing phenotypes and mAPI.
Materials and Methods:
Ninety-eight children who were <4 years of age with history of at least 4 episodes of wheezing during the past 12 months and 51 age-matched healthy controls were included in the study. Children with RW were classified according to wheezing phenotypes as episodic viral wheeze or multitrigger wheeze, and positive or negative mAPI. Blood for Ang-1, Ang-2, and periostin levels was drawn during wheezing episode-free periods.
Results:
Atopic children with RW (31.4 ± 34.4 ng/mL) demonstrated higher serum Ang-1 levels than nonatopic children (16.5 ± 13.8 ng/mL) with RW (P = 0.03). When we compared children according to wheezing phenotypes, we could not find any difference in serum Ang-1, Ang-2, and periostin levels between groups. Children with positive mAPI showed similar Ang-1, Ang-2, and periostin levels with children having negative API and healthy children.
Conclusions:
We have found higher serum Ang-1 levels in atopic children with RW, and this result might be explained by increased inflammation. The evidence was not strong enough to associate serum Ang-1, Ang-2, or periostin and asthma in preschool children with RW. However, Ang-1 can be a candidate for investigating its role in predicting atopic children and diagnosing atopic childhood asthma.
Introduction
R
RW may be the first clinical sign of asthma in first years of life, however, which child with RW will have asthma in later childhood cannot be easily estimated. Wheezing phenotypes according to symptoms have been described for clinical purposes in preschool children with wheezing disorders as episodic viral wheeze (EVW) and multitrigger wheeze (MTW). 3 Asthma predictive index (API) and modified API (mAPI) for determining the risk of future asthma in children with RW were developed.4,5 However, using API, mAPI, and symptom-based phenotypes may not always help to predict future asthma, and there is also no established biomarker for diagnosis of childhood asthma in children with RW.
Asthma is a chronic inflammatory disease of airways. Angiopoietins (Ang) have a key role in regulating inflammation and maintaining homeostasis of endothelial cells. Ang-1 is an essential mediator of angiogenesis that establishes vascular integrity and Ang-2 acts as its natural inhibitor. Ang-1 and Ang-2 have been shown to involve in pathogenesis of asthma.6–8 Periostin is an extracellular matrix protein associated with Th2 inflammation and upregulated in response to interleukin (IL)-4 and IL-13. Serum periostin is found to be correlated with eosinophilic airway inflammation and related with pediatric asthma.9,10
Researches for finding biomarkers to diagnose asthma in early childhood particularly in children with RW attract attention.11,12 Our aim was to examine serum Ang-1, Ang-2, and periostin levels in children with RW, and demonstrate whether Ang-1, Ang-2, and periostin differ according to wheezing phenotypes and mAPI.
Materials and Methods
Children who were <4 years of age with the history of at least 4 episodes of wheezing during the past 12 months were included in the study. Children with RW were enrolled from outpatient clinics of pediatric allergy unit and pediatrics department, and healthy children were enrolled from outpatient clinics of pediatrics department. At the time of visits, all the children underwent clinical examination and parents were asked whether their child had any history of allergic disease and physician-diagnosed RW. Parents of the child with RW were also asked about the presence of symptoms in episode-free periods, age at first wheeze, frequency of wheezing during past 12 months, and night symptoms, asthma symptoms, and short acting b2-agonist need in a week during the past month. Wheezing episodes were diagnosed by a general pediatrician or a pediatric allergist.
Characteristics of subjects with RW and age-matched healthy controls were compared. Children who had wheezing episode and/or systemic steroid treatment at the time of evaluation or during the past 3 months were excluded from the RW group. Subjects with any allergic disease, history of asthma symptoms, allergic rhinitis symptoms, or wheezing episode were excluded from the control group. Children were further classified according to wheezing phenotypes. Children who had wheezing only during viral colds and had no symptoms between wheezing episodes were included in the EVW group. Children who had wheezing not only with viral colds but also between wheezing episodes and with other triggers, including allergens, cold air, cigarette smoke, exercise, crying, or laughter, were included in MTW group.
