
Abstract
Rationale:
Asthma is a common comorbid condition in sickle cell disease (SCD). However, obstructive lung disease is prevalent in SCD, independent of a diagnosis of asthma. It is speculated that the heightened state of inflammation in SCD, involving pathways distinct from allergic asthma, may underlie the SCD-specific obstructive disease.
Objective:
The objective of the study was to compare airway and systemic inflammatory markers between SCD patients with pulmonary manifestations and patients with allergic asthma, and correlate the discriminating inflammatory markers with clinical measures of pulmonary disease.
Materials and Methods:
In a pilot translational study conducted at the Children's Hospital at Montefiore, 15 patients with SCD, and history of asthma, airway obstruction, or airway hyper-reactivity, and 15 control patients with allergic asthma 6–21 years of age were recruited. Inflammatory markers, including peripheral blood T helper cell subsets, serum and exhaled breath condensate (EBC) cytokines and chemokines of the Th-1/Th-17, Th-2, and monocytic pathways, and serum cysteinyl leukotrienes B4 (LTB4), were quantified, compared between the study groups, and correlated with atopic sensitization, pulmonary function tests, and markers of hemolysis.
Results:
White blood cells (P < 0.05) and monocytes (P < 0.001) were elevated in the SCD group, while atopic characteristics were higher in the control asthma group. Tumor necrosis factor-alpha (P < 0.01), interferon gamma inducible protein (IP)-10 (P < 0.05), and interleukin-4 (P < 0.01) in serum and monocyte chemotactic protein (MCP)-1 in EBC were higher in the SCD group (P ≤ 0.05). Forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV1) in patients with SCD inversely correlated with serum IP-10 and LTB4 levels.
Conclusions:
Compared with atopic asthmatic patients, inflammatory markers involving Th-1, Th-2, and monocytic pathways were higher in the SCD group, among which Th-1 measures correlated with pulmonary function deficits.
Introduction
Sickle cell disease (SCD) affects 1 in 100,000 people in the United States, including 1 in every 365 African Americans and 1 in 16,300 Hispanic Americans. 1 Asthma is one of the most common comorbid conditions in SCD associated with increased risk of acute chest syndrome (ACS), respiratory symptoms, pain episodes, and death.2–8 While retrospective and cross-sectional studies have estimated asthma prevalence in 50% of children with SCD,2,6,9–11 data from large prospective cohorts of children with SCD report asthma prevalence rates of 17%–28%, similar to the general prevalence of asthma in the African American population (∼21%).4,12–14
There is a high prevalence of lower airway obstruction (up to 57%)15,16 and airway hyper-reactivity (up to 77%)15–19 in children with SCD, independent of a diagnosis of asthma. Furthermore, recurrent episodes of ACS are a leading cause of death in SCD, 20 but their effect on future pulmonary function is unclear. 21 Thus, SCD has a large pulmonary disease burden, possibly independent of asthma, with poorly understood pathophysiology.
There is increasing evidence on the role of leucocytes, neutrophils, and monocytes and their associated inflammatory markers in the pathophysiology of SCD-related complications,22–24 mechanisms that differ from classic allergic asthma that is associated with an eosinophilic Th-2-driven inflammatory response.
Murine studies suggest that SCD-related airway inflammation is distinct from allergic inflammation, with altered Th-2 and monocytic inflammatory profile observed in SCD models of allergen sensitization25,26 and a Th-1 predominant pathway found in an ischemia/reperfusion model. 27 There is also evidence for other interplaying mechanisms such as leukotriene production and hemolysis-induced decrease in NO production and arginine bioavailability.28,29 However, there is a dearth of human studies investigating these mechanisms of airway inflammation found in SCD murine studies.
To address this knowledge gap, in a pilot cross-sectional study, we compared systemic (blood and serum) and airway [exhaled breath condensate (EBC)] Th-1/Th-17, Th-2, and monocyte inflammatory markers in patients with SCD with pulmonary involvement with non-SCD control patients with classic allergic asthma. We also investigated the differences in the association of these inflammatory markers with clinical measures of atopy, airway involvement, and markers of hemolysis in the 2 study groups. We hypothesized that patients with SCD and pulmonary disease have an immune/inflammatory phenotype that differs from classic allergic asthma and is associated with clinical disease burden.
