
Abstract
Background:
Peanut introduction guidelines have undergone significant reversal since 2001 from recommending delayed introduction to rescinding the recommendations in 2008 to actively recommending early introduction of peanut between 4 and 11 months of age in high-risk infants in 2015. This qualitative study aims to explore pediatrician beliefs, practices, facilitators, and barriers regarding peanut introduction and testing.
Methods:
General pediatricians from academic, private, large group, and underserved practices in Northern California underwent individual semi-structured interviews in 2017. We asked about experiences surrounding infant peanut introduction, strategies for staying up-to-date with current recommendations, and barriers and facilitators to the new peanut introduction and testing recommendations. The data were coded, and using grounded theory methodology, a conceptual framework was developed around early peanut introduction and testing in infants.
Results:
Eighteen general pediatricians participated. We identified barriers that may contribute to pediatrician reluctance to recommending early peanut introduction or testing including lack of awareness, lack of agreement, lack of resources, and lack of outcome expectancy. A framework was created that suggests that pediatricians need to be knowledgeable about new recommendations, agree with the recommendations, have resources to carry out the counseling and testing, and have buy-in from the parents in order for successful uptake of peanut introduction guidelines.
Conclusion:
Recommending early peanut introduction or testing causes significant apprehension in some pediatricians, and there are many barriers to following recent early peanut introduction recommendations. A potential limitation of the study is that it was conducted right after the addendum guidelines were changed, leaving the possibility that attitudes and practices may have evolved since 2017. It is still likely that a multifaceted approach that addresses primary care provider guideline awareness, limited primary care resources for education and testing, and includes support and collaboration from subspecialty practices is more likely to lead to improved early peanut introduction uptake.
Introduction
Between 2000
In 2015, the Learning Early About Peanut (LEAP) study was published and was a randomized control trial of atopic infants that found that early peanut introduction between 4 and 11 months of age was beneficial: in infants with negative peanut skin tests, 13.7% of the group avoiding peanut and 1.9% of the early introduction group were peanut allergic at 5 years old, demonstrating an absolute risk reduction of 11.8%. 4 Subsequently, the AAP, the American Academy of Allergy, Asthma, and Immunology, and the American College of Allergy, Asthma and Immunology released a consensus communication to provide interim guidance before a full guideline was created. 5 The consensus communication recommended early introduction of peanut between 4 and 11 months of age to high-risk infants and suggested that those with severe eczema or egg allergy in the first 4–6 months of life may benefit from skin testing before introduction. In 2017, the National Institute of Allergy and Infectious Diseases sponsored an addendum guideline endorsed by the AAP that provided more detail to the recommendations and added an option for serum peanut IgE testing in high-risk infants before introduction and supported home or in office introduction in low-risk infants.
Although general pediatricians almost universally provide guidance on solid food introduction as it is a developmental stage that all infants and families encounter, few studies have explored general pediatrician views of new and important approaches to allergenic food introduction. Some small studies have found that only 11%–60% of pediatricians surveyed were adhering closely to the new peanut introduction and testing recommendations.6,7 To improve guideline uptake in primary care, a framework to approach interventions would be required to promote behavior change. Prior frameworks have hypothesized that physician knowledge, attitudes, and behaviors must be aligned with the guidelines for patient outcomes to change, but these frameworks are not specific to food allergy and may miss potential barriers to implementation of guidelines. 8 We utilized a qualitative approach to perform the first in-depth assessment of pediatrician beliefs, practices, barriers, and facilitators regarding early peanut introduction and peanut allergy testing.
Materials and Methods
Study population
General pediatricians in Northern California were recruited from the University of California, San Francisco (UCSF) database of referral centers and other practices identified through online searches. The sampling frame included more than 300 general pediatricians across the greater nine-county Bay Area. According to the American Academy of Allergy, Asthma, and Immunology, there are 81 allergists practicing in the area, demonstrating that access to allergists in this area is fair. Recruitment letters were mailed to 20 pediatricians at a time, and follow-up phone calls were made and e-mails were sent. Purposive sampling occurred to ensure that pediatricians from a variety of practice backgrounds including academic, large group, private, and federally qualified health center practices would be equally represented. 9 Recruitment and sampling continued until thematic saturation was reached.10,11
Study design
Grounded theory methodology was used to conduct this qualitative study using individual semi-structured interviews with pediatricians. 12 An interview guide (Supplementary Data) was developed in fall 2016 before the release of the 2017 addendum guidelines, which were not brought up by the interviewer. If participants brought up the addendum guidelines, they were probed about their viewpoints regarding the guidelines. The guide aimed to elicit narrative accounts from general pediatricians regarding beliefs and practices surrounding peanut introduction and allergy testing in infants, how they stay up-to-date with current recommendations, both generally and about food introduction practices, and barriers and facilitators to recommending peanut introduction or testing. Two preliminary interviews were performed, and the interview guide was revised for flow and content. Interviews were conducted either in person or over the phone by A.C., per participant preference between December 2016 and July 2017. Participants verbally consented to participation before initiation of the interview. The interviews were recorded and transcribed. Interviewers kept memos and field notes to provide contextual support of nonverbal cues. Participants were given a $50 gift card; to improve enrollment toward the end of the study, the last 4 participants received a $100 gift card. The study was approved for exemption by the University of California, San Francisco Institutional Review Board.
