
Abstract
Introduction:
Pulmonary aspiration in infants and children is common, with 25% of the pediatric population reported to experience some type of nonspecific swallowing dysfunction. Diagnosing and managing oropharyngeal aspiration remain a challenging task due to the lack of distinguishing clinical or laboratory characteristics. We conducted a large, physician-based survey in an effort to determine the differences in the diagnosis and management of patients with oropharyngeal aspiration across different centers, using a quantitative online questionnaire.
Methods:
A survey was developed with the goal of understanding the physician demographics, diagnosis, management strategies, and the role of specialized centers for airway, voice, and swallowing disorders (also known as Aerodigestive Disease Centers). The questionnaire was sent to the pediatric membership of the American Thoracic Society.
Results:
A total of 136 questionnaires were completed and physicians from 42 different Aerodigestive Digestive Centers participated in the survey. Ninety-two percent of respondents believed that the evidence is unclear on the best methods for diagnosing lung disease related to oropharyngeal aspiration. Modified barium swallow (MBS) study and fiberoptic endoscopic evaluation of swallowing were the most useful studies in making the diagnosis of the oropharyngeal aspiration according to the participants. The majority of the participants preferred to repeat the feeding evaluations and MBS after the initial intervention. For children with suspected or confirmed aspiration, 68.6% of the respondents stated that they combine endoscopy and flexible and/or rigid bronchoscopy for further evaluation, while 27.1% preferred to perform the procedures individually at the discretion of each specialty provider. Inhaled corticosteroids were mostly prescribed if there was any component of bronchial hyperreactivity, and acid suppression therapy was primarily prescribed if there was a diagnosis or suspicion of gastroesophageal reflux disease. Empirical thickening of the feeds was not uniformly performed among the aerodigestive centers as a therapy method for the children with swallowing dysfunction with aspiration.
Conclusion:
In the survey, physicians mentioned about the importance of better guidelines for aspiration, the requirement of new diagnostic measures, the necessity of multicenter trials of sensitivity and specificity of current diagnostic tools, and developing a scoring system for reading the radiological studies for children with oropharyngeal aspiration.
Introduction
Swallowing disorders in the pediatric age group are common, with 25% of the infants and children reported to experience some type of nonspecific feeding difficulty. 1 However, the true prevalence of pediatric pulmonary aspiration remains largely unknown, as there is no gold standard diagnostic method, established registry, standardized reporting system, or other means of objectively tracking aspiration in all of the possible contexts that may occur in infants and children. 2 Oropharyngeal dysphagia is the most commonly encountered feeding disorder. Prematurity, upper aerodigestive tract anomalies, central nervous system malformations, neurodevelopmental delays, and craniofacial syndromes are risk factors for developing oropharyngeal dysphagia, although the feeding abnormalities could also be seen in otherwise healthy children. 1 Pulmonary aspiration has the potential to cause permanent damage to the developing lungs of infants and children. Therefore, it is imperative to early diagnose and appropriately manage this problem in pediatric populations. 3
Diagnosing and managing the different types of aspiration events remain a challenging task due to the lack of distinguishing clinical or laboratory characteristics. 4 There are many challenges to overcome to improve patient outcomes, including early disease recognition and treatment, identifying reliable measures of disease activity by way of clinical tools, biomarkers, quantification methods and accessible novel imaging techniques, as well as defining optimal treatment through clinical trials. These children frequently require care from multiple pediatric subspecialists, including gastroenterologists, nutritionists, otolaryngologists, pulmonologists, respiratory therapists, and speech-language pathologists. Over the past 20 years, a number of pediatric tertiary care hospitals have established interdisciplinary clinics to coordinate care for children with pulmonary aspiration. 5
Although many of these efforts have been promising, there is currently no broadly accepted consensus for the diagnosis and management of the aspiration syndromes in the pediatric age group. In the absence of such consensus, individual centers have implemented a heterogeneous assortment of workflows that may be influenced by individual physician preference, institution-specific factors, or incomplete awareness of effective solutions at competing institutions. In this work, we aimed to attain a broader perspective on pulmonary aspiration disorder approaches by conducting a nationwide survey of practices in effect at different pediatric centers, identify highly consistent workflow steps that may indicate general agreement on best practices in real-world conditions, and recognize areas of greater workflow variability that may suggest that such a consensus has yet to emerge.
