
Abstract
Pediatric severe asthma is a complex syndrome associated with significant morbidity and financial cost. Affected children often have poor school attendance, and day to day suffer with poor sleep quality, and reduced exercise performance. Children with severe asthma are at higher risk of obesity and its complications, to the extent that dyspnea due to deconditioning is mistaken for poor asthma control. 1 During winter, children with severe asthma frequently experience lapses in symptom control with the annual rhinovirus and flu seasons, and not uncommonly require acute care and ICU admissions for seasonal exacerbations. As a result, care providers often have interrupted employment schedules, and the siblings of children with severe asthma are adversely impacted by a chaotic home environment. Single parents of a child with severe asthma must involve extended family members to care for the child to work. Asthma medications have increased in cost, to the extent that middle-income families are challenged by the out-of-pocket costs of branded metered-dose inhalers and co-pays associated with health care. The social determinants of health are vitally important in affecting asthma outcomes, a glaring truth that has been grossly underestimated by health care providers, drug manufacturers, public health officials, and governments.
The driving principle in the formulation of treatment guidelines for severe asthma is the view that it predominately is a disorder of type-2 mediated airways inflammation, which, if managed appropriately, is effectively controlled by appropriate dose inhaled corticosteroids (ICSs) combined with long-acting bronchodilators. Our experience at the University of Virginia (UVA) has been that most children evaluated for problematic wheeze/asthma who undergo detailed studies do not have type-2-predominant lung inflammation (Fig. 1). 2 Furthermore, we have struggled to provide medications that conform to the guidelines. For example, in peer review of our article describing the phenotypic characteristics of school-age children with poorly controlled asthma, 2 1 reviewer pointed out the relatively low proportion of children in the sample not treated with high-dose ICS/long-acting beta agonist (LABA) combination therapies. Despite significant effort, we could not get Medicaid managed care organizations and private health insurers to cover the costs of these medications! As a result, ∼40% of the children in that report were treated with alternate day oral prednisone, a practical solution that costs pennies compared with the out-of-pocket cost for an ICS/LABA inhaler. Paradoxically, in an era when the pharmacotherapy of asthma has greatly improved, asthma symptom control is poor in many patients. 3
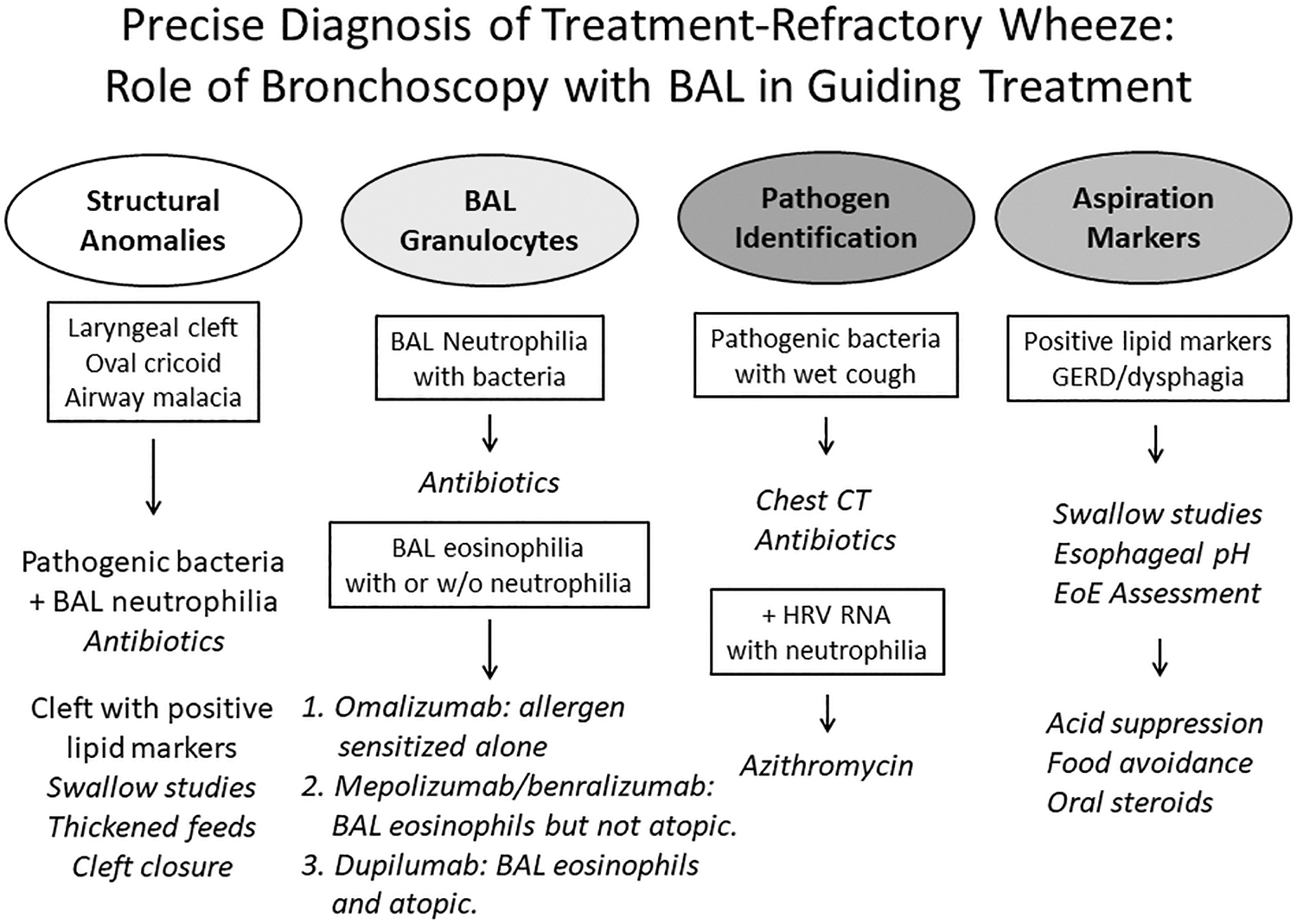
Approach to the precise diagnosis of problematic wheeze/asthma of childhood. Bronchoscopy advised in children with poor symptom control despite supervised treatment and evaluation of comorbid conditions and remediable factors. Important elements of the evaluation include examination of the larynx and lower airways for anomalies, and BAL for assessment of granulocytes, pathogens, and quantification of lipid-laden macrophages. With experience and monitoring, this approach is safe with a low prevalence of major expected and unexpected adverse events. 2 BAL, bronchoalveolar lavage.