Materials and Methods
Study population
Fifteen patients with SCD, ages 6–21 years with HbSS or HbSβ0 thalassemia disease, physician-diagnosed asthma, positive screening on an asthma questionnaire (using a standardized ISAAC questionnaire, Supplementary Data), or with abnormal pulmonary function such as obstructive or restrictive defect or airway hyper-reactivity were enrolled between July 2016 and April 2018 from the Sickle Cell or Pulmonary Clinics at Children's Hospital at Montefiore (CHAM), the teaching hospital at Albert Einstein College of Medicine.
Fifteen nonobese children without SCD and with allergic asthma, ages 6–21 years, were recruited as controls. As this was a pilot study, we were unable to include a group of SCD patients without any pulmonary manifestations as an additional comparison group. In the SCD group, patients with recent episodes of ACS or blood transfusion within the previous 1 month, pain crisis requiring emergency room visits or hospitalization in the previous 1 month, or with pain crises managed by self-administered opioid analgesics in the preceding 2 weeks, or after stem cell transplant were excluded. Patients with neurological or cognitive impairment, coexistent autoimmune diseases, systemic diseases, recent pneumothorax, thoracic, abdominal, or eye surgery, those unable to perform pulmonary function tests (PFTs), or pregnant were excluded. The study was approved by the Institutional Review Board at Montefiore Medical Center and Albert Einstein College of Medicine.
Study procedures
All participants completed a study questionnaire querying demographic and clinical information, which was used for characterization of disease severity. Other clinical data were abstracted from medical records. Blood was collected on the day of recruitment for peripheral blood mononuclear cells (PBMCs) and serum separation. Vitamin D level and atopic sensitization (skin prick test or radioallosorbent test positivity to 1 or more common northeast allergens, including birch, Dermatophagoides farinae, cat dander, dog dander, Timothy grass, cockroach, goose feathers, Alternaria, Penicillium notatum, Cladosporium herbarum, Aspergillus fumigatus, oak, maple, common ragweed, and English plantain) were quantified for all participants and baseline hemolytic markers were obtained for SCD patients.
EBC was collected using the R tube® (Respiratory Research, Inc., Charlottesville, VA). Patients performed regular tidal volume breathing for 20 min while breathing into the tubes. The samples were immediately frozen using dry ice and stored at −80°C until analysis.
Pulmonary function tests
PFTs were performed in accordance with the American Thoracic Society guidelines30,31 at the PFT Laboratory at CHAM or results of recently performed PFTs (within previous 6 months) were abstracted from medical records. Spirometry (with postbronchodilator testing following treatment with nebulized albuterol), lung volumes, and diffusing capacity of the lung for carbon monoxide (DLCO) using CareFusion Vmax Encore 229C E spirometer and CareFusion Vmax Autobox 62 J body plethysmography were included in the analysis. Fractional exhaled nitric oxide (FeNO) was quantified as per published ATS/ERS guidelines 32 using the NiOx Vero. Further details are provided in the Supplementary Data. All patients completed spirometry. Lung volumes (n = 23), DLCO (n = 18), bronchodilator response (n = 22), and FeNO (n = 18) were completed by a subset of participants.
Flow cytometric analysis of PBMCs for quantification of Th cell subsets and monocytes
PBMCs were separated from heparinized whole blood following red cell lysis using lysis buffer (Thermo Fisher Scientific, Waltham, MA) within 24 h of collection and PBMCs were stored in liquid nitrogen until batched analysis. Additional details are in the Supplementary Data. Percent Th-1 (CD4+IFN-γ+ or CD4+TNF+), Th-2 (CD4+IL-4+ or CD4+IL-13+), and Th-17 (CD4+IL-17+) cells and monocytes (CD14, CD16) were quantified on the LSRII Flow cytometer (Becton Dickinson, San Jose, CA) and were analyzed on FlowJo software (FLOWJO, LLC). Analysis of a representative sample is shown in Supplementary Fig. S1.
Quantification of cytokines and chemokines in serum and EBC
Cytokines, including those associated with Th-1/Th-17 inflammation [interferon gamma (IFN-γ), tumor necrosis factor (TNF), interleukin (IL)-2, IL-8, IL-17, IFN-γ inducible protein (IP)-10], Th-2 inflammation (IL-4, IL-5, IL-9, IL-13), and monocyte activation [monocyte chemotactic protein (MCP)-1 and IL-6], were quantified in serum and EBC using the Luminex multiplex technology (EMD Millipore, Burlington, MA). Detailed methods are provided in the Supplementary Data.