Materials and Methods
We developed a questionnaire to learn about the current practices related to swallowing dysfunction with oropharyngeal aspiration in children. Questions included information about physician demographics, diagnosis, management strategies, and the role of specialized centers for airway, voice, and swallowing disorders (also known as Aerodigestive Disease Centers). Respondents were assured that their responses would be kept confidential and used for research purposes only. The questionnaire was sent electronically, using Survey Monkey, to the pediatric membership of the American Thoracic Society. This study was approved by American Thoracic Society and it was exempted from IRB approval.
Results
A total of 136 questionnaires were completed from pediatric pulmonologists. Of the participating physicians, 91.9% (n = 125) of respondents were in active practice, 83.1% were employed at an academic institution, and 61.8% were employed at a free-standing children's hospital. Average years of clinical practice since the graduation from the fellowship were 17.8 ± 10.2 years. Mean percentage of time spent in clinical settings was 61% ± 25.3%, while the time spent in research was 22.4% ± 13.4% and in other settings was 15.6% ± 12.3%.
Of the participants, 58.1% stated that they did have an aerodigestive center in their current hospital, however, 49.3% of this group identified themselves as not a member of the aerodigestive center in their institutions. Physicians from 42 different aerodigestive centers participated in the survey; 36 centers from the United States, 2 from Canada, 1 each from Australia, Brazil, Italy, and Colombia. When asked if their department/practice has a standardized approach for diagnosis and workup of oropharyngeal aspiration, 28.8% of the participants replied as “yes,” 65.3% said “no,” and 5.9% were “unsure.” Pulmonary, Otorhinolaryngology, Gastroenterology, and Feeding Team were the most common subspecialties involved in the aeordigestive centers (Fig. 1).
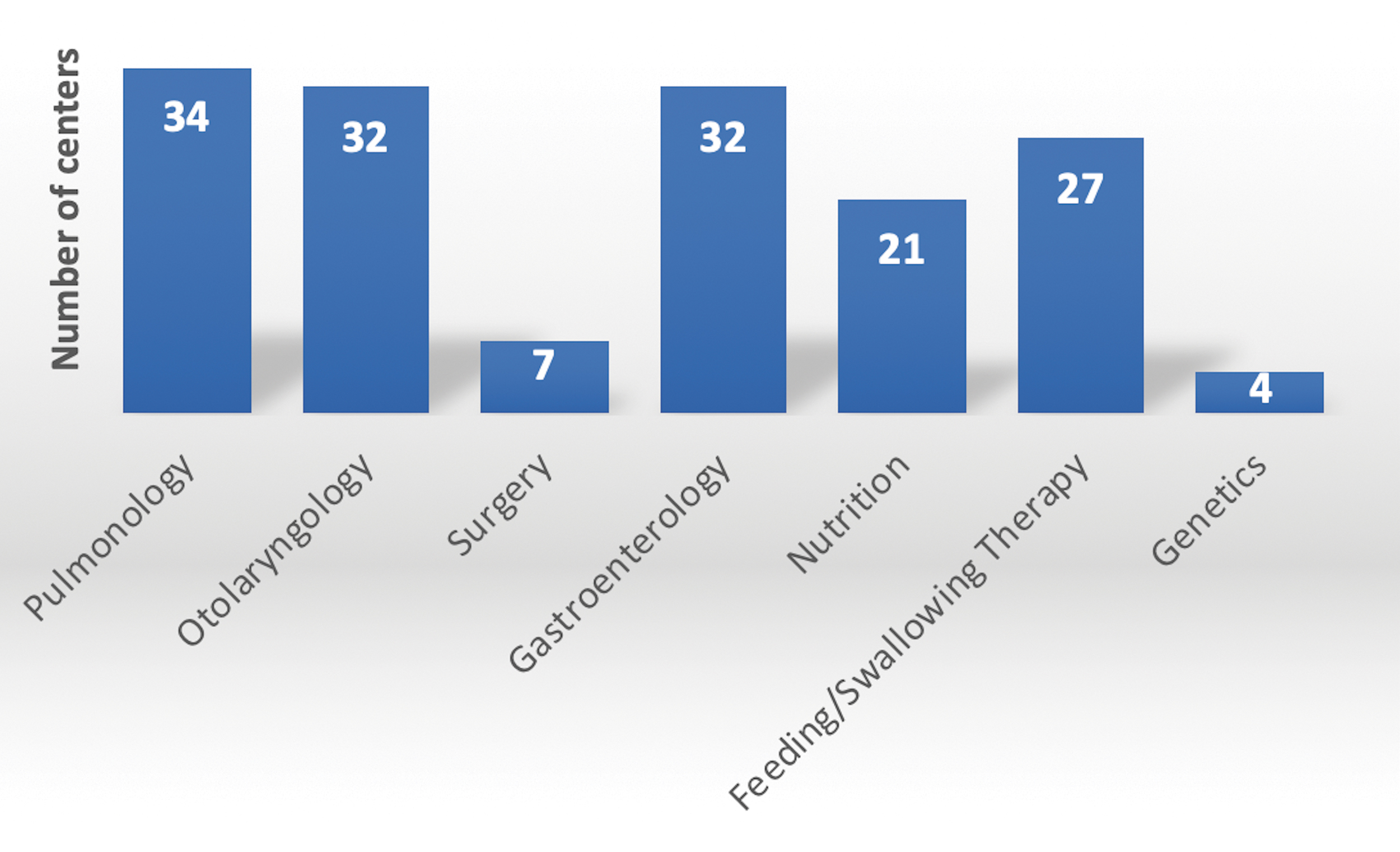
Components of aerodigestive centers. Color images are available online.
The participants stated that, the most common clinical indicators that might prompt them to suspect aspiration were gagging/choking, recurrent pneumonia, tachypnea, recurrent cough, increased work of breathing, apneas, recurrent wheezing and bronchiolitis, hoarseness, recurrent stridor, and oxygen desaturations. The other common clinical indicators were emphasized as failure to thrive, coexisting morbidities (neuromuscular disorders, genetic