Even though severe asthma is highly prevalent in children, the National Institutes of Health/National Heart, Lung and Blood Institute (NIH/NHLBI) Severe Asthma Research Program (SARP) investigators have focused more on adults than children. 4 Severe asthma of childhood typically does not progress from mild asthma, but instead emerges in late preschool years as “severe from the start,” and a subgroup with airflow limitation can be identified early in life. There is great heterogeneity in phenotypes, 5 although type-2 mediated respiratory mucosal inflammation is often found, 2 the predominant airspace T helper cell motif is Th1/Th17, supporting the important role of respiratory pathogens in regulating airspace inflammatory signatures. 6 Most children with severe asthma have normal lung function between exacerbations, but demonstrate heightened bronchodilator responsiveness. 4 Peripheral blood eosinophilia is common, and most children with severe asthma have significant immunoglobulin E (IgE)-mediated sensitization to environmental allergens. The lung fluid contains increased eosinophils and neutrophils, 2 and expired nitric oxide is often elevated. An important newly recognized feature of severe asthma of childhood is a significant degree of ventilation heterogeneity, manifest as large ventilation defects with hyperpolarized noble gas magnetic resonance imaging. 7
Whereas the definition of severe asthma is based on the requirement of treatment with high-dose corticosteroids and a second controller to maintain symptom control, 8 the issue of corticosteroid resistance has been raised repeatedly, and studied further by SARP investigators. However, SARP, similar to most large asthma research consortiums, has only partially considered poor adherence and the social determinants that inform outcomes (Fig. 2). The true prevalence of end-organ corticosteroid resistance in severe asthma is not well understood. However, stimulated by the opportunity to improve outcomes in adults, biological therapies have been developed by the private sector to treat corticosteroid-refractory severe asthma. The first to market was omalizumab, targeting the IgE receptor, with significant benefit for children down to age 6 years with demonstrable allergen sensitization. Then came mepolizumab (Mepo) and benralizumab, targeting eosinophil-driven asthma through inhibition of IL-5 and IL-5R. “Mepo” was recently approved down to age 6 years for children with eosinophilic asthma. After the success of omalizumab and mepolizumab, dupilumab, which targets IL-4R, suppresses IgE- and eosinophil-mediated inflammation. Despite their efficacy, how have these biological therapies actually been used in the at-risk population of children with severe asthma? And second, what is a feasible pathway to justify their use, given their high cost and the fact that so many outcomes in severe asthