
Abstract
Background:
There have been varying reports on the prevalence of antineutrophil cytoplasmic antibodies with bactericidal/permeability-increasing protein (BPI-ANCA) specificity in cystic fibrosis (CF) patients. These autoantibodies are believed to develop in response to infection and colonization, especially with Pseudomonas aeruginosa. The aim of this review was to estimate the overall prevalence of BPI-ANCA in CF patients.
Methods:
We searched PubMed, Scopus, and Embase databases for studies reporting the prevalence of BPI-ANCA in CF patients. We also searched the Journal of Cystic Fibrosis and our institution's library for relevant studies on BPI-ANCA. We calculated the proportion with a 95% confidence interval (CI) to assess the prevalence of BPI-ANCA in the individual studies and then pooled the results using a random effects model. Publication bias was assessed using graphical and statistical methods. Finally, we assessed statistical heterogeneity using the I2 test.
Results:
Our search yielded 12 eligible studies published between 1996 and 2015. The prevalence of BPI-ANCA in patients with CF varied from 17.9% to 83% with a pooled prevalence of 49.45% (95% CI 35.53–63.42). No evidence of bias was found. However, there was evidence of statistically significant variation in the prevalence estimate due to heterogeneity (I2 = 93.4%, P < 0.01).
Conclusions:
Given the highly varying prevalence of BPI-ANCA in patients with CF, more well-designed prospective clinical studies are needed to determine its true prevalence and clinical relevance.
Introduction
Cystic fibrosis (CF) is a multisystem life-limiting autosomal recessive disease that primarily affects Caucasians. CF is caused by a mutation in the cystic fibrosis transmembrane conductance regulator (CFTR) gene on chromosome 7 that encodes for a chloride channel in the respiratory epithelium. According to the Cystic Fibrosis Foundation Registry, over 30,000 people in the United States are living with CF, and more than 1,000 new cases are diagnosed each year. Despite being a multisystem disorder, progressive deterioration of pulmonary function from chronic airway inflammation and infection, particularly with Pseudomonas aeruginosa, still remains the major cause of mortality and morbidity in patients with CF. 1 Several studies have reported a varying prevalence of antineutrophil cytoplasmic antibodies (ANCA) in CF patients, especially those with bactericidal /permeability-increasing protein (BPI) specificity.
BPI is an endotoxin-binding host protein with important antibacterial effects against Gram-negative bacteria, such as P. aeruginosa. It is a 55 kDa protein most abundantly found in the azurophilic granules of neutrophils. 2 BPI also acts as a target antigen for antineutrophil cytoplasmic autoantibodies. These antibodies have been identified in several diseases, including CF, inflammatory bowel diseases, vasculitis, rheumatoid arthritis, and primary sclerosing cholangitis and often develop in CF patients after colonization by more virulent strains of P. aeruginosa.3–6
During the last decade, several studies have reported varying prevalence rates of BPI-ANCA in CF patients and its link to a poor prognosis secondary to a progressive deterioration in lung function.3,6–9 The largest study reported by Carlsson et al. was a cross-sectional study of BPI-ANCA association with P. aeruginosa colonization and its effect on lung function in 366 CF patients (age: 0.5–55 years) and had a prevalence rate of 62.8%. 10 We systematically reviewed literature that provides information on the prevalence of BPI-ANCA in patients with CF to determine a more exact estimate of the frequency of this antibody in patients with CF.
Methods
Protocol and registration
The investigators structured this systematic review according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. 11 The study protocol was registered with PROSPERO (CRD42018090529).
Inclusion and exclusion criteria
We included studies that reported the prevalence of BPI-ANCA in CF patients. These studies needed to report whether or not the patients were colonized with P. aeruginosa.
We excluded the following studies: (1) editorials, case reports, and studies using nonhuman subjects; (2) studies describing the prevalence of BPI-ANCA in diseases other than CF; (3) studies that were done on non-CF patients. Figure 1 represents a flow diagram for identifying studies included in the meta-analysis.

Flow chart to illustrate the process by which articles were selected or rejected for inclusion in the study.
Search strategy
We searched PubMed, Scopus, and Embase databases (till February 2018) using the following free text terms: (“BPI” OR “bactericidal/permeability-increasing protein”) AND (“ANCA” OR “antineutrophil cytoplasmic antibodies”) AND (“CF” OR “cystic fibrosis”). See Supplementary Table S1 for search code and results. We reviewed the references for reviews and editorials on this topic. We also reviewed the references from the primary studies identified during the search. In addition, we searched the Journal of Cystic Fibrosis for any relevant studies, reviews, and abstracts. Finally, we searched our institution's libraries for any related studies or abstracts that might not be found online.
Study selection, data items, and collection process
The results collected from the database searches were compiled in a spreadsheet, and all duplicate citations were eliminated. The citations were first screened by the authors to capture the relevant studies. The full text of each citation was obtained and reviewed in detail. The following items were extracted: (1) publication details (title, authors, publication year, sample size, journal, country subjects were from); (2) age range of the study population; (3) prevalence of BPI-ANCA in patients with CF; (4) method of determining BPI-ANCA; (5) type of study; (6) report of P. aeruginosa colonization; (7) lung function test using Forced Expiratory Volume at one second (FEV1); and (8) study findings.
Assessment of risk of bias
The Newcastle–Ottawa Quality Assessment Scale (Fig. 2) measured the qualitative risk of bias by evaluating each study by these 3 categories: Selection, Comparability, and Outcome. Selection focused on the representativeness of the exposed cohort, the selection of the nonexposed cohort, the ascertainment of the specific exposure, and clear demonstrability that the outcome of interest was not present at the start of the study. Comparability was evaluated by the intrinsic design or analysis of each study through evaluation of study controls. The outcomes of each study were evaluated by the choice of assessment tool used for reporting the outcomes, if sufficient time was given to follow-up for outcomes to occur, and if an adequate number of the study population returned for follow-up.
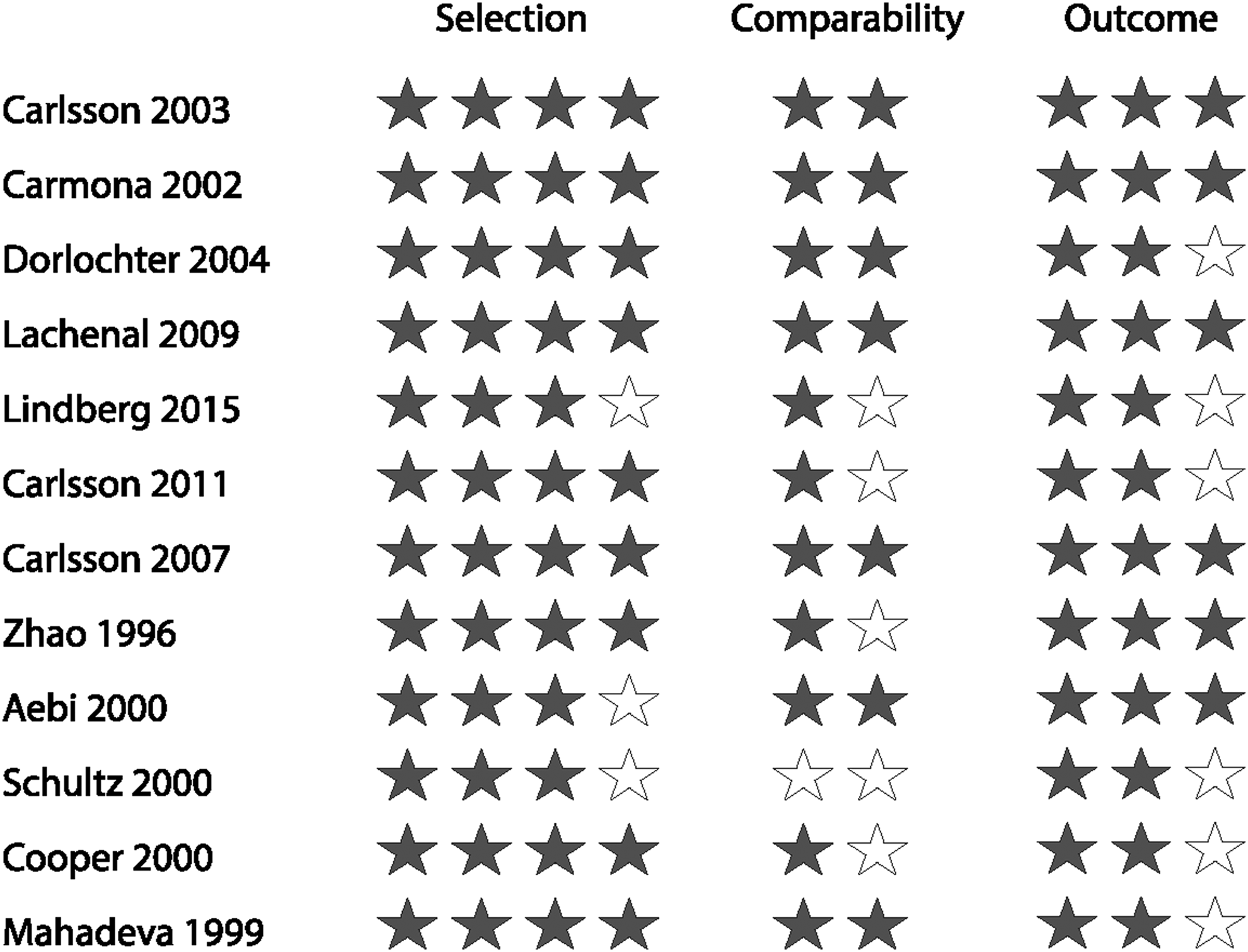
Newcastle–Ottawa Quality Assessment Scale for cohort studies.
Data analysis
We present the results of the systematic review both in table and narrative synthesis formats. Statistical analysis was performed on Stata 13.1 for Mac (StataCorp., College Station, TX). We used the developer .metaprop_one random ftt command to run a random effects meta-analysis of prevalence data, assuming that variation among studies was due to multiple random study characteristics, including countries where studies were conducted. 11
Freeman–Tukey double arcsine transformed proportions were calculated to stabilize variances and avoid estimates out of the 0 to 1 range. Computation of 95% confidence intervals (CIs) was done using exact binomial (Clopper–Pearson) method. 12 We calculated the pooled prevalence of BPI-ANCA in patients with CF. The impact of heterogeneity on the pooled estimates of the individual outcomes of the meta-analysis was assessed using the I2 test. Based on the suggested adjectives by Higgins et al., we interpreted the variation attributable to heterogeneity as low for I2 values between 25%–50%, moderate for 50%–75%, and high for ≥75%.
Analysis of publication bias
We assessed publication bias by visual inspection of asymmetry in funnel plots, which we plotted using developer metafunnel command. 13 We also carried out Begg and Mazumdar adjusted rank correlation test and Egger et al. regression asymmetry test for publication bias [Sterne] 13 using metabias command.
Results
Study characteristics
Our initial database search retrieved 31 citations, of which 12 were finally included in the systematic review (Fig. 1). All studies were published between 1996 and 2015. Reference country, sample size, age group, and main findings are summarized in Table 1.1,3,6–8,10,14–19 Most studies were from European nations. Seven studies included children. The age range was unknown in 3 studies.
Studies Describing the Prevalence of BPI-ANCA in Patients with Cystic Fibrosis
NR, all the positive patients had lung infections (most of them caused by P. aeruginosa).
BPI-ANCA, antineutrophil cytoplasmic antibodies with bactericidal/permeability-increasing protein; CF, cystic fibrosis; FEV1, forced expiratory volume at one second; FVC, forced vital capacity; HRCT, high-resolution computed tomography; NR, not reported; PFT, pulmonary function test; PMN, polymorphonuclear; ROS, reactive oxygen species; TNF, tumor necrosis factor.
Overall, the inclusion criteria and population characteristics of the analyzed studies were heterogeneous. Eight of the 11 studies reviewed included information on how BPI-ANCA was measured. All the reported testing techniques used indirect immunofluorescence for ANCA detection; enzyme-linked immunosorbent assay (ELISA) was used to test for BPI specificity. The patients who tested positive for BPI-ANCA were also reported to be colonized with P. aeruginosa.
Prevalence of BPI-ANCA in CF
The Carlsson studies focused on adults and children with CF in 2 Scandinavian countries and reported with BPI-ANCA prevalence rates of 71.7%, 62.5%, and 57.1%.7,10,14 All 3 studies reported colonization using 3 successive positive cultures and used ELISA for identification of BPI-ANCA isotypes. The first study used an ELISA upper level of 50 U/mL as the cutoff level; the other 2 studies used 67 U/mL as their cutoff level. Since BPI-ANCA is not normally found in serum, the authors used +3SD of the normal sera levels as their cutoff levels. The study published in 2007 included 366 patients from 2 CF centers in Sweden and Denmark and provided several important observations. 10 Positive serology for BPI-ANCA predicted a poor prognosis resulting in either lung transplantation or a significant loss in lung function. Serum levels of BPI-ANCA were higher in patients with reduced lung function (FEV1 below 50% of predicted) and Pseudomonas colonization. The frequency of Pseudomonas colonization, a positive BPI-ANCA test, and severe lung damage increased with age. In general, BPI-ANCA levels were stable over time but did decrease following lung transplantation. One study differed from the other 2 studies in that lung function was not measured, since the study specifically focused on the concentrations of interleukin (IL)-8 in A549 cell-stimulated supernatants. 14
The Lindberg study included patients from the Skane University Hospital CF center in Lund, Sweden. Bacterial colonization in respiratory secretions was defined by the Leeds criteria; the determination of antibodies against BPI was analyzed by ELISA. 3 However, the study did not report upper cutoff values for their ELISA technique. Thirty-one percent of the patients in this study were positive for BPI-ANCA.
The 2 United Kingdom studies were the Zhao and the Mahadeva studies. Zhao included only adults; Mahadeva did not mention the age of the patients.16,17 Zhao reported a BPI-ANCA prevalence of 83%, and Mahadeva reported a prevalence of 55.4%. P. aeruginosa colonization required 2 consecutive sputum cultures 6 months apart and a chest X-ray assessed by a CF physician using the northern system in the Mahadeva study. The Zhao study listed sputum collection for P. aeruginosa colonization. Both the Zhao and Mahadeva studies used ELISA for serology detection; Zhao did not list a cutoff level, and Mahadeva listed an optical density value >17% derived from a >3SD from mean value from a control population (n = 50).
The Schultz study included primarily pediatric patients from Germany. 18 Bacterial colonization was determined by sputum samples, and the presence of serum antibodies. ANCA was detected by immunofluorescence therapy and ELISA. No cutoff values were listed in the study; the BPI-ANCA prevalence rate was 59.3%.
The Carmona study in Spain included 56 adults and 49 children with BPI specificity tested by ELISA. However, antibody titer cutoff levels were not listed. They recorded a prevalence of 25.4%. 19 The Dorlochter study involved adults and children treated at the Haukeland University Hospital in Western Norway. 8 This study reported that a prevalence of 33%. P. aeruginosa colonization was verified by 2 or more antibodies against P. aeruginosa by ELISA and repetitive P. aeruginosa cultures within 6 months. ELISA for BPI-ANCA used the same methodology as the Carlsson group and was tested at the same laboratory (Wieslab AB, Lund, Sweden). Cutoff values for a positive test were 0.14 OD for IgA and 27 U/mL for IgG, based on +3SD of the normal sera levels as their cutoff point.
The Lachenal study involved adult patients treated at the CF center in Lyon, France. 1 Bacterial colonization was considered only positive after 3 consecutive positive sputum cultures. ANCA was screened by indirect immunofluorescence with a screen considered positive with >1 AU. These patients had a prevalence rate of 23.6%.
The Aebi study reported both pediatric and adult patients from the University Children's Hospital of Bern in Switzerland. 15 Bacterial colonization was determined by culture of respiratory secretion without clear description of handling procedures. BPI-ANCA antibodies was determined by ELISA with cutoff value of 4 IU/mL based on +3SD of normal sera levels. The BPI-ANCA prevalence in the Aebi study was 37%.
The Cooper study from Australia identified BPI-ANCA prevalence by ELISA by defining positive sera as greater than mean + 3SD of control population (n = 35). 6 The prevalence was recorded as 79%.
In summary, the prevalence of BPI-ANCA in patients with CF varied from 17.9% to 83.0% with a pooled prevalence of 49.45% (95% CI 35.53%–63.42%) (Fig. 3). There was no evidence of publication bias based on visual examination of the funnel plot (Fig. 4), and no significant bias was determined using statistical tests (Egger's test bias = 2.44, P = 0.124; Begg–Mazumdar Kendall's tau = 14, P = 0.373). Although the random pooled estimate was significantly different from zero (P < 0.01), there was high and statistically significant variation in the prevalence estimate due to heterogeneity (I 2 = 93.4%, P < 0.01).

Pooled prevalence of BPI-ANCA from the individual studies. The prevalence of BPI-ANCA in the individual studies is represented by a square (percentage) which runs a horizontal line (95% confidence interval [CI]). The diamond at the bottom represents the pooled prevalence from the studies. BPI-ANCA, antineutrophil cytoplasmic antibodies with bactericidal/permeability-increasing protein.
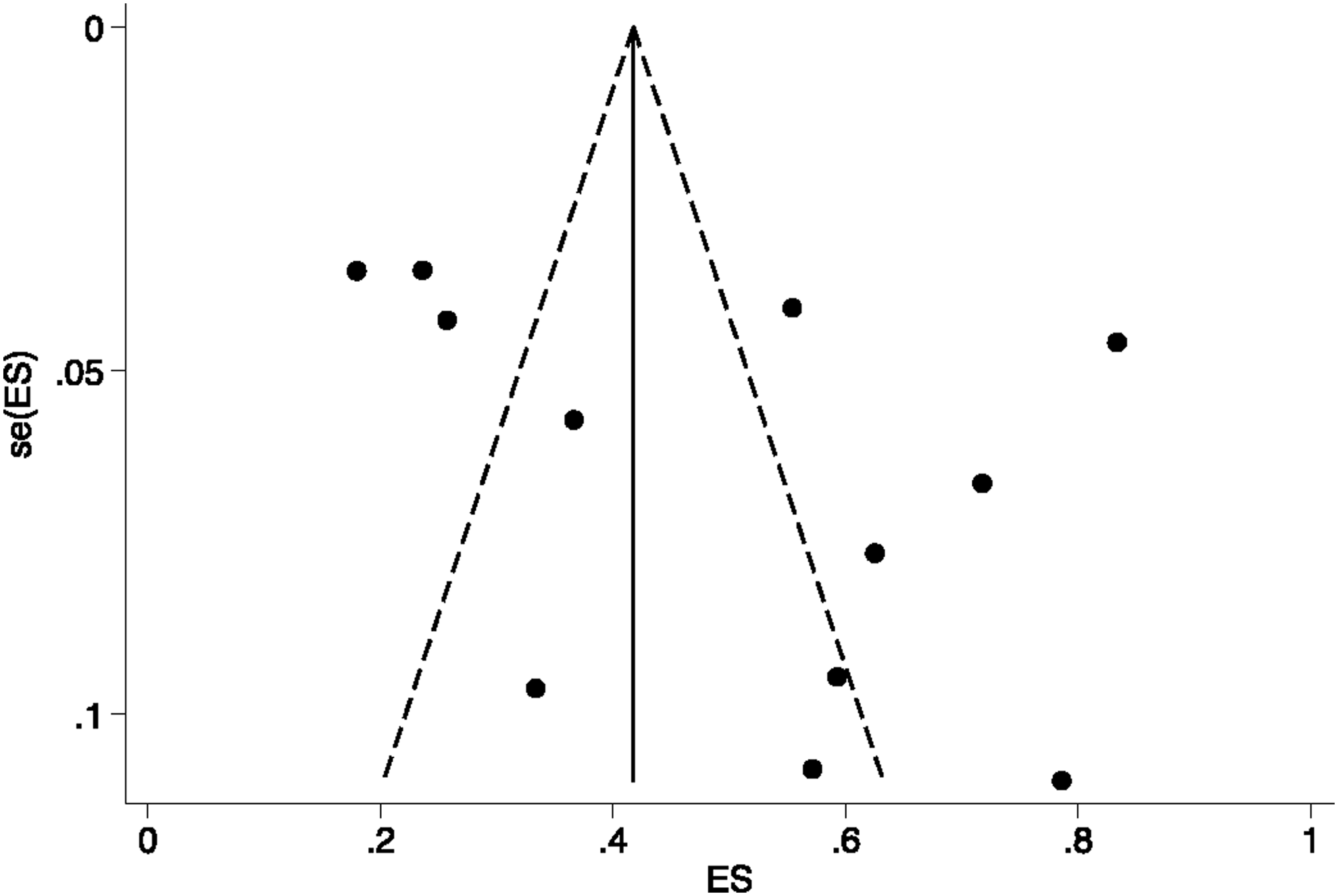
Funnel plots comparing the proportion versus the standard error of the proportion for the prevalence of BPI-ANCA in patients with cystic fibrosis.
Discussion
The purpose of this meta-analysis was to perform a systematic review of the prevalence rates of BPI-ANCA in CF patients. The current literature highlights studies from single and multicenter research groups, and this meta-analysis surveyed these individual studies to calculate a pooled prevalence rate and its statistical significance. Studies were assessed for their risk of bias; data analysis determined the pooled prevalence and the statistical variation of the study outcomes among the studies. Studies were also surveyed for differences in methodology, age range of patients studied, criteria for bacterial colonization, and cutoff values for positive ELISA tests. The results from this meta-analysis suggest a high and heterogeneous prevalence of BPI-ANCA with a median prevalence of 49.45 and a 95% confidence range of 35.53%–63.42% in patients with CF. We could not analyze the prevalence based on age since the majority of the studies did not report the BPI-ANCA status based on age. However, some of the studies showed a higher prevalence trend of BPI-ANCA in older patients colonized with P. aeruginosa.1,8,16
BPI is an endogenous antibiotic protein with potent killing activity against Gram-negative bacteria. This protein was initially identified in neutrophils; however, recent studies have reported its presence in epithelial lining of mucous membranes. Its antimicrobial activity occurs through both bacterial killing and binding to lipopolysaccharides produced by Gram-negative bacteria. Antibodies against BPI could decrease host defense responses in the lung parenchyma, slow bacterial clearance during infections, and increased lung injury. The studies we reviewed reported an association between P. aeruginosa colonization, high BPI-ANCA levels, and reduced lung function in CF patients. Most patients who were colonized with P. aeruginosa and were BPI-ANCA negative had preserved lung function. This observation supports the idea that BPI-ANCA may serve as a prognostic marker in patients with CF since chronic lung infections with deteriorating lung function are the main cause of death in these patients.1,7,10 Several investigators have studied the diagnostic significance of specific IgG antibodies to Pseudomonas in patients with CF and reported that elevated levels of specific anti-Pseudomonal antibodies are risk factors for developing chronic P. aeruginosa infection.3,20 For example, the odds ratios for positive antibodies against water-soluble antigens (St-Ag: 1–17) and exotoxin A for chronic Pseudomonas infections were 4.9 and 2.7 (both with a P < 0.05). 3 However, antibodies against Pseudomonas alkaline phosphatase, elastase, and exotoxin A correlate poorly with BPI-ANCA IgA levels. Antibody levels against BPI-ANCA identify patients chronically colonized with P aeruginosa and with FEV1s below 80% of predicted (area under the curve: 0.799) better than antibodies against these Pseudomonas proteins. 3
The possible role of BPI-ANCA as a biomarker for deteriorating lung function in patients with CF has led to studies using inhibitors against these antibodies. NEUPREX is a recombinant 21 kDa portion of the BPI molecule called rBPI21 developed by Xoma Ltd. (Berkeley, CA) and could competitively inhibit antibodies against BPI in patients. Levin et al. randomized 393 children with severe meningococcal sepsis in double-blind, placebo-controlled trial of rBPI21 and reported decreased morbidity (fewer amputations) in the children treated with rBPI21. 21 This protein has also been studied in small trials in patients with CF and lung infections. 22 To better understand the role of BPI-ANCA in CF patients who are colonized with P. aeruginosa, more studies need to focus on understanding the mechanism of this autoantibody in the production of disease.
Our study has several limitations. The significant clinical and statistical heterogeneity in these studies limits the confidence in the prevalence estimates. However, this clinical heterogeneity in the studies seems inevitable since the clinical information about autoimmunity and testing for BPI-ANCA in CF patients have evolved over the last decade. There were differences in data collection methodology as these centers had varying cutoff levels for BPI-ANCA-positive tests and different standards for defining positive bacterial colonization. Most of the reported studies came from Europe, potentially limiting the generalization of the estimated prevalence. In most developed countries, CF patients are cared for in specialized CF centers; therefore, the possibility of referral bias cannot be excluded in this study. When calculating the pooled prevalence of BPI-ANCA for studies reporting both IgA and IgG antibodies, we used the value for the IgA antibodies. This might have led to a slight underestimation of the true prevalence as IgG antibodies may contribute to the overall severity of autoimmunity in these patients.
In conclusion, we have systematically analyzed the prevalence of BPI-ANCA in CF patients. Future studies should adopt uniform testing procedures using multicenter heterogeneous patient populations, and the clinical significance of BPI-ANCA should also be investigated in a well-designed prospective study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.