abnormalities, prematurity, etc.), persistent physical examination findings, radiographic abnormalities, history of emesis/reflux, chronic nocturnal respiratory findings, and impaired mucociliary clearance.
Ninety-two percent of respondents believed that the evidence is unclear on the best methods for diagnosing oropharyngeal aspiration lung disease. Modified barium swallow (MBS) study and fiberoptic endoscopic evaluation of swallowing (FEES) were the most useful studies in making the diagnosis of the oropharyngeal aspiration according to the participants (Table 1). Chest X-Ray (XR) and MBS were the most commonly ordered initial studies in the work of aspiration in the clinical practice of the respondents (Fig. 2). When asked about the utilities of the further studies, except for FEES, the answers were almost equally distributed (Fig. 3).
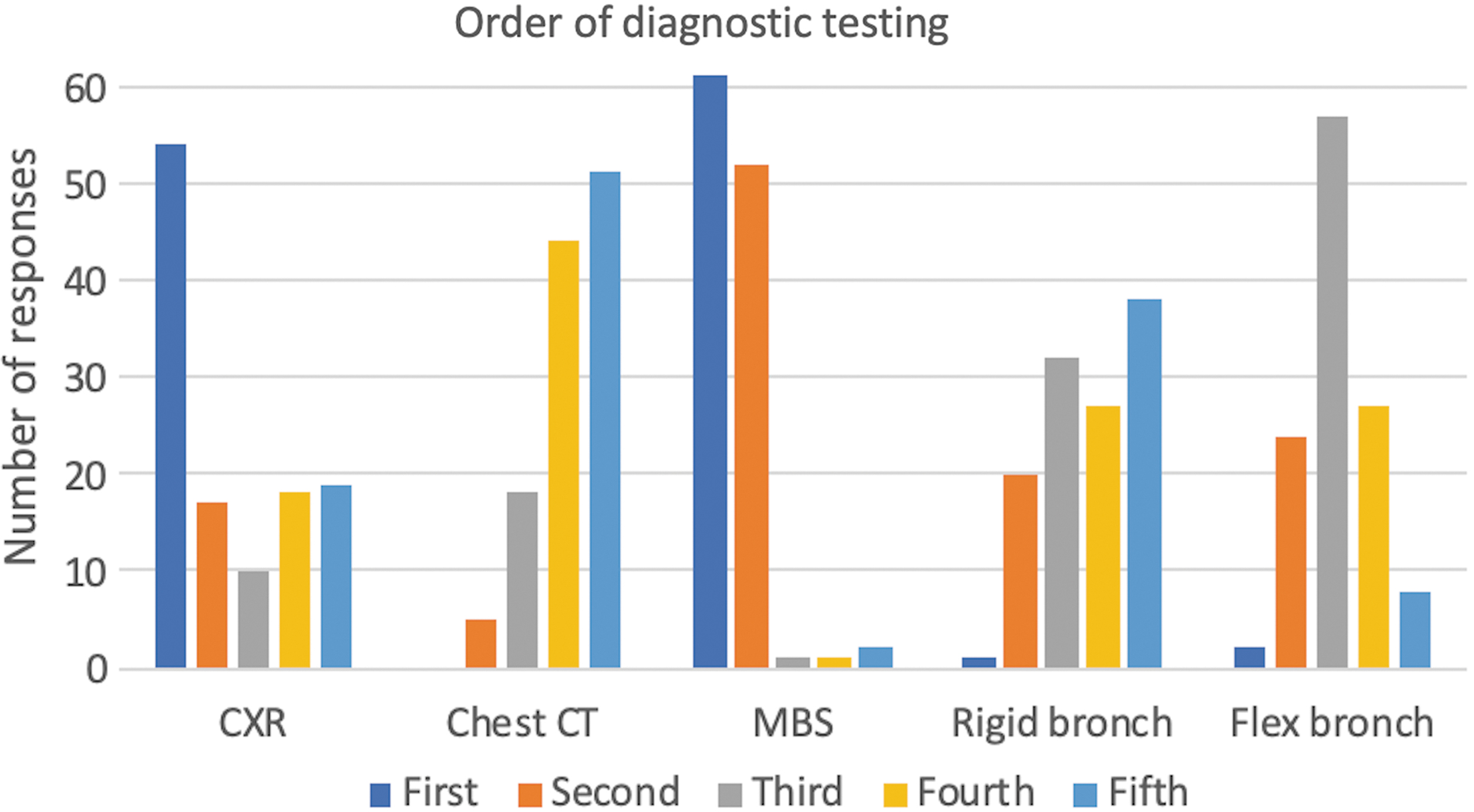
Question: In which order are you most likely to pursue the following tests? Color images are available online.
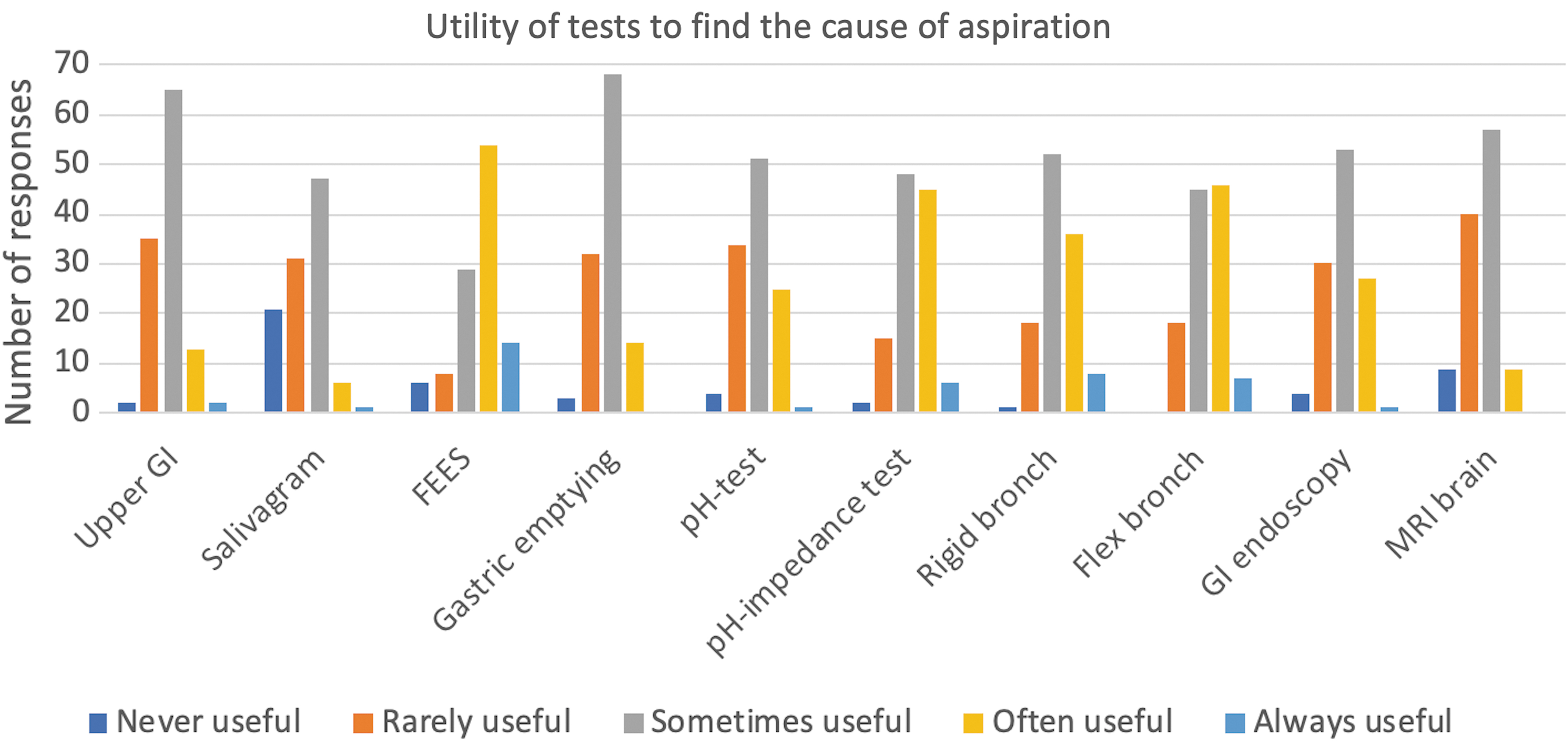
Question: How useful are the following diagnostic tests to find the cause of aspiration lung disease? Color images are available online.
Question: How Useful Are the Following Diagnostic Tests to Confirm the Diagnosis of Aspiration Lung Disease?
For children with suspected or confirmed oropharyngeal aspiration, 68.6% of the respondents stated that they combine endoscopy and flexible and/or rigid bronchoscopy for further evaluation, while 27.1% preferred to perform the procedures individually at the discretion of each specialty provider. Direct visualization of the airway anatomy (91.5%) and bronchoalveolar lavage (BAL) for cytology (83.9%) were relatively more useful aspects of flexible bronchoscopy according to the participants when compared to BAL for bacterial culture (67%), direct visualization for bronchial wall integrity (63.6%), and BAL for fungal culture (24.6%). Studying lipid-laden macrophages to confirm the aspiration was always found useful according to 9.3% of the physicians, sometimes useful according to 74.6% and never useful according to 16.1%. Only 3 centers were using pepsin and 2 centers were using bile acid from BAL or saliva samples as additional biomarkers to confirm the diagnosis of aspiration.
The majority of the participants preferred to repeat the feeding evaluations and MBS after the initial intervention (Fig. 4). Chest XR was mostly repeated if clinically needed, while chest tomography, salivagram, and flexible bronchoscopy were generally not repeated during the course of therapy.
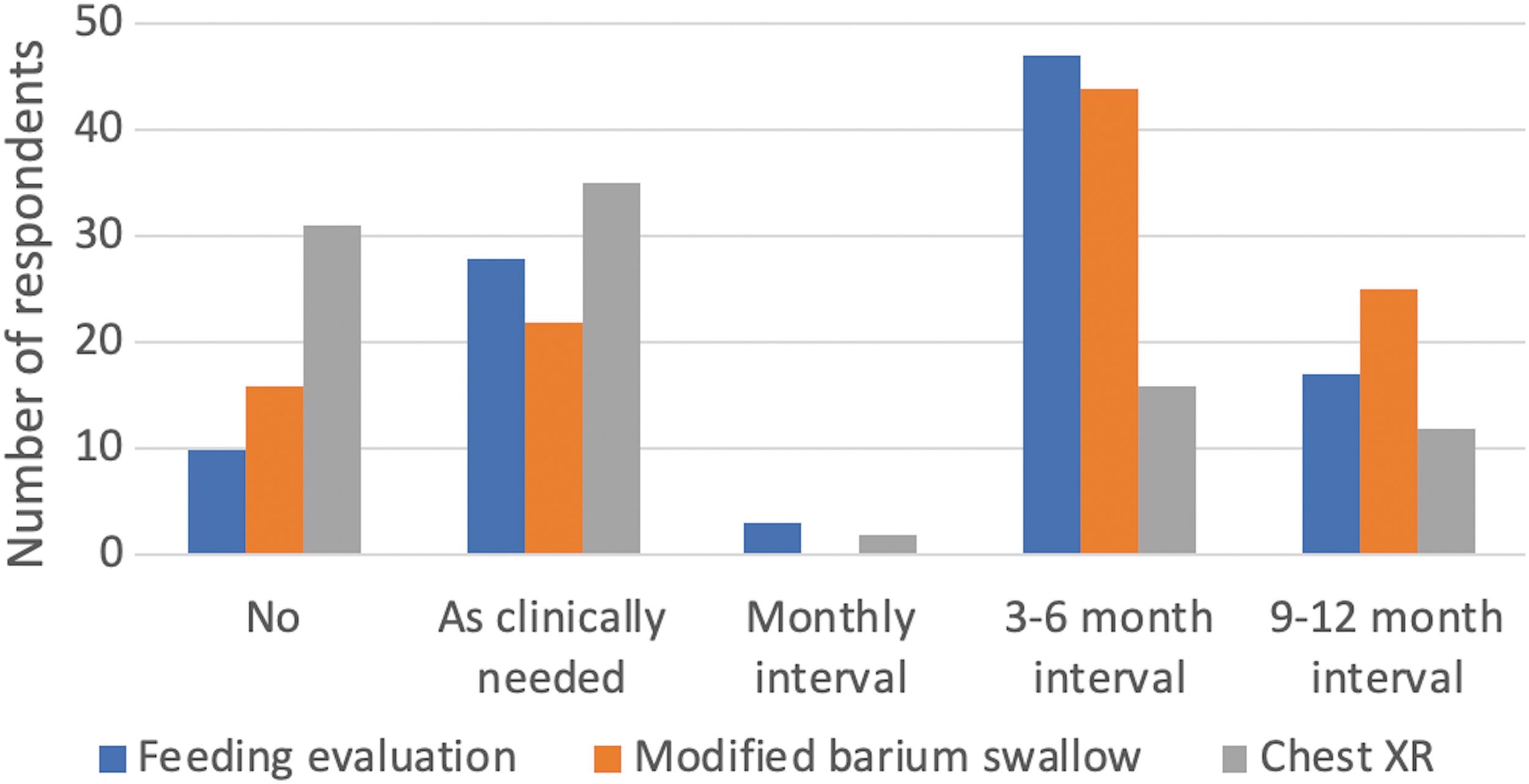
Question: Do you repeat diagnostic testing in children who aspirate and how often? Color images are available online.
The treatment choices for patients with oropharyngeal aspiration were not used the same way among different centers and providers (Table 2). Ninety percent of respondents emphasized that they do not find clear evidence for best management of aspiration lung disease. The most common reasons for prescribing inhaled steroids were having confirmed asthma, reactive component, or evidence of airway obstruction or if the physicians detected inflammation on bronchoscopic evaluation. The participants did not prefer to prescribe inhaled steroids for patients with laryngeal cleft, any other anatomical abnormalities, neuromuscular disorders unless there was a component of bronchoconstriction, and for patients who were not responsive to oral steroids.
How Often Do You Recommend These Therapies?
The 2 most common indications for prescribing acid suppression therapy were (1) clinical suspicion of gastroesophageal reflux disease and (2) gastroesophageal reflux disease diagnosed by dual pH-multichannel intraluminal impedance or esophagitis seen on biopsy. Most common clinical scenarios for empirically thickening the oral fluid intake were (1) awaiting MBS study, (2) strong clinical suspicion, (3) gastroesophageal reflux disease or spit-ups, and (4) neurological or developmental deficits. The majority of the participants preferred postpyloric tube feeds (62.6%) for children with aspiration who require enteral tube nutrition, while 23.4% preferred gastric feeding (nasogastric tube or gastrostomy tube); 14% of the respondents stated that the clinical situation of the patient is important in making the decision of the feeding route for the management of aspiration.
Discussion
Pulmonary aspiration syndrome is a frequent problem, which particularly affects a vulnerable population in the pediatric age group and is often underestimated or misdiagnosed. 4 Pulmonary aspiration might be secondary to swallowing disorders, gastroesophageal reflux disease, laryngeal clefts, tracheoesophageal fistulas, and/or saliva aspiration. Although the technological advances, new treatment modalities and intensive care approaches have led to increased survival rates for patients of all ages, poor airway protection during the aspiration event is an important contributory factor to aerodigestive morbidity. 6 The primary goal of pediatric interdisciplinary coordination of care is to improve outcomes; over the past couple of decades, a number of pediatric tertiary care hospitals have established interdisciplinary clinics to coordinate care, however, many clinical practices are accepted widely on the basis of experience. 7 In this study, we conducted a large, physician-based study to determine the differences in the diagnosis and management of patients with aspiration across different centers, using a quantitative online questionnaire. There were no major differences in responses between US versus non-US centers except for some minor variance in wording and approaches in open-ended questions.
The correct recognition of the pulmonary aspiration syndromes is greatly impeded by the absence of gold standard diagnostic tools and biomarkers that can truly pinpoint the diagnosis. To be able to differentiate between the distinct types of aspiration could have significant prognostic and therapeutic implications. Numerous biomarkers in serum, sputum, and BAL have been studied, however, their role in the identification of aspiration still remains controversial. 4 In our survey, in addition to the history and physical examination, MBS study and FEES were considered as the most reliable tools in making the diagnosis of oropharyngeal aspiration according to the respondents. Clinical feeding evaluations and/or the MBS studies were the preferred follow-up studies after the initial interventions in majority of the centers. Biomarkers such as pepsin, bile acid, C-reactive protein, procalcitonin, cytokines, and studies such as exhaled breath condensate leukotrienes or dye imaging were not routinely used in any of the centers participated in the study. In the survey, physicians mentioned about the importance of better guidelines for aspiration, the requirement of new diagnostic measures and the necessity of multicenter trials of sensitivity and specificity of current diagnostic tools and developing a scoring system for reading the radiological studies for children with aspiration. The participants also emphasized the significance of tailoring the evaluation and management according to each individual based on their underlying conditions.
The empirical data regarding the efficacy of treatment intervention are essential for provision of evidence-based practice. 2 In our survey, the majority of the physicians stated that currently there is no clear evidence for best management of aspiration lung disease. Inhaled corticosteroids were mostly prescribed if there was any component of bronchial hyperreactivity, and acid suppression therapy was primarily prescribed if there was a diagnosis or suspicion of gastroesophageal reflux disease. Empirical thickening of the feeds was not uniformly performed among the aerodigestive centers as a therapy method for the children with oropharyngeal aspiration; however, feeding/nutritional training for children with oral-phase swallowing problems was largely recommended, which generally involves exercises aimed at improving the sensory and/or motor skills required for drinking and eating. Some physicians emphasized that, without confirmatory diagnostic testing, recommendations for management unfortunately seem premature. The prophylactic antibiotic therapy was not routinely recommended, however, some centers preferred to use alternate day azithromycin until the swallowing functions mature. According to some participants, aspirating saliva is also a big problem especially for patients with neuromuscular disorders, and the role of salivary gland botulinum toxin application needs to be demonstrated as this use is considered off-label by the Food and Drug Administration and some centers offer this therapy in their clinical practice.
In this study, we aimed to identify the current status of the aerodigestive centers and their approach to diagnosing and managing the children with aspiration lung disease. Discussing the evidence behind all the diagnostic measures and treatment modalities was beyond the scope of this article. Differential diagnosis and management of the pulmonary aspiration syndromes are often not straightforward and require collaboration between multiple disciplines. Although the increasing number of aerodigestive centers and research trials are encouraging for better management strategies in the future, almost all the participants in our study stressed the importance of establishing a best practice model that could be followed in different institutions. This study once again showed that there are many unknowns and uncertainties about oropharyngeal aspiration-related lung disease and its management. Additional research efforts will provide the needed data to guide future management and intervention protocols.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.