
Abstract
Background:
Type 3 von Willebrand disease (VWD) is a severe bleeding disorder with a prevalence of 1:1 million live births. There are several von Willebrand factor (VWF) replacement products used in the treatment of acute bleeding episodes or as prophylaxis. Patients who receive multiple transfusions have an increased risk of developing antibodies against these products. These antibodies can lead to life-threatening anaphylactic reactions. Previous studies have identified immune complex formation and complement activation as the trigger for anaphylaxis, rather than IgE. IgE-mediated anaphylaxis against VWF concentrates has not yet been published.
Case:
A 4-year-old female patient with type 3 VWD was referred to our hospital because of an anaphylactic reaction during FVIII/VWF concentrate (Immunate®) infusion. She had previously received FVIII/VWF concentrate (Haemate P®) infusions 8 times without any complications. She did not have antibodies against VWF and FVIII, and serum IgA level was normal. Since she needed factor replacement therapy as a result of a growing hematoma on her scalp, we performed skin prick and intradermal tests 2 days after the reaction. The prick test, with FVIII/VWF (Immunate), was negative, but the intradermal test was positive. We administered a 12-step desensitization protocol with FVIII/VWF concentrate (Immunate) successfully without any reactions.
Conclusion:
Anaphylactic reaction to factor replacement products is a major problem for patients with VWD, especially type 3 VWD requiring multiple factor infusions. We achieved a successful desensitization with FVIII/VWF concentrate in a patient who had an anaphylactic reaction during the infusion of this product. Our patient is important since she represents the first case of IgE-mediated anaphylaxis against VWF concentrate reported in the literature.
Introduction
Von Willebrand disease (VWD) is an autosomal recessive inherited disease caused by defects in the quantity or the quality of von Willebrand factor (VWF). 1 It is the most common hemostasis disorder, with a prevalence of ∼1 of 1000 subjects. 2 Type 3 VWD is the most severe form of VWF with undetectable VWF levels (<1 U/dL) and it affects 1:1 million live births.2,3 Patients with type 3 VWD have severe mucosal bleeding and also musculoskeletal bleeding, like hemophilia, and require multiple factor replacement products.
There are several VWF replacement products that can be used in the treatment of acute bleeding episodes or as prophylaxis. Unfortunately, 5.8%–9.5% of the patients develop alloantibodies (commonly polyclonal IgG) against these products. 4 These antibodies are called “inhibitors.” Patients who receive multiple transfusions and who carry large deletions have an increased risk of developing inhibitors.5,6 These antibodies can lead to life-threatening anaphylactic reactions as a result of immune complex-mediated activation of the complement system.7–10 Previous studies have suggested immune complex formation and complement activation as anaphylaxis triggers in VWF concentrate-induced anaphylactic reactions.4,7 However, IgE-mediated mechanism in anaphylactic reactions to this factor concentrate has not yet been published.
Herein, we present a patient with type 3 VWD who developed an IgE-mediated anaphylactic reaction during plasma-derived FVIII/VWF concentrate infusion and completed a successful desensitization with FVIII/VWF concentrate.
Case Presentation
A 4-year-old female patient with type 3 VWD (3% VWF activity and 3% F8 activity) was referred to our hospital as a result of an anaphylactic reaction during FVIII/VWF concentrate (Immunate®) infusion. Medical history of the patient stated that she had suffered bleeding from the gums and scalp hematomas after minor traumas since aged 1 year. She was diagnosed with type 3 VWD when she was 3 years old. She had received plasma-derived FVIII/VWF concentrate (Haemate P®) infusions on 8 previous occasions due to prolonged bleeding and hematomas after minor traumas, so our pediatric hematology department planned to start prophylactic factor replacement therapy twice a week. During the first dose of the Immunate infusion at another hospital, generalized urticaria, angioedema of the lips and eyelids, hypotension, vomiting, and respiratory distress had developed. The infusion had been stopped immediately. After adrenaline administration, her vital signs had turned back to normal and she had been referred to our hospital. Her vital signs and physical examination revealed no pathology during her attendance at our hospital. The serum tryptase level was 2.47 IU/dL, but the blood sample was sent 8 h after the anaphylactic reaction. No inhibitor was detected, neither against VWF nor F8, and serum IgA level was normal. She had no prior allergic reaction to foods, vaccines, antimicrobial, or anesthetic drugs and no history of a familial allergic disease.
Since it was not possible to perform specific IgE test or any other in vitro tests, we decided to perform skin prick and intradermal tests with factor replacement products to define the mechanism, even if the interval between the reaction and tests was short. Recent recommendations suggest that skin tests can be performed immediately after a reaction but only positive skin tests should be taken into account. 11 We performed skin prick and intradermal tests with plasma-derived FVIII/VWF concentrate (Immunate) and plasma-derived FVIII concentrate (Hemofil M®) 2 days after the reaction. Skin prick tests were performed by pricking the skin percutaneously with a 1-mm metal lancet through the factor concentrates (1/1 dilution) and read 15 min later. After the skin prick tests were found to be negative, we performed intradermal tests by injecting 0.02–0.05 mL of each factor concentrate with 1/10 and 1/1 dilutions as Platt et al. 12 performed in their previous report despite using different brands. The reaction was considered positive since the initial wheal increased by 3 mm in diameter with 1/10 dilution and 4 mm with 1/1 dilution after 20 min, with a flare around 13 (Fig. 1). The prick and intradermal test results of the patient are shown in Table 1. We did not perform skin tests to healthy controls because of ethical considerations about the factor concentrates being plasma derived, so the intradermal test positivity might be a false positive reaction due to irritant effect. We administered FVIII/VWF concentrate (Immunate) with a 12-step desensitization protocol same as previously performed by Platt et al. 12 (Table 2). The total dose of FVIII/VWF concentrate (Immunate) was calculated as 30 IU/kg FVIII. Written informed consent was taken from the patients' parents before each procedure. An intravenous line was inserted, and premedication with pheniramine (1 mg/kg), methylprednisolone (1 mg/kg), and ranitidine (1 mg/kg) was administered intravenously 1 h before desensitization. The patient was monitored during the procedure. The protocol was completed without any reactions.
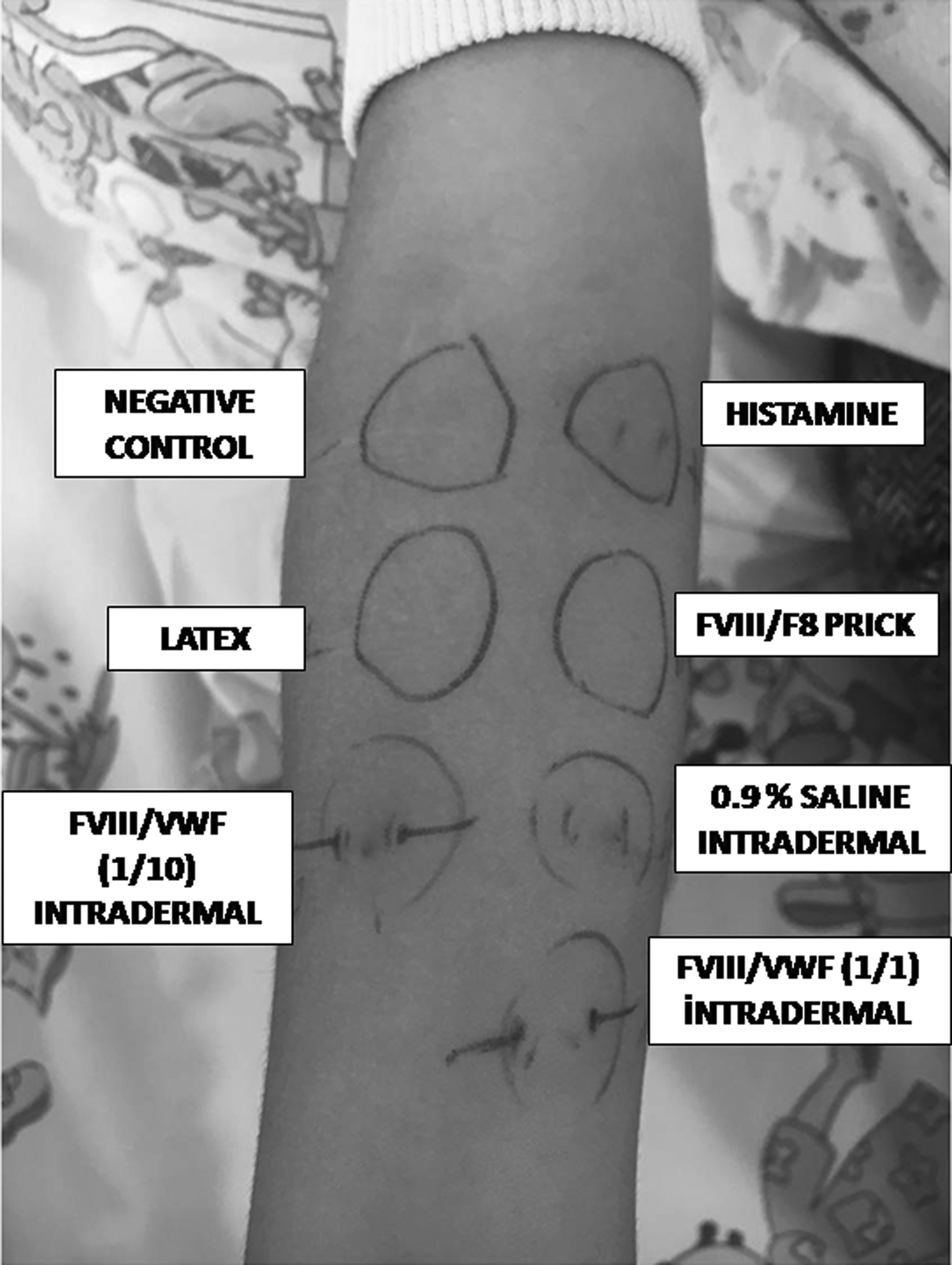
Skin prick and intradermal tests of the patient. Intradermal test with FVIII/VWF concentrate (Immunate®) was positive; the size of the initial wheal increased by 3 mm in diameter with 1/10 dilution (10 IU F8 + 7.5 IU VWF/1 mL) and 4 mm with 1/1 dilution (100 IU F8 + 75 IU VWF/1 mL) after 20 min with a flare around. FVIII, Factor VIII; VWF, von Willebrand factor.
Prick and Intradermal Test Results of the Patient
F8 concentrate 1/1 = 50 IU F8/1 mL. FVIII/VWF concentrate 1/1 = 100 IU F8 + 75 IU VWF/1 mL.
FVIII; VWF, von Willebrand factor.
Twelve-Step Desensitization Protocol with FVIII/VWF Concentrate (Immunate) 12
Discussion
We describe a case of type 3 VWD with IgE-mediated anaphylactic reaction to VWF concentrate. The low serum tryptase level in our case might be due to a delay in the blood sample collection; in contrast, a normal tryptase level does not rule out anaphylaxis. 14 The clinical findings of the patient were compatible with anaphylaxis, with generalized urticaria, angioedema, hypotension, vomiting, and respiratory distress. The positive early phase reaction in the intradermal test supported the IgE-mediated mechanism of anaphylactic reaction. Although we could not perform skin prick and intradermal tests with VWF concentrrate on controls and there is a possibility of having a false positive reaction, these test concentrations were not found positive in any patients and controls in a previous report by Platt et al. 12 From the patient's negative inhibitor status, we excluded the complement-mediated mechanism. As the factor concentrate was plasma derived, we also checked for selective IgA deficiency and found the patient's serum IgA level in a normal range. Although we could not make skin tests with the other components of the VWF/FVIII concentrate—such as albumin, glycine, sodium chloride, and calcium chloride—these components were found in both FVIII/VWF and FVIII concentrates. We excluded these components as a cause of anaphylactic reaction after the negative skin prick and intradermal tests with FVIII concentrate. Platt et al. 12 reported on 2 siblings with type 3 VWD that had an anaphylactic reaction during plasma-derived VWF replacement product infusions. Both patients showed anti-VWF antibodies. Skin prick and intradermal tests were performed with several plasma-derived FVIII/VWF products and recombinant FVIII products, as well as polysorbate 80, but no positivity was found. The researchers managed successful desensitization with a 12-step protocol. 12 Franchini et al. 15 reported anaphylactic reactions to both FVIII/VWF and recombinant FVIII concentrates in a patient with type 3 VWD. They did not perform skin tests. They found increased levels of anti-VWF antibodies and suggested them as the trigger of complement-mediated anaphylaxis in their patient.
IgE-mediated mechanisms in anaphylactic reactions have previously been reported in a small number of patients with hemophilia. Cugno et al. 16 reported a case with hemophilia B, featuring an anaphylactic reaction with recombinant FIX concentrate. They showed anti-FIX IgE and anti-FIX IgG antibodies together with LTC4 release after basophil activation with human recombinant FIX. Kadar et al. 17 reported that they found intradermal skin test positivity with purified and recombinant FVIII concentrates and found IgE and IgG antibodies against recombinant FVIII in a patient with severe hemophilia A and anaphylaxis. To the best of our knowledge, our patient is the first case confirming the IgE-mediated mechanism as the trigger of anaphylaxis against VWF.
Recombinant FVIII concentrates or recombinant FVIIa concentrates can be used in patients with previous anaphylactic reactions to VWF products. But their efficacy and safety are lacking.18,19 Franchini et al. 15 reported a case of anaphylaxis both with VWF and recombinant FVIII concentrate, and traces of VWF in the production process of recombinant FVIII have been hypothesized as being responsible for the reaction. Recombinant FVIIa concentrate is an alternative but a much more expensive therapy. Therefore, desensitization with VWF concentrate can be an effective option for these patients.
In conclusion, anaphylactic reactions to VWF products are important for patients with VWD, especially type 3 VWD, who have serious bleeding episodes requiring multiple factor infusions. Administering VWF products with desensitization is an effective and safe option. Our patient is important in that she is the first case of IgE-mediated anaphylaxis against VWF concentrate reported in the literature. Further studies investigating the best therapeutic approach for these patients, and the mechanism of anaphylaxis with factor concentrates, are needed.
Footnotes
Acknowledgments
We thank the parents of the patient for giving written consent for publication of this article.
Disclaimer
This work received no specific grant from any funding agency in the public, commercial, or no-for-profit sectors.
Author Disclosure Statement
No competing financial interests exist.