
Abstract
Background:
The parameters of lung sounds have been suggested as biomarkers of airway changes. Using a commercially available lung sound analyzer, we investigated the characteristics of the lung sounds in infants with acute respiratory infection (ARI).
Methods:
Infants with ARI who were 6 to 18 months of age were included in this study. The lung sound parameters, the ratio of the third area and fourth areas to the total area under the curve of the sound spectrum (A3/AT and B4/AT), and the ratio of power and frequency at 75% and 50% of the highest frequency of the power spectrum (RPF75 and RPF50) were evaluated. With an original Japanese questionnaire based on American Thoracic Society-Division of Lung Disease, the risk factors of asthma development in infants were examined.
Results:
One hundred ten infants with ARI and 248 infants in good health for comparison were included. All infants were completely analyzed, and then divided into 2 age groups for a stratification analysis (6–12 and 13–18 months). In the overall analysis, among infants with a history of wheezing, recurrent wheezing, allergy, and atopic dermatitis, the values of RPF50 of infants with ARI were significantly lower compared with those without ARI. In the 6- to 12-month-old group, the RPF50 values of atopy-positive infants with ARI were lower compared with those without ARI (P = 0.003).
Conclusions:
The lung sounds of the infants with asthma-developing risk factors were more affected by ARI than those of infants without risk factors. Analyzing the changes in the lung sounds induced by ARI may be useful for evaluating the characteristics of the airways in infants.
Introduction
The diagnosis and intervention should be made as early as possible in infants who are likely to develop asthma, as early action is associated with immeasurable benefits, such as significant treatment and patient education for the long-term improvement and remission of asthma. 1 However, the diagnosis of asthmatic children <5 years is difficult.2,3
Large-scale prospective research on risk factors for the development of asthma has been conducted.4,5 Infants with an atopic condition or other risk factors related to recurrent wheezing tend to develop childhood asthma. 4 Although some indices are utilized, 6 a more accurate criteria for diagnosing childhood asthma is required in the pediatric clinical field.
A lung sound analysis is a simple and safe technique for assessing bronchial changes. 7 Recently, novel methods of signal processing have been developed, and the extraction of information from lung sounds became accurate.8–10 According to previous reports, lung sounds are sensitive to airway changes. Even in infants, significant differences in the lung sound parameters are observed by airway narrowing.10,11 Furthermore, wheezing-like inaudible noises have been studied in children with asthma 12 and cough-variant asthma.13,14 Recently, a large-scale multicenter-prospective study was conducted using an analysis of inspired lung sounds. In infants participating in an infant health examination, statistical differences were noted in the parameters of lung sounds of the infants with atopy compared with those of the controls. 15
In this study, we focused on acute respiratory infection (ARI), which induces an unavoidable stress on respiratory tracts in infants. Using a new method of analyzing lung sounds that is less strongly affected by the age, stature, and lung function,10,11 the relationship between the risk factors related to asthma development and the parameters of the lung sound spectrum of infants with ARI were examined, and the results were compared with those of age-matched infants without ARI.
Patients and Methods
Study subjects
To avoid any influence of age or structure, we also determined that the age range of the subjects was 6–18 months. In a cross-sectional study of a prospective multi-institutional study (Diagnosis of Infantile Asthma Using Lung Sound Analysis; DIAL), 15 115 infants with ARI (median age, 8 months, boy:girl, 52:63) who attended a health checkup for infants at Isehara Municipal Clinic, Dokkyo Medical University, National Hospital Organization Yokohama Medical Center, Yamato Municipal Hospital, and Uchida Iin Y Child Clinic from January 1, 2012, to March 31, 2016, agreed to participate in this study. Informed consent to their participation in this study was obtained from all subjects. The criteria of exclusion were as follows: infants with severe diseases of heart, lung, and others, with a fever, and/or respiratory symptoms. 15 For a comparison, 248 age-matched infants who had been in good health in a previous study 15 were included.
In this report, “infants with ARI” referred to infants who had had an ARI within the past 7 days, and “infants in good health” means infants who had not had an ARI within the past 7 days. The presence of an ARI was judged by the guardians based on the existence of airway symptoms, such as nasal discharge, nasal congestion, moist cough, wheezing, and shortness of breath with or without a fever. 16 No subjects had received medication for long-term management before the test.
Study design
The assessments were performed in the presence of guardians, mainly their mothers. The lung sounds were collected when taking rest. The absence of wheezing and rales was confirmed based on auscultation by a pediatrician before lung sound collection.
Questionnaire
Based on American Thoracic Society-Division of Lung Disease, an original Japanese questionnaire 17 was used (Table 1). By Question 1, the history of ARI within 7 days of the visit was collected. The history of wheezing, the factors related with respiratory infection and atopy, which are recognized as asthma-development risk factors, was collected through subsequent questions.1,2 In this study, a domestic pet meant an animal with fur, cat, dog, or other animals. Positivity for passive smoking referred to living in the presence of 1 or more family members who smoked. Positivity for a family history of allergy referred to a family member within 2 degrees having a history of allergic diseases. 15
Original Questionnaire (Translated to English)
Lung sound analysis
A lung sound analysis was performed for all participants, as described previously.10,18,19 Lung sounds were collected in a quiet booth using a dedicated hand-held small microphone. The microphone was placed on the right upper anterior chest at the second intercostal space on the mid-clavicular line. Lung sounds at inspiration were analyzed using a sound spectrometer (LSA-2000; Kenz Medico Co., Saitama, Japan).10,18
The recorded sounds were analyzed according to a fast Fourier transformation. The sampling frequency was 10,240 Hz. The spectra were obtained using a Hanning window. The sounds were displayed as a spectrograph. The dBm values were plotted on the Y-axis, and the Hz values were plotted on the X-axis. To analyze the power spectrum images, the zero point of the Y axis (0 dB) was decided based on the mean of the background noise, and was considered to be −90.0 dBm in this report.10,18
The point of the maximum frequency (Hz) in the shape during inspiration was used for the sound spectrum analysis. The third area under the curve (A3), fourth area under the curve (B4), and total area under the curve of 100 Hz to the highest frequency of the dBm power spectrum (AT) were conventionally calculated according to the Hz and dBm [1 arbitrary unit (dBm·Hz) on a spectrum curve]. The A3/AT, B4/AT, RPF75, and RPF50 were calculated by a conventional method. A 5-point moving average was used as a smoothing technique for the slope of the sound spectra.10,18
Three lung sound samples from among >10 samples were obtained. In each institute, 2 or more licensed pediatricians discussed the selection of sound samples with the same-shaped sound spectrum and without noises for each individual. 15 After the point of the maximum frequency was determined, personal lung sounds were automatically calculated using an in-house calculation software program.15,19 The median value from 3 samples was calculated for each subject.
Statistical analyses
The statistical analyses were performed using the SPSS software program (IBM SPSS Statistics, Version 22 for Windows; IBM Corp., Armonk, NY). Wilcoxon's signed-rank test was used to compare 2 samples. Bonferroni's correction was used for multiple comparisons, and the level of statistical significance was set at P < 0.025 (0.05/2 = 0.025). A Fisher's exact test was used for the test of independence.
Ethics
Written informed consent was obtained from their guardians, and the study protocol was approved by the Institutional Review Board of Tokai University Hospital (No. 11R-158, approval date; December 21, 2011).
Results
The lung sound analysis
One hundred ten of the 115 subjects with ARI within the past 7 days at the first visit (95.7%) successfully did a lung sound testing (Table 2). Five infants did not participate through the final respiratory sound analysis due to crying or restlessness. In these 110 subjects (range, 6–18 months; mean age, 8 months, male:female, 50:60), none of the lung sound spectrograms showed outside noises. For a comparison, we analyzed the 248 infants (range, 6–18 months; mean age, 8 months, male:female, 117:131) who had no history of ARI within the past 7 days. 15
Characteristics of the Study Population With and Without Acute Respiratory Infection
P value, Mann–Whitney U test.
From the DIAL study (Ref. 15).
Median (first quartile, third quartile).
Positive response to Question 2, 3, or 5
Positive response to Question 10 or 11.
ARI, acute respiratory infection; DIAL, Diagnosis of Infantile Asthma Using Lung Sound Analysis; RSV, respiratory syncytial virus.
Differences in the lung sound parameters in each questionnaire item between the infants with and without an ARI
In the overall study population, among infants with a history of wheezing, recurrent wheezing, allergy, and atopic dermatitis, the values of RPF50 of the infants with ARI were significantly lower than those of infants without ARI (P = 0.009, 0.004, 0.001, and <0.001, respectively) (Fig. 1). Among the infants with a history of allergy, the RPF75 values of infants with ARI were also significantly lower than those of infants without ARI (P = 0.009, Table 3). The analysis of passive smoking, domestic pets, and air pollution did not show any statistically significant differences between the ARI-positive and ARI-negative groups (data not shown).