Data analysis
De-identified transcripts were entered into Dedoose 8.0 (Los Angeles, CA), a qualitative coding software. Four researchers (A.C., S.P., T.N.L., and M.O) coded the data. Qualitative analysis started with open coding by A.C. to develop the initial categories. Further analysis was performed and the categories were finalized by 2 investigators (A.C. and M.O.). Two investigators (S.P. and T.N.L.) then performed focused coding of all data and further developed the categories. Finally, 3 investigators (A.C., M.O., and M.D.C.) performed an iterative analysis to investigate subthemes and characterize specific topics to create a conceptual framework around peanut introduction in infants using grounded theory methodology.12,13
Results
A total of 18 general pediatricians from a variety of backgrounds participated in individual interviews (Table 1). A common theme for pediatricians who were aware of the early introduction and testing recommendations was that they felt uncomfortable with the recommendations and were not following them closely. They consistently identified barriers that fell into 4 major categories: lack of awareness, lack of agreement with the recommendations, lack of resources, and lack of outcome expectancy (Table 2). We describe the major categories and subcategories below.
Participant Data (n = 18)
Exemplary Quotes Regarding Barriers to Peanut Introduction and Testing
AAP, American Academy of Pediatrics.
Lack of awareness
While some providers were very familiar with the early introduction and testing recommendations, others were unaware of their existence. In general, pediatricians stated that they tried to stay up-to-date through both informal and formal continuing medical education methods. Formal methods of education include reading journals, attending society meetings or grand rounds, and referring to published practice guidelines. They also identified barriers to completing formal methods of education including lack of time to read or attend grand rounds as well as increased cost of attending society meetings. Informal methods of education included learning from colleagues, patients who are increasingly savvy and would mention new studies, local subspecialists, e-mail updates from professional societies, and popular media. Physicians in group practices stated that they often discussed new findings that they thought would alter their practice with their colleagues. Multiple pediatricians also stated that they expected pediatric professional society e-mails to highlight major medical changes.
When queried about peanut introduction studies and recommendations, multiple pediatricians stated that they rarely read the primary studies, instead relying on summaries to trickle down important information.
“I can't give you specific data. I mean to be honest, I can't tell you where they were published or anything because I'll just tend to read more through the newspaper version than the primary source.”
Lack of agreement
While some pediatricians stated that they would do their best to adhere as closely to the guidelines as possible, other pediatricians disagreed with testing recommendations, had concerns about pediatricians carrying out introductions in low-risk patients, and were cynical of yet another guideline change.
Concerns about testing
Some pediatricians who knew about the testing recommendations felt that testing high-risk infants was unnecessary. Some felt that infants, regardless of risk, should just be introduced to allergenic foods without adding an additional step of a priori testing.
“I'm not going to start somebody off on the blood test. If I want to know if the kid's got a response, then you have to do a food challenge.”
Concerns about carrying out supervised feedings
Pediatricians who were aware of the addendum guidelines expressed a lack of self-efficacy in regard to the recommendation that low-risk patients could undergo a supervised feeding at the pediatrician's office. They expressed fear of causing life-threatening anaphylactic reactions during allergenic food introduction. They felt particularly uncomfortable and untrained in introducing potentially allergenic foods in their office as prescribed by the guidelines. Furthermore, they expressed frustration that the allergy community had imposed this responsibility on them without having a plan in place to train pediatricians.
“They say ask your pediatrician to supervise giving a potentially life-threatening thing to your tiny infant. Give me a break. I would prefer that we don't get recommendations that put us in a bind. I feel like it came out a little prematurely before there was a plan of action from the allergists.”
Mistrust due to guideline changes
Another pediatrician barrier was frustration with and mistrust of the guidelines due to the multiple changes in guideline recommendations over the past 2 decades. They stated guilt over the fact that their past recommendations of delaying food introduction may have harmed children.
“You told me that I must wait to introduce allergenic foods, and all of a sudden, you're telling me that all along we're actually increasing the rate of allergies in children. It will always cause a little bit of cynicism.”
Lack of resources
Pediatricians cited allergists as important partners in successful uptake of allergenic food introduction recommendations for a number of reasons: the ability to provide skin testing and oral food challenges to high-risk patients, a better understanding of the studies that led to the creation of the recommendations.
Concerns about access to allergists
While the Northern California area had a good total number of allergists in the area, some pediatricians still felt that their patients had a difficult time getting an allergy appointment. They expressed concern that it may take many months before high-risk patients could see an allergist and result in delaying introduction, putting families in a paradoxical bind.
“By the time they have an [allergist] appointment, you wish they really tried the eggs. They will be 10 or 11 months by the time they see an allergist, and so that aspect is harder actually to carry out here.”
Need for specialty endorsement
Some pediatricians who wanted to carry out the recommendations still did not feel totally comfortable following them without the endorsement of local allergists. In particular, some felt discordance between guidelines from the World Health Organization and the AAP that endorse exclusive breastfeeding for the first 6 months with the new recommendations that encourage peanut introduction as early as 4 months.14,15 Pediatricians expressed that they needed to hedge between the guidelines that were in direct conflict with one another and preferred to have a local allergist weigh in on the recommendations. If pediatricians had not discussed the new recommendations with their trusted subspecialist colleagues, some felt more reluctant to carry out the recommendations.
“I think the new recommendation seems really radical. I would call an allergist and ask, ‘Are we sure that we need to do this?’ We will do whatever [they] tell us to do.”
Pediatricians also expressed frustration that it was not clear to them how much, how often, and how long patients should ingest peanut and felt unable to fully counsel on these issues. Pediatricians desired more educational materials for parents that were endorsed by allergy and pediatric societies that would explain the rationale behind the guidelines and provide specific directions to parents.
Practice-level barriers
Pediatricians who wanted to adhere to the recommendations expressed some systems barriers to executing the recommendations. Specifically, some noted a lack of time to effectively counsel about allergenic food introduction and felt that allergists were better poised to do so. They also cited that pediatricians were being asked to do more and more and that they did not have the time to do so.
“It is just crazy what's being asked of pediatricians. Every couple of months the AAP is coming out and saying, ‘You're supposed to include this, you're supposed to include that.’ Well, it is not possible.”
Some pediatricians felt that allergenic food introduction was a low priority topic due to the perception that food allergy was uncommon in their practice and did not think that early introduction would make a difference to their patients; they preferred to focus on other topics during the 4–6 month well-child visits. In particular, pediatricians in federally qualified health center practices felt that there were competing practice priorities that needed to be discussed during a short visit.
“They are worried about nutrition, food insecurity, housing insecurity, domestic violence, maternal depression. All those things can end up being much more priority than taking five to seven minutes to counsel about food introduction.”
Lack of outcome expectancy
The final major category of barriers that arose was due to pediatricians' views of parental fears about peanut introduction or allergy testing, either due to concerns that recommendations had changed from previous children or that parents did not feel comfortable with introducing peanut or their child undergoing testing.
Parental skepticism
Pediatricians expressed that for families who had older children that were advised to delay or not actively introduce allergenic food introduction, the new recommendations would cause skepticism and frustration on the part of the parents as recommendations have changed in a relatively short amount of time.
“It just seems like a big change, and especially if it's their second or third kid, they're like, ‘Wow we weren't able to do that until after their birthday, are you sure?’”
Parental fear of introduction or testing
Even if pediatricians did feel comfortable applying the new recommendations and counseling patients, many did not think it likely that such counseling would lead to parents agreeing to testing or carrying out peanut introduction. Multiple physicians stated that parents of high-risk infants have been fearful of and resistant to agree to skin or serum-specific IgE testing and preferred delaying peanut introduction rather than have their child undergo testing. In addition, after parents of low-risk infants have been counseled to introduce the allergenic food to their child, physicians have perceived that they are still not actually comfortable doing so. Multiple physicians expressed that parents were reporting that they were introducing foods in emergency room parking lots or on their way to the pediatrician's office due to concern that the allergenic food introduction would cause an allergic reaction.
Conceptual framework
Our analysis was based on the assumption that there were unique barriers and facilitators to physician uptake of peanut introduction and testing recommendations. These constructs were well aligned with a guideline framework developed by Cabana et al. 8 Our work was then able to generate a unique, peanut introduction focused framework to help guide future research, implementation efforts, and policy on promoting early peanut food introduction (Fig. 1). This framework illustrates that to improve pediatrician uptake of early peanut introduction, they need to be knowledgeable about the new recommendations, agree with the recommendations, have resources to carry out the counseling and testing, and have buy-in from the parents.
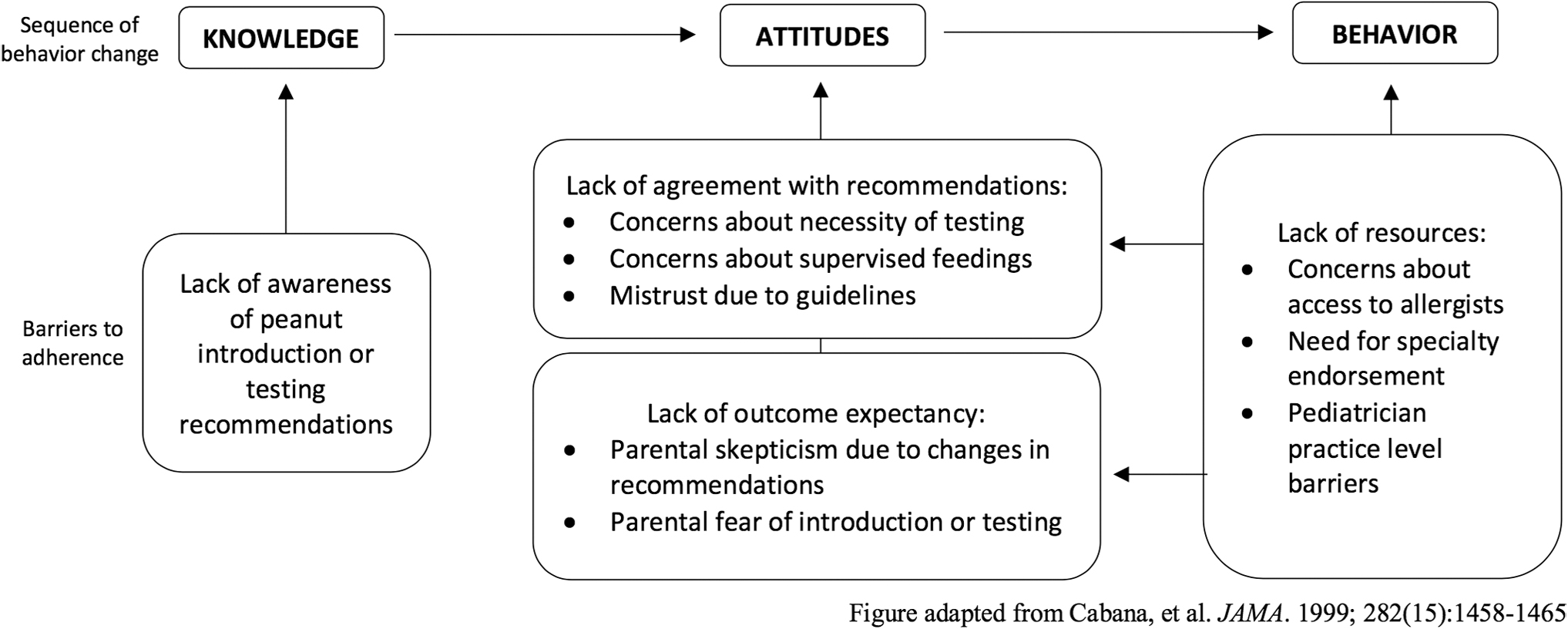
Barriers to physician adherence with peanut introduction/testing guidelines in relation to behavior change.
Discussion
The 180-degree change in guideline recommendations between 2000 and 2015 regarding allergenic food introduction provides a unique opportunity to examine how pediatricians apply such changes shortly after new recommendations are released. Our framework can be used to better understand of the barriers to practice change that can help expedite this process of allergenic food introduction. Specifically, it is important to address the knowledge and attitudes of physicians to improve early peanut introduction and testing recommendation uptake.
Consistent with previous studies, our framework hypothesizes that pediatricians' knowledge about food allergy and its management can be lacking despite the AAP trying to publicize the LEAP study findings and associated recommendations.16,17 Pediatricians expressed interest in understanding the evidence base supporting the guideline recommendations, as well as having resources to explain these recommendations to families. Improved guideline formatting may include succinct and specific clinical recommendations, as well as the descriptions of the clinical trial data supporting the recommendations. 18 Clinical support tools, patient education materials, and websites have been used to help support primary care practices to be more consistent with evidence-based guidelines. 19 Pediatricians were often unaware of resources included in the addendum guidelines that offered explicit instructions for pediatricians and parents to facilitate early peanut introduction. 15
Our framework also suggests that increasing stakeholder input in implementation of guidelines is critical, as manifested by pediatrician attitudes about the recommendations. Lack of agreement and lack of outcome expectancy were commonly expressed by the pediatricians. Pediatricians in this study expressed frustration that there has been so much change on recommendations for allergenic food introduction over their careers. They also felt that the recommendations were “unfunded mandates” where recommendations are made to providers, but supports were not provided by the health systems, AAP, or allergists to successfully carry out the recommendations. In addition, recent studies about parental willingness to carry out early peanut introduction or testing have demonstrated low support for the recommendations as well as low implementation rates. 20 Consistent with our framework, this would suggest that pediatricians require assistance to address parent perceptions, which often are barriers to carrying out the recommendations. 7 Potential interventions to assist pediatricians may be developing specific skills in counseling and motivational interviewing that can help improve patient adherence. 21 In addition to lecture-based continuing medical education, skills-based training has been useful in improving physician and nurse self-efficacy in counseling and education. 22
Our framework also reflects pediatricians concerns about lack of resources, a barrier to following the recommendations. Timely access to allergists is needed for high-risk infants and their parents to receive counseling, get skin testing, and undergo food challenges without delaying introduction. Pediatricians wanted affirmation from familiar local allergists to assure them that the new recommendations are worthwhile for them to implement, specifically in regard to the need for a priori testing as a risk stratification measure. Pediatricians also sought allergists to help reconcile differences between guidelines. Specifically, the World Health Organization and the AAP guidelines endorse exclusive breastfeeding until 6 months, but this is in conflict with the addendum guidelines that recommend allergenic food introduction as early as 4 months.
Potential methods to improve access include telemedicine, use of an allergy management support system for primary care, or allergist training of primary care pediatricians to enhance management skills.23,24 For example, webinars have been used to train community general pediatricians on the management of common food allergy-related scenarios. 25 To improve physician agreement with current guidelines, general pediatricians preferred use of local opinion leaders, such as local AAP chapters or other influential individuals in their community, and consistent endorsement by professional organizations to learn about new technologies, therapies, or approaches to care.26,27
Limitations
While this study is focused on uptake of early peanut introduction and testing recommendations following the 2015 LEAP study and consensus communication, the 2017 addendum guidelines added granularity, including options for skin testing and feedings. The addendum guidelines were released shortly after the development of the interview guide and after the pilot interviews had taken place. While they were brought up by some of the participants, the timing of the study likely affected familiarity and comfort with the recommendations. Some studies suggest that it may take up to 17 years for research to be widely adopted into clinical practice, but there is likely incremental change over shorter periods of time. 28 It is possible that pediatrician knowledge, attitudes, and behavior have also evolved since the time of the interview.
It is possible that not all themes and codes related to barriers to early peanut introduction were captured, although thematic saturation was reached. We sampled general pediatricians from various urban and suburban practice settings and training sites to bring a diverse lens to the topic area, but sampling was restricted to Northern California. Their experiences may not be fully representative of pediatricians' experience across other areas of the United States, including rural areas, where allergist access may be significantly less. Physicians stated that parents played a significant role in successful guideline uptake, as parental fear was believed to be a major barrier in guideline adoption. However, parents of atopic infants were not interviewed directly to confirm these beliefs.
Conclusion
We developed a framework to assist physicians, researchers, and policy makers in generating future approaches to improve uptake of peanut introduction guidelines to help decrease rates of peanut allergy in children. Based on our analysis, a single intervention to improve primary care use of peanut introduction guidelines is unlikely to be successful. Rather, any initiative to change current practice will need to be multifaceted. Interventions need to help pediatricians be more and comfortable with the recommendations and disseminate the rationale and evidence for current recommendations. Given the limited resources in primary care practices, any intervention may need to include enhanced partnership or support from allergists and pediatricians to offer more in-depth counseling to parents, skin testing, as well as support and facilities for performing observed feedings that promote early introduction. Finally, a primary care intervention could also be supported by parent educational materials that address parental fears about testing and concerns.
Footnotes
Author Disclosure Statement
Michael D. Cabana, MD, MPH, is a member of the United States Preventive Services Task Force (USPSTF). This article does not necessarily represent the views and policies of the USPSTF. No authors have any other personal, financial, or commercial associations that might create a conflict of interest in connection with the submitted article.
Funding Information
This work was supported by the Academic Pediatric Association (McLean, VA) Young Investigator Award (Grant number A129622, 2017).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.