Serum cysteinyl leukotriene B4
Leukotriene B4 (LTB4) was measured in serum using a competitive enzyme immunoassay through which serum was combined with an LTB4 binding antibody, and subsequently incubated with a secondary antibody, to determine the amount of bound enzyme activity. Samples (50 μL) were run in duplicate and the optical density of the color generated was measured at 450 nm using an EnSpire 2300 by Perkin Elmer to determine the amount of LTB4 bound in pg/mL.
Statistical analyses
All statistical analyses were performed on STATA v.14. Demographic and clinical variables and inflammatory markers were compared between the study groups using Student's t-test for data with normal distribution, or its nonparametric equivalent, Mann–Whitney test. Statistical significance was set a priori at α = 0.05. Results for serum cytokines, leukotrienes, EBC cytokines/chemokines, and Th cell and monocyte subsets were log10 transformed before analysis given their skewed distribution; log transformation of results lower than 1 resulted in negative values. Correlation analysis was performed using Pearson or Spearman tests for parametric and nonparametric data, respectively.
Results
Demographic and clinical characteristics
Demographic and clinical characteristics of the 2 study groups are shown in Table 1. The 2 groups were similar in age, gender, and ethnicity. Patients with SCD had experienced at least 1 episode of ACS in their lifetime. Atopic characteristics were more prevalent in the allergic asthma group, with more children having eczema (P < 0.0001), allergic rhinitis (P < 0.0001), family history of asthma (P < 0.05), and allergic sensitization (P < 0.01). The asthmatic group had higher eosinophil counts (5.5 ± 3.8 versus 2.7 ± 2.1; P < 0.05) and mean immunoglobulin E (IgE) levels compared with the SCD group, although both groups had elevated IgE levels (894 ± 869.8 versus 240.3 ± 453.6; P < 0.01). The SCD group had more emergency department visits (P < 0.05) and hospital admissions (P = 0.05) in the preceding 12 months. White blood cells (WBCs) and monocytes were higher in the SCD group (11.5 ± 2.0 versus 8.7 ± 3.9; P < 0.05, 12 ± 2.5 versus 7.1 ± 2.6; P < 0.001).
Demographic and Clinical Characteristics
Bold italic represents statistical significance.
BMI, body mass index; ED, emergency department; IgE, immunoglobulin E; SD, standard deviation; WBC, white blood cell.
Additional disease characteristics of the SCD group are summarized in Supplementary Table S1. Eighty percent of patients were on hydroxyurea. Polysomnograms had been previously done in 9 patients, 2 of whom had obstructive sleep apnea with hypoxemia and 3 others had nocturnal hypoxemia. All patients had had echocardiograms, which did not reveal evidence of pulmonary hypertension.
Pulmonary function tests
Results of PFTs and FeNO are shown in Fig. 1. Normal lung function was seen in 20% of patients with SCD and 13% of patients with asthma. Obstructive lung disease was present in 20% of the SCD and 60% of the asthma group. A restrictive pattern was seen in 47% of SCD (percent-predicted total lung capacity (TLC) SCD versus asthma, 76.1 ± 7.7 versus 92.7 ± 11.4; P < 0.001). A mixed obstructive and restrictive pattern was noted in another 13% of SCD patients. The asthma group had more air trapping and hyperinflation [percent-predicted residual volume (RV), 113.6 ± 27.2 versus 71.1 ± 12.6; P < 0.0001, RV/TLC ratio, 28.6 ± 4.2 versus 22.7 ± 3.4; P < 0.01]; a trend toward more airway obstruction [forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio, 77.5 ± 8.6 versus 82.5 ± 7; P = 0.09]; and a trend toward elevated FeNO (43.2 ± 40.1 versus 16.4 ± 8.4; P = 0.07). Percent-predicted DLCO values were lower in the SCD group (75.2 ± 12.6 versus 91 ± 12.6; P < 0.05), however, DLCO adjusted for alveolar volume and hemoglobin (DLCO/VA adj) was higher in the SCD group (110.8 ± 20.0 versus 88.0 ± 7.7; P < 0.05). Bronchodilator reactivity was seen in 16% of tested patients with SCD and 30% of tested children with asthma.
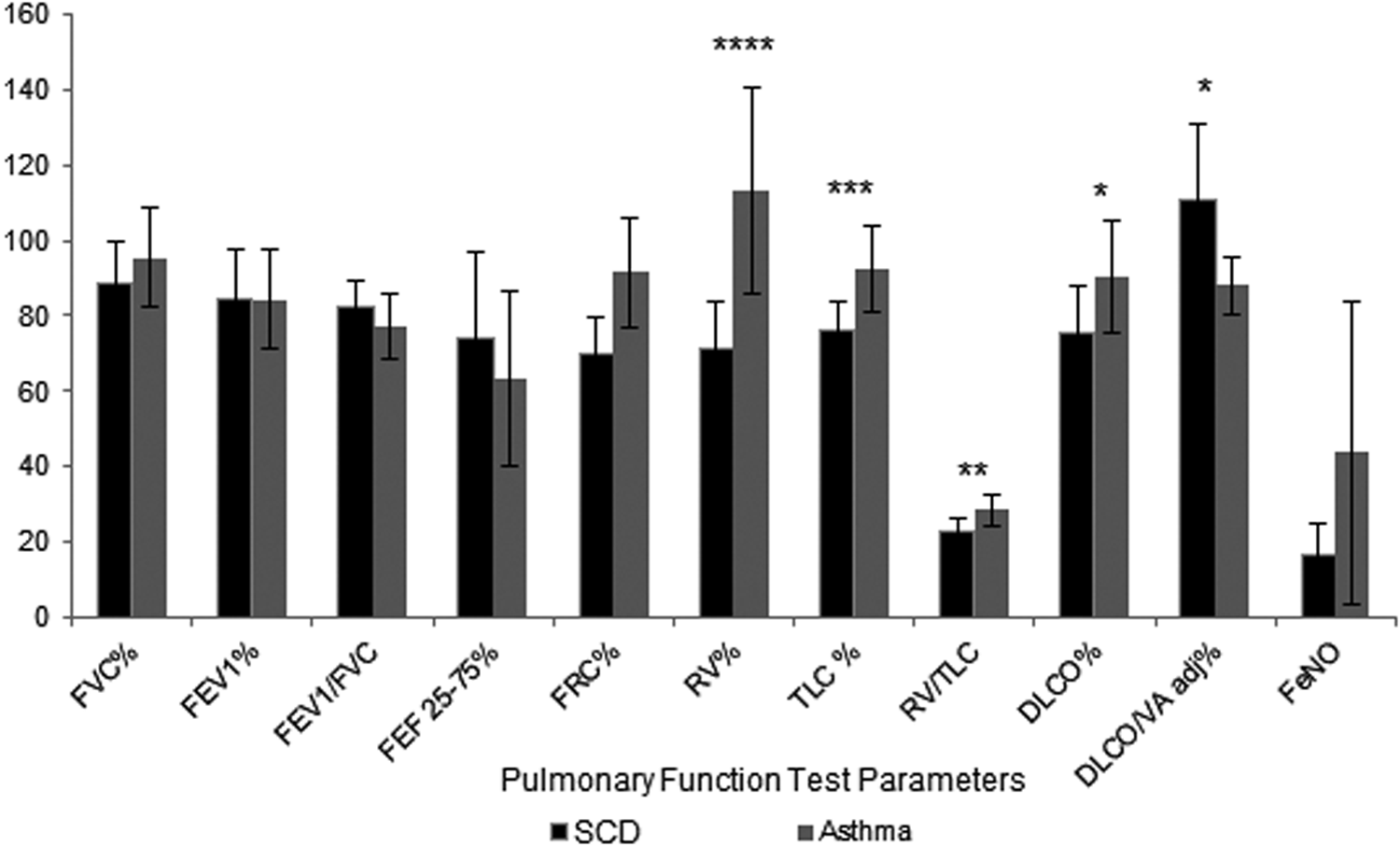
PFTs and FeNO in asthma and SCD groups. PFT parameters are reported as percent predicted and FeNO levels as ppb. Lung volumes (FRC, TLC, RV, RV/TLC)—12 SCD and 11 asthma patients. DLCO—11 SCD and 7 asthma patients. FeNO—10 SCD and 12 asthma patients. *P < 0.05; **P < 0.01; ***P < 0.001; ****P < 0.0001. DLCO, diffusing capacity of the lung for carbon monoxide; DLCO/VA adj, DLCO adjusted for alveolar volume and hemoglobin; FeNO, fractional exhaled nitric oxide; FEV1, forced expiratory volume in 1 s; FEV1/FVC, ratio of FEV1 and FVC; FEF25–75%, forced expiratory flow rate at 25%–75% of expiratory flow; FVC, forced vital capacity; PFT, pulmonary function test; RV/TLC, ratio of residual volume and total lung capacity; SCD, sickle cell disease; SD, standard deviation.
Serum and EBC cytokines, chemokines, and leukotrienes
Several serum cytokines, including particularly, TNF (0.70 ± 0.28 versus 0.52 ± 0.01 pg/mL; P < 0.01), IP-10 (2.41 ± 0.25 versus 2.20 ± 0.20 pg/mL; P < 0.05), and IL-4 (0.45 ± 0.91 versus −0.68 ± 0.90 pg/mL; P < 0.01), were elevated in the SCD compared with the asthma group (Fig. 2). Although most cytokines were below detection limits in the EBC samples, MCP-1 was detected in 15 SCD and 13 asthmatic samples with elevated levels observed in the SCD group (−0.06 ± 0.19 versus −0.16 ± 0.07 pg/mL; P < 0.05) compared with the asthma group.

Serum and EBC cytokines, chemokines, and leukotrienes in asthma and SCD groups. Serum and EBC cytokines and chemokines were measured using LUMINEX and results were reported in pg/mL. Serum LTB4 was measured using ELISA and results reported in pg/mL. All values were log transformed. *P < 0.05; **P < 0.01. EBC, exhaled breath condensate; IFN-γ, interferon gamma; IL, interleukin; IP, IFN-γ inducible protein; LTB4, leukotriene B4; MCP, monocyte chemotactic protein; SCD, sickle cell disease; TNF, tumor necrosis factor.
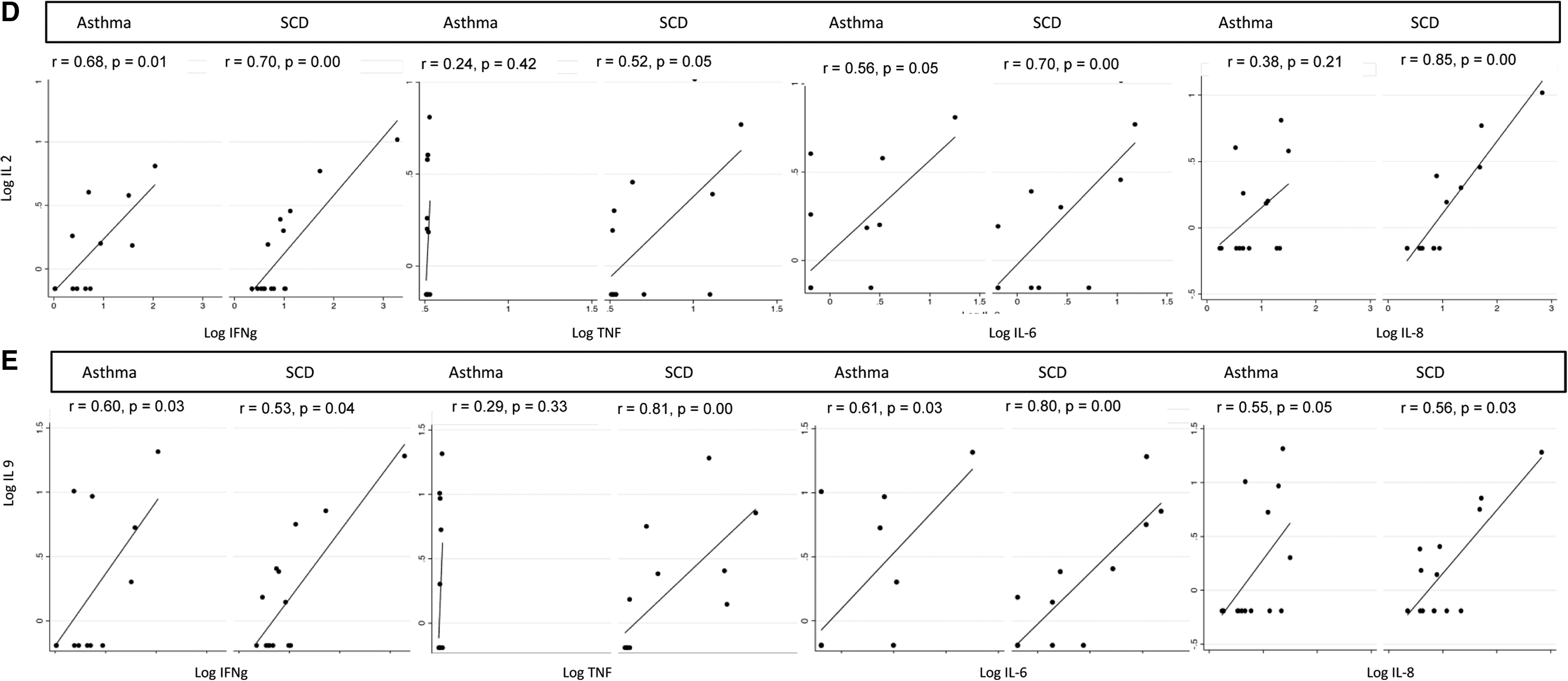
As shown in Fig. 3, serum MCP-1 trended to correlate with EBC MCP-1 in the SCD group (r = 0.46, P = 0.08), but not in the asthma group (r = 0.36, P = 0.23). Furthermore, in the SCD group, MCP-1 correlated significantly with TNF-α (r = 0.55, P = 0.04) and trended toward correlation with IFN-γ (r = 0.5, P = 0.06), IL-6 (r = 0.45, P = 0.09), and IL-8 (r = 0.45, P = 0.09), while there was a negative correlation between these parameters for the asthma group. Uniquely in the SCD group, TNF-α, IFN-γ, IL-6, and IL-8 correlated with IL-4 and IL-5 (Fig. 4A–E).

Correlation of serum MCP-1 with EBC MCP-1 in asthma and SCD groups. Serum and EBC MCP-1 levels were reported in pg/mL and values were log transformed. EBC, exhaled breath condensate; MCP, monocyte chemotactic protein; SCD, sickle cell disease.
Quantification of Th cell subsets and monocytes
Th cell subsets were quantified in 14 samples in each group, while monocytes were quantified in all 15 patients in each group. Differences in Th cell subsets and CD14+/CD16+ patrolling monocytes between the 2 groups did not reach statistical significance (Supplementary Table S2).
Association between systemic inflammatory measures and clinical parameters
Uniquely among the SCD group (Fig. 5A, B), FEV1 inversely correlated with IP-10 (r = −0.54, P = 0.04), while the inverse correlation of FVC with IP-10 approached statistical significance (r = −0.48, P = 0.07). A similar pattern was noted with LTB4 being inversely correlated with FEV1 (r = −0.49, P = 0.07) and FVC (r = −0.58, P = 0.02) in the SCD group. Markers of hemolysis (lactate dehydrogenase and reticulocyte counts) did not correlate with cytokines or PFT parameters. In the SCD group, monocytes quantified in WBC correlated with percent reticulocytes (r = 0.64, P = 0.01) and trended toward correlation with absolute reticulocyte count (r = 0.48, P = 0.07). There was no correlation between IgE and markers of hemolysis.

Correlation between cytokines and leukotrienes with lung function in SCD group.
Discussion
We quantified systemic inflammatory measures in patients with SCD and pulmonary disease and compared the findings with control patients with asthma to explore the pathophysiology of pulmonary involvement in SCD. Patients with SCD had elevated monocytes and TNF-α, IP-10, and Il-4 levels. Furthermore, TNF-α, IFN-γ, IL-4, Il-5, IL-6, IL-8, and MCP-1 levels trended to correlate with each other only in SCD patients. These patterns were partially replicated in the EBC analysis in the SCD group, which revealed elevated MCP-1 levels with trending correlation with serum MCP-1. PFTs showed a restrictive pattern with decreased DLCO but with elevated DLCO/VA adj in the SCD group, while airway obstruction, air trapping, and hyperinflation were more common in the non-SCD asthma control group. However, FEV1 and FVC were found to inversely correlate with IP-10, a Th-1 chemokine, and with LTB4, only in the SCD group. Together, our findings suggest higher systemic inflammation in the SCD group, including both monocytic and Th cell inflammation, compared with an age-matched allergic-asthma group. While there was no differential upregulation of atopic or nonatopic measures of inflammation, nonatopic inflammation correlated with pulmonary function in SCD.
Consistent with prior literature suggesting monocyte activation in SCD,33–36 monocytes and its chemokines were elevated in our SCD group, and airway levels of MCP-1 correlated with systemic levels. Since monocytes play a role in vaso-occlusion through several mechanisms, including endothelial activation, expression of tissue factor, formation of monocyte-platelet aggregates, and downregulation of endothelial NOS,33,35–37 we speculate that monocyte activation and release of its cytokines in the lung may be contributing to airway inflammation. Furthermore, endothelial cells can be activated in SCD and promote transmigration and activation of monocytes.35,38 IL-6 and IL-8 cytokines that tended to correlate in our study have been implicated in the monocyte procoagulant activity through tissue factor expression. 39 Our observation of higher serum levels of TNF-α and IL-6 and correlation between systemic MCP-1 and TNF-α, IFN-γ, IL-6, and IL-8 levels in patients with SCD further supports a role of monocytes in pulmonary disease in SCD, similar to findings by Belcher et al., 33 but they differ from those of Safaya et al., 36 which reported downregulation of NF-κB pathway and associated cytokines E-selectin, VCAM-1, ICAM-1, MCP-1, MMP-1, TNF-α, IL-6, and IL-1β, while incubating SCD monocytes with pulmonary artery and lung microvascular endothelial cells. Furthermore, we have reported on MCP-1 quantification in the airway emphasizing the importance of simultaneous investigation of the systemic and organ-specific compartments in well-characterized clinical cohorts to elucidate the pathophysiology of pulmonary disease in SCD.
Hemolysis of erythroid cells has been shown to activate monocytes via expression of TNF-α, IL-1β, IL-8, and MCP-1.40,41 The correlation of monocytosis with reticulocytes in our SCD group further supports the role of hemolysis in our patients. Moreover, studies have demonstrated augmented lipoxygenase pathways in monocytes in SCD resulting in increased leukotriene production that could mediate airway obstruction and airway hyper-responsiveness 42 via IL-13 and leukotriene pathways. 43 Although LTB4 did not differ between study groups in our study, unlike prior studies, 37 we did find an inverse correlation of LTB4 with FVC and FEV1 in the SCD group, further supporting its role in airway inflammation in SCD. These pilot results provide the framework to further investigate the overlap between systemic and airway inflammation responses and their distinct nature among patients with SCD with and without airway disease.
In keeping with mouse models of SCD with allergic sensitization showing an augmented and variable cytokine response with elevated Th-2 markers-Il-4, IL-5, and IL-13, as well as elevated TNF-α, IL-6, and MCP-1, 16 and other prior studies, 44 we also found elevated IgE in our patients with SCD and atopy, but not in those with SCD without atopy. Given our small sample size, we were unable to conduct further subgroup analysis among those with and without atopy to investigate the links between atopy and systemic inflammatory patterns in these children. Our findings and those of murine studies highlight this as an area that needs further exploration since ethnicities affected by SCD are also those that reside in urban environments and have higher prevalence of atopic asthma. 45
Invariant natural killer T (iNKT) cells, which bridge the innate and adaptive immunity, are another T cell subtype that produces IFN-γ, IL-2, and IL-4 and promotes activation of dendritic cells, natural killer cells, B cells, CD4+ (including Th-1 and Th-2 responses), and CD8+ T cells.27,46 These cells have been found to be activated in ischemia/reperfusion pulmonary injury mouse models as well as in patients with SCD and pulmonary disease, and can trigger a downstream inflammatory cascade contributing to pulmonary dysfunction.23,27 Although we did not quantify iNKT cells in our study, our findings of elevated IP-10 (an IFN-γ-induced protein), as well as IL-4 levels, and the correlation of IFN-γ with IL-2, IL-4, and IL-5 in the SCD group suggest that these cells may be key players in patients with SCD and pulmonary disease.
Similarly, neutrophils also play a substantial role in SCD inflammation through adhesion to endothelial cells and formation of neutrophil extracellular traps that trap circulating red blood cells and promote vaso-occlusion. 23 Although we did not find a significant difference in the neutrophil counts between our SCD and control asthma groups, likely explained by the usage of hydroxyurea in 80% of our patients with SCD given its suppressive effect on neutrophils, we speculate that functional studies on neutrophils may identify distinct pathways.47,48 Similarly, we can only speculate on the impact of inhaled corticosteroid use among our study patients. Inhaled corticosteroids are known to reduce Th-2-related inflammatory markers in asthma. The use of inhaled steroids in adult patients with SCD without asthma has demonstrated reduced systemic inflammatory markers. 49 In our study, 8/15 SCD patients and 12/15 asthma patients were on inhaled corticosteroids and this may have affected our outcomes for some of the cytokines and chemokines. Given the small numbers, we were unable to perform a detailed analysis.
Several studies have investigated PFTs in SCD, with an obstructive defect seen more commonly in the pediatric age group and a restrictive defect in older adolescents and adults.50,51 In our study, the prevalence of restrictive disease (47%) was higher and closer to that in the adult population, 51 while the prevalence of obstructive lung disease (20%) was within the previously reported range. 16 Our high prevalence of restrictive lung disease could be due to our small sample size or a higher disease burden in our population. Although FEV1 did not differ between the 2 groups, the inverse correlation of FEV1 with IP-10 and trend with LTB4 only in the SCD group supports a link between systemic inflammatory measures and pulmonary function. We also observed low DLCO but elevated DLCO/VA, as has been previously reported in SCD and attributed to pulmonary vascular disease and restrictive pathology.51,52 Since DLCO/VA represents the carbon monoxide diffusing capacity per unit alveolar volume, 53 decreased DLCO due to low lung volumes can be associated with elevated KCO due to increased efficiency and increased capillary blood flow per unit volume (assuming no change in cardiac output). 53 These findings support the phenomenon of a hyperdynamic circulation in SCD patients leading to increased capillary blood volume and airway resistance.54,55
Not all children had bronchodilator response testing. Among those who did, we reported a finding of 16% of bronchodilator responsiveness among children with SCD and 30% among those with asthma. Airway hyper-responsiveness has been reported in SCD, 19% to 77%, patients in various studies using different types of bronchial challenges. 16 Finally, we found lower FeNO in our patients with SCD compared with those with asthma, validating previous studies.56,57 As hemolysis releases free hemoglobin and heme (that consumes NO), and arginase (that destroys L-arginine, a substrate for NO production), 28 our findings suggest that our patients with SCD may be having more hemolysis than those participants in prior studies with higher FeNO reported. 58 Simultaneous quantification of FeNO and markers of hemolysis in future studies will further clarify the role of FeNO as a measure of allergic airway inflammation relative to severity of disease in SCD.
Our study has investigated several inflammatory markers of systemic and airway inflammation between SCD and asthma patients, thus challenging the common notion that airway inflammation in SCD is secondary to asthma. Our findings support those of a previous study evaluating cytokine levels among children with SCD in Jamaica and England, which had demonstrated higher IL-4 levels and a Th-2 profile among Jamaican children who were also more likely to have asthma, but their SCD status and non-asthma status correlated with cytokine levels. 59 We have identified multiple elevated cytokines in our SCD group that are distinct from classic eosinophilic inflammation, and are suggestive of primarily monocytic, Th-1, and Th-2 cell-driven inflammation in patients with SCD and pulmonary involvement.
We acknowledge our study limitations due to a small sample size, and the need for validation in larger study populations. We were limited by the pilot nature of the study and did not have additional control groups of patients with SCD but no pulmonary disease and/or healthy controls. In light of our finding, the overlap and differences in inflammatory cytokines in patients with SCD with and without pulmonary manifestations need to be studied further for better understanding of the inflammatory processes specifically contributing to pulmonary manifestations. Although we identified distinct cytokine patterns in our study patients, our technical limitations with frozen blood sample processing led to inconclusive results on Th cell subsets and monocyte quantification. Future human studies investigating these cellular mechanisms can help to better delineate the underlying pathophysiology of pulmonary involvement in SCD, and elucidate the specific Th cell associated with the immune profiles observed in our study. Even though we attempted to quantify several airway cytokines, we were unable to successfully quantify most. As previously suggested, our limitations in detection of EBC cytokines could be due to EBC cytokine levels being close to assay detection limits, a limitation that may have been overcome by lyophilization and concentration of the sample. 60 The other limitation could have been our use of R-tubes for collections that can have variable results compared with other collection systems. 60
Overall, our findings, suggestive of a role of monocytes in pulmonary inflammation in SCD, open avenues for several therapeutic options in these patients. Elevated inflammatory profiles of Th1 and Th2 pathways need to be studied further for therapeutic implications. The current practice has been to associate most patients with SCD who have pulmonary involvement with asthma and manage them with standard asthma medications. With more insight into the underlying mechanisms of SCD pulmonary injury, future therapeutic targets could be directed toward more specific disease mechanisms. Our study thus provides a platform for new evidence and insights into airway inflammation in SCD and directions for future research of these basic pathophysiologic mechanisms and potential therapies.
Footnotes
Acknowledgments
The authors thank the following: Biomarker Analytic Research Core (BARC) and Einstein-Montefiore Biorepository, Albert Einstein College of Medicine; Flow Cytometry Core Facility, Albert Einstein College of Medicine; Clinical Research Center, Albert Einstein College of Medicine; HIV Mucosal Immunity Core, Albert Einstein College of Medicine.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The project described was supported, in part, by the National Center for Advancing Translational Sciences (NCATS), components of the National Institutes of Health (NIH), through CTSA grant numbers UL1TR001073, KL2TR001071, and TL1TR001072.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.