We also compared subjects with RW according to mAPI. mAPI was considered as positive when 1 major or 2 minor clinical criteria were present in children with RW. 5 The major criteria include parental history of asthma, physician-diagnosed atopic dermatitis, and allergic sensitization to at least 1 aeroallergen. The minor criteria include wheezing unrelated to colds, peripheral blood eosinophils ≥4%, and allergic sensitization to food(s). Children who had allergy to aeroallergens and/or food(s) according to skin prick tests or serum tests were defined as atopic. Results of epidermal skin prick tests, specific IgE to cow's milk and hen's egg, and complete blood counts were obtained from the medical records. Epidermal skin prick tests for Dermatophagoides farinae, Dermatophagoides pteronyssinus, Alternaria alternata, Cladosporium herbarum, Aspergillus fumigatus, grass mix, tree mix, weed mix, cereal mix, and cat were performed.
Blood was drawn during wheezing episode-free periods. Blood samples were obtained from all participants and were stored at −80°C. Serum Ang-1, Ang-2, and periostin levels were measured by ELISA (Cusabio®) according to manufacturer's instructions. The minimum detection limits for Ang-1, Ang-2, and periostin were 0.091, 0.31, and 1.56 ng/mL, respectively.
Written informed consent was obtained from all parents before the study.
Statistical analysis
The results of tests are expressed as the number of observations (n), mean ± standard deviation, median, and min-max values. Shapiro–Wilk's test was used to assess the normality of distributions of the variables, and Levene's test was used to assess the homogeneity of variances between groups. If parametric test assumptions were available, 2 normally distributed independent groups were compared by Student's t-test and correlations between variables were analyzed by Pearson correlation coefficient. If parametric test assumptions were not available, for comparison of 2 independent groups Mann–Whitney U test was used and correlations between variables were analyzed by Spearman's ρ correlation coefficient.
Three or more groups were compared by Analysis of Variance and Tukey HSD (Honest significant difference) multiple comparison tests. If parametric test assumptions were not available, comparisons of 3 independent groups were performed by Kruskal–Wallis test or Bonferroni–Dunn test. Categorical data were analyzed with Fisher's exact test and χ2 test. The exact and Monte Carlo methods provide means for obtaining accurate results when the data fail to meet any of the underlying assumptions necessary for reliable results using the standard asymptotic method. All statistical analyses were performed with the SPSS software (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.) P value of <0.05 was considered as statistically significant.
Results
Ninety-eight children (47 EVW and 51 MTW) with RW and age-matched 51 healthy children were included in the study. Characteristics of participants are presented in Table 1.
Characteristics of Children with Recurrent Wheeze and Healthy Subjects
Values are mean ± SD unless otherwise indicated.
Median (IQR) value.
Ang, angiopoietin; CRP, C-reactive protein; IQR, interquartile range; SD, standard deviation.
Serum Ang-1, Ang-2, periostin levels, and Ang-1/Ang-2 ratio did not show any difference between RW and control groups (Table 1).
Thirteen children with EVW and 38 children with MTW had positive mAPI. When we compared children according to wheezing phenotypes, we could not find any difference in serum Ang-1, Ang-2, periostin levels, and Ang-1/Ang-2 ratio between groups (Table 2). Children with positive mAPI had no difference in Ang-1, Ang-2, periostin levels, and Ang-1/Ang-2 ratio compared with children with negative API (Table 3).
Characteristics of Children with Episodic Viral Wheeze, Multitrigger Wheeze, and Healthy Subjects
Values are mean ± SD or number (%) unless otherwise indicated.
Median (IQR) value.
Ang, angiopoietin; API, asthma predictive index; CRP, C-reactive protein; Hb, hemoglobin; IQR, interquartile range; SD, standard deviation.
Characteristics of Children with Positive and Negative Asthma Predictive Index
Values are mean ± SD unless otherwise indicated.
Median (IQR) value.
Ang, angiopoietin; API, asthma predictive index; IQR, interquartile range; SD, standard deviation.