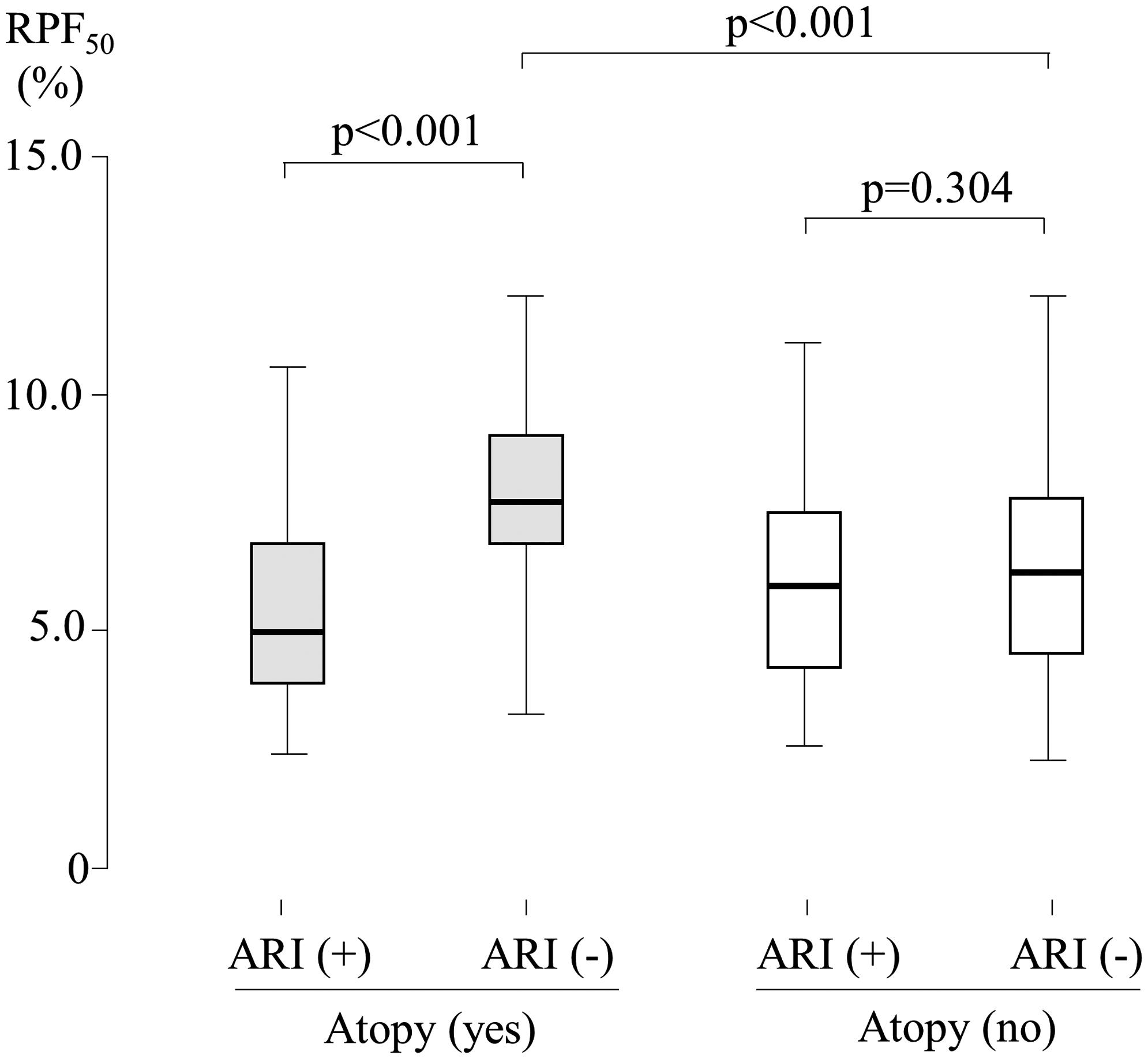
A comparison of the 4 groups of infants with or without atopy. The Mann–Whitney U test was used for these comparisons. In the positive-responding infants with atopy, the RPF50 value of those with ARI was significantly lower than in those without ARI. Among the infants without atopy, there were no significant differences in the RPF50 value between the infants with and without ARI. Among the infants without ARI, the RPF50 value in those with atopy was higher than in those without atopy. Atopy group: infants with positive responses for atopy-related items (Question 10 or 11). ARI, acute respiratory infection; RPF75 and RPF50, ratio of power and frequency at 75% and 50% of the highest frequency of the power spectrum.
Results of the Analysis of Parameters in the Breath Sound Spectrum in the Infants With and Without Acute Respiratory Infection
Bold letters represent values with a significant difference (P < 0.025).
P value, Mann–Whitney U test.
Atopy group, infants with positive responses for atopy-related items (Question 10 or 11).
Median (first quartile, third quartile).
A3, third area under the curve; ARI, acute respiratory infection; AT, total area under the curve of 100 Hz to the highest frequency of the dBm power spectrum; B4, fourth area under the curve; RPF50, ratio of power and frequency at 50% of the highest frequency of the dBm power spectrum; RPF75, ratio of power and frequency at 75% of the highest frequency of the dBmpower spectrum.
In Table 2, there was a significant difference in age between the infants with ARI and the infants without ARI (P < 0.001, Table 2). To avoid the effect of age, we divided the subjects with ARI into 2 age groups for a stratification analysis; 6–12 months (n = 58, median age, 7 months, male:female, 26:32) and 13–18 months (n = 52, median age, 18 months, male:female, 24:28). In the 2 groups, there was no difference in age between the infants with ARI and the infants without ARI. In the positive-responding infants with atopy in the group 6–12 months of age, the RPF50 values in those with ARI were significantly lower than in those without ARI (P = 0.003) (Table 4). In contrast, in the negative-responding infants with atopy in the group 6–12 months of age, the RPF50 values in those with ARI were not significantly different from the values in those without ARI. Other parameters showed no significant differences (data not shown). With no significant differences, the same tendency was seen in the group 13–18 months of age (Table 5).
Results of the Analysis of Parameters in the Lung Sound Spectrum in Infants 6–12 Months of Age With and Without Acute Respiratory Infection
Bold letters represent values with a significant difference (P < 0.025).
Median (first quartile, third quartile).
P value, Mann–Whitney U test.
ARI, acute respiratory infection.
Results of the Analysis of Parameters in the Lung Sound Spectrum in Infants 13–18 Months of Age With and Without Acute Respiratory Infection
Median (first quartile, third quartile).
P value, Mann–Whitney U test.
ARI, acute respiratory infection.
Differences between the infants with positive responses for Question 2–6 and those with positive responses for Question 10–12
To confirm the presence of any overlap between the infants with positive responses to wheezing-related items (Question 2, 3 or 5) and those with positive responses to atopy-related items (Question 10 or 11), we performed a Fisher's exact test. The numbers of infants with both wheezing and atopy, with wheezing and without atopy, without wheezing and with atopy, and without either wheezing or atopy were 7, 50, 55, and 286, respectively. The P value of Fisher's exact test was 0.494. There were no differences in spectrum curve indices between the infants with atopy and without wheezing and the infants without atopy and with wheezing (Data not shown).
Discussion
We have studied the usefulness of a lung sound analysis as a reliable, safe lung function test for infants and children.10,11,18 In our recent study, we reported the effects of risk factors of asthma development on the lung sound parameters in infants. 15 In that study, 95.7% of the participants were able to perform a lung sound analysis. These results show the suitability of a lung sound analysis for evaluating the lung function of infants.
To our knowledge, this is the first report to discuss the characteristics of lung sounds in infants with ARI. In this report, it is interesting that the values of spectrum curve indices, especially the RPF50 value in the infants with ARI, were significantly lower than those in the infants without ARI, when they had risk factors of atopy-related items (positive responses to Question 10 or 11). This tendency was not statistically seen in the infants without risk factors for asthma. Furthermore, in our previous report, the RPF50 value in the infants with risk factors of atopy-related items was statistically higher than those in infants without risk factors of atopy-related items when they did not have ARI. 15 We speculate that the lung sounds of the infants with the risk factors of asthma were more markedly affected by ARI than those of the infants without these risk factors.
We previously reported that the sound spectrum curve indices were decreased by bronchoconstriction with methacholine inhalation 18 and increased by bronchodilatation with β2 agonist inhalation. 19 The A3/AT and B4/AT values are the ratio of the higher frequency areas (A3 and B4) to the total area (AT) of the sound spectrum. The RPF75 and RPF50 indicate the angles of the high-frequency area of the sound spectrum. The RPF50 is more sensitive to the changes in the moderate-to-high-pitched sound areas than the RPF75. When bronchoconstriction is induced, the change mainly occurs in the high-frequency area of the sound spectrum.20,21 A prolonged high-frequency area with bronchial constriction resulted in decreases in the RPF75 and RPF50 values.10,18 The characteristics of infants with risk factors for asthma development may have already been present in this period, and we thought that some constriction of the airways in such infants might have easily been induced by inflammation with respiratory tract infection.
The ARI in this report was likely induced by respiratory viruses 22 and a natural stimulus of the airway in infants. Many reports have suggested the relationship between respiratory tract infections and recurrent wheezing and/or asthma development.23,24 In infants, ARI is popular and will likely be experienced many times over the course of a year. 25 Such events can be considered provocation tests in daily life that is not what they want. Indeed, the negative-response group showed a trend in which the spectrum curve indices among ARI-positive infants were slightly smaller than those in ARI-negative infants. Effective treatment and patient education requires understanding that some causative mechanisms of asthma are already present in infancy. Using a lung sound analysis, which can detect fine changes in airways,19,26 we may be able to diagnose asthma during these respiratory provocations early in life. However, such efforts will require available data on lung sounds with and without ARI for each individual subject.
Among infants with risk factors for asthma, 2 groups of this study—infants with wheezing (positive response to Question 2, 3, or 5) and infants with atopy (positive response to Question 10 or 11)—may have different pathologies. However, in lung sound analysis, the ARI induced the same reaction on the airways of both of these groups. This finding may underscore the clinical universality of their airways, such as their bronchial hyperresponsiveness. 27 We further speculated that this result indicates the presence of pathological phenotypes of wheezy infants and/or infantile asthma.
Among the infants without ARI, the RPF50 value in those with atopy were higher than in those without atopy. 15 This tendency may be due to the fact that the middle-pitched sound area in the lung sound spectrum was emphasized. Previous results suggest that, the middle-pitched lung sounds in healthy-state atopic infants were stronger than those in nonatopic infants.15,28 The high-frequency area of the inspired lung sound may have been induced by the peripheral bronchial narrowing,10,11 and some constriction near the central airways may produce a middle-pitched lung sound in them. However, it was not able to directly suggest the portion of the bronchi that caused the additional lung sounds. We will study this point in the near future.
In the present study, there were no marked differences in the spectrum curve indices when comparing with or without passive smoking (Question 13), domestic pets (Question 14), and air pollution (Question 15). Smoking in mothers is suggested to be harmful for infants.29,30 However, the effect of family smokers or pets with fur was clearly affected by background factors, familial economy, parents' education level, and other factors. 31 Sufficient and appropriate classification of participating families is required to examine the influence of certain factors on the lung sound analysis.
One of the limitations associated with this study was that it was not able to identify which virus or bacteria caused ARI. The major cause of ARI is likely a viral infection. 22 Since some viruses are known to be associated with asthma development in infants and children,32,33 it is meaningful to identify the causative viruses. This study was a multicenter, questionnaire-based, cross-sectional trial. In the next trial, we plan to check viral antigen. Another limitation was that we did not have correct data on the effect of aging on lung sounds in infants. In this report, as there was a clear difference in age between the infants with ARI and the infants without ARI, we examined both the data of the overall study population and a stratified analysis by age, which yielded similar results. We should collect more data on the lung sounds of individual subjects with and without ARI.
Conclusion
Our results clarify that the lung sounds of the infants with risk factors for asthma are clearly affected by ARI, 34 which may aid in the objective examination of bronchial reversibility. Of note, infants without risk factors for asthma showed no major influence of ARI on their airways. Our results seem to be convincing, as the infants with risk factors for asthma may have been predisposed in some manner with regard to bronchial hyperresponsiveness of their airways. Furthermore, the present findings suggest the usefulness of some common risk factors of asthma development. New diagnostic criteria of asthma-developing risk factors may be determined in combination with the ARI history and appropriate risk factors and lung sound data in the near future.
Footnotes
Author Disclosure Statement
S.I. reports grants from Chugai Pharmaceutical CO., LTD, Sanofi, Zenyaku Kogyo Company, Japan Blood Products Organization, Teijin, Maruho, Novartis, Mitsubishi Tanabe Pharma, Pfizer, and Astellas. H.F. reports grants from JSPS KAKENHI Grant Numbers 18K10013.
Funding Information
This study was supported by the Environmental Restoration and Conservation Agency of Japan in fiscal years 2009–2014 and 2015–2018.