Atopic children with RW (31.4 ± 34.4 pg/mL) demonstrated higher levels of serum Ang-1 than nonatopic children with RW (16.5 ± 13.8 pg/mL) (P = 0.03) (Fig. 1). There was no significant difference in serum Ang-2 (13 ± 8.3 pg/mL versus 10.7 ± 9 pg/mL) and periostin (108.7 ± 113.6 ng/mL versus 88.5 ± 74.7 ng/mL) levels between atopic and nonatopic children with RW (Table 4).
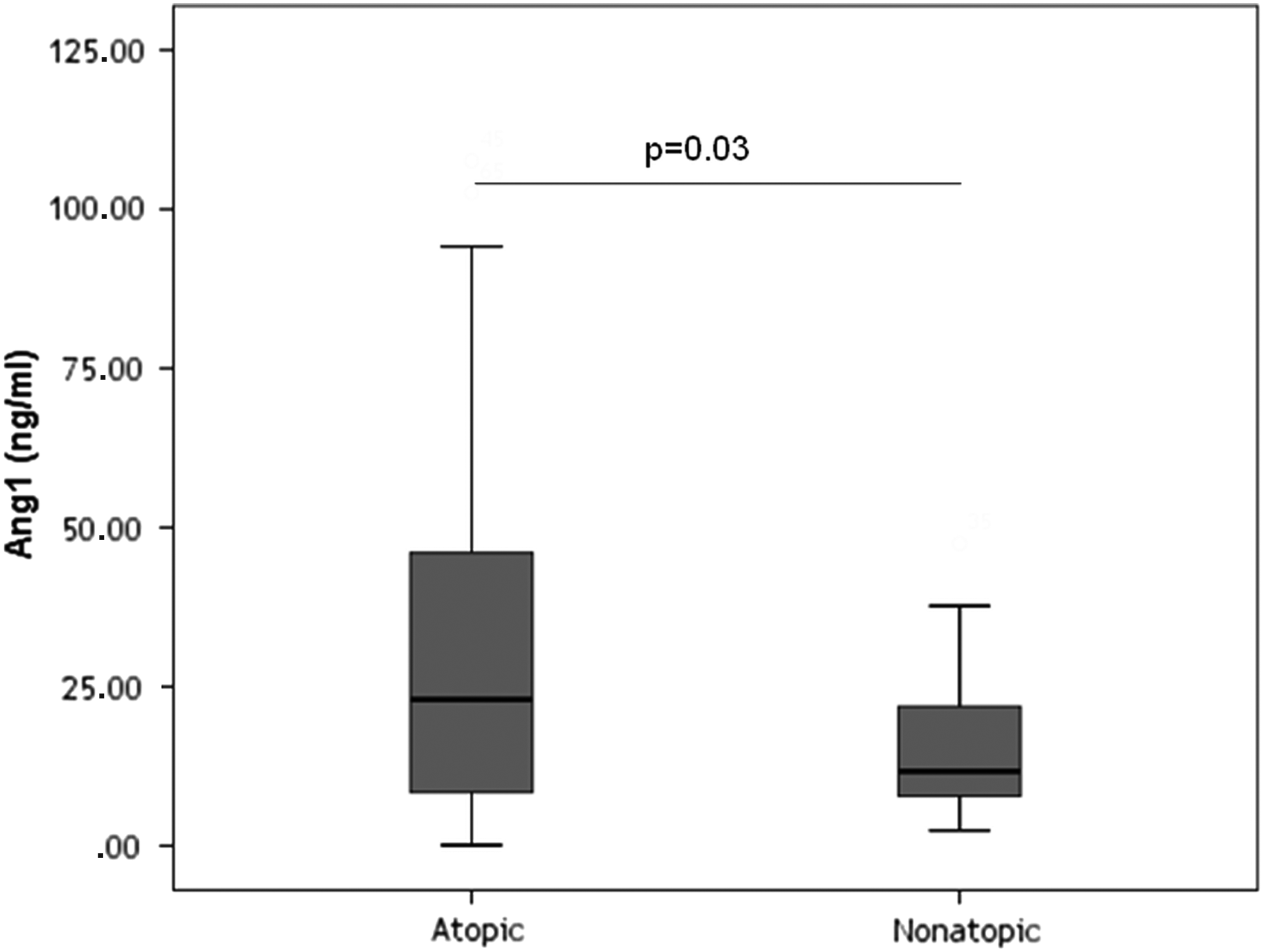
Comparison of serum Ang-1 levels between atopic and nonatopic subjects. Ang, angiopoietin.
Angiopoietin-1, Angiopoietin-2, Ang-1/Ang-2 Ratio, and Periostin Levels of Wheezy Children With Atopy and Without Atopy
Values are shown as mean ± SD and amedian (IQR).
Ang, angiopoietin; IQR, interquartile range; SD, standard deviation.
Frequency of treatment using children was higher in MTW (68.4%) than in EVW (31.6%) group (P = 0.01). Thirty-eight children (12 EVW, 26 MTW) were receiving continuous treatment with inhaled steroid and/or montelukast. Children with positive API (73.7%) had more frequent treatment than children with negative API (26.3%) (P = 0.04).
Eighteen patients had a high (>400 cells/μL) peripheral eosinophil count. Ang-1, Ang-2, and periostin levels were similar between children with high (>400 cells/μL) and low (<400 cells/μL) peripheral eosinophil counts.
Frequency of RW, EVW, or positive API was higher in boys than girls (P < 0.01, P < 0.001, P < 0.01, respectively). Serum Ang-1, Ang-2, and periostin levels showed no association with gender in either RW or control groups.
Age at first wheeze was lower in EVW (9.5 ± 6.9 months) than in MTW (15.5 ± 8.9 months) group (P < 0.001) (Table 2). Frequency of days with asthma symptoms in a week during past month was positively correlated with Ang-1 levels (r:0.35, P < 0.05). No significant correlations were observed between Ang-1, Ang-2, periostin levels, and duration of disease, age at first wheeze, or frequency of wheezing during the past 12 months.
Discussion
Diagnosing asthma and deciding to start control treatment for children with RW <4 years of age can be difficult for clinicians in daily practice. API, mAPI, and phenotypes including EVW and MTW have been described for this purpose. The identification of biomarkers of childhood asthma is an active area of research. 13 In this study, we wanted to examine serum Ang-1, Ang-2, and periostin levels in children with RW during symptom-free periods and we also wondered whether Ang-1, Ang-2, and periostin levels help to guide clinicians for diagnosing pediatric asthma. Our data indicated higher Ang-1 levels in atopic children with RW than in nonatopic children with RW. This result allows us to suggest that Ang-1 can be a candidate for investigating its role in diagnosing atopic childhood asthma.
Children with a positive API or mAPI are at increased risk of developing asthma. A stringent API has been statistically validated as a clinical tool for asthma prediction. 4 So that we have chosen children with at least 4 episodes of wheezing during the past year. Ang-2 and periostin levels did not show any difference between groups. However, Ang-1 levels were higher in atopic children with RW than in nonatopic wheezers, and frequency of days with asthma symptoms in a week during the past month was also positively correlated with Ang-1 levels. Although statistically not significant, Ang-1 level was higher in the MTW group than in the EVW group and it was also higher in the API positive group than in the API negative group. All of these results may support the notion that Ang-1 is related to inflammation. We believe that future studies including higher number of children with RW may also show significant results between MTW and ETW or between positive API and negative API groups.
Ang-1 and Ang-2 are involved in the pathogenesis of asthma.14,15 Ang-1 protects against microvascular leakage and has anti-inflammatory properties. 16 Simoes et al. proposed that Ang-1 levels may rise to provide vascular integrity. 6 We think that Ang-1 levels may remain high to protect vascular integrity and decrease inflammation, particularly in atopic children with RW. Since Ang-1 is an anti-inflammatory and protective protein, when inflammation increases, Ang-1 levels may also increase to protect airways. Moon et al. demonstrated higher serum Ang-1 levels in patients with asthma and suggested that Ang are useful markers for the diagnosis of asthma. 8 Since children with atopy and positive mAPI have more risk to develop asthma, our data may also support these results.
In our previous study, we found that children with asthma had lower serum Ang-1 levels than healthy children. 7 Those children had stable asthma and were using inhaled steroid treatment. We think that Ang-1 levels may fluctuate according to use of asthma medication and asthma control levels. Since Ang-1 is a protective protein, in earlier childhood Ang-1 levels may increase in wheezy children who will develop asthma in later childhood.
Higher serum Ang-1 levels may indicate inflammation and asthma in children. However, serum Ang-2 and periostin do not seem to help in predicting childhood asthma. As a consequence of choosing children who did not have wheezing episode or systemic corticosteroid treatment at the time of evaluation and during the past 3 months, Ang-2 and periostin levels may have showed similar results with healthy controls in our study. We think that Ang-2 and periostin levels return to normal levels when the inflammation is under control and during wheezing episode-free periods. For definite results, future studies including wheezing episodes and prospective follow-up of the children with RW are needed to show which patients will develop asthma.
Lee et al. showed increased circulating Ang-2 in patients with exacerbated asthma, and their results suggested that Ang-2 levels are decreased to recruit inflammatory cells leading to less severe airway obstruction. 14 Ang-2 is stored in Weibel-Palade bodies predominantly in the cytoplasm of endothelial cells and quickly secreted when needed. Plasma Ang-2 levels were correlated with blood eosinophil proportions and with the severity of airway occlusion. 14 Since our patients had no wheezing episode at the time of evaluation and small number of patients had high eosinophil counts, we may have found similar Ang-2 levels with controls.
Periostin has also been shown to be involved in allergic inflammation, and periostin levels were found higher in children with asthma than in healthy controls.17–19 In our study, we could not find a difference in periostin levels between EVW and MTW phenotypes or between children with positive and negative mAPI. Similar to our study, Castro-Rodriguez et al. found that serum periostin is not related to API. 20 Since we could not show any difference in periostin levels between groups, we think that periostin is not helpful in diagnosing early childhood asthma during wheezing episode-free periods. We consider that periostin would guide the clinicians to diagnose asthma in children with older ages or adults. In contrast, periostin seems to be a reliable protein to determine eosinophilic asthma. A significant correlation has been demonstrated between periostin and blood eosinophil counts.18,19 In our study, only 18 patients had a high peripheral eosinophil count. We may have found similar periostin levels between groups due to small number of patients with a high peripheral eosinophil count. Inogue et al. suggested that measuring serum periostin, FeNO, and eosinophils could improve diagnosis of asthma. 10 Anderson et al. described that high periostin levels (>150 ng/mL) and high eosinophil counts (>300 cells/μL) at the age of 2 years may predict future asthma at the age of 6 years. 21 We believe that as long as new cutoff levels of biomarkers for different ages are described, we will be able to predict later childhood asthma. Future prospective studies in which periostin levels will be measured in different age groups will shed light on this subject.
Our work is the first study examining Ang-1 and Ang-2 levels in children with RW. We have chosen children with frequent wheeze that would support asthma, and we evaluated children with positive mAPI. Our results referred to atopy, but not asthma. Ang-1 might be used to detect atopic children <4 years of age. Limitations of our study are including limited population and relying on clinical criteria of positive API and wheezing phenotypes. A longitidunal study would be performed to evaluate how many wheezers with elevated inflammatory markers will develop asthma.
In conclusion, we showed that serum Ang-1 levels were higher in atopic children with RW than in nonatopic children with RW. Since we have found higher serum Ang-1 levels in atopic children, this result might be explained by increased inflammation. The evidence was not strong enough to associate serum Ang-1, Ang-2, or periostin and asthma in preschool children with RW. However, serum Ang-1 may help to predict atopy and diagnose asthma, particularly in atopic children with RW. Further studies with longitudinal design, including children with different age groups and different disease states, are needed to understand the roles of Ang and periostin in children with RW.
Footnotes
Acknowledgments
This study was approved by Baskent University Ethical Committee (KA15/378) and supported by Baskent University research fund.
Author Disclosure Statement
No competing financial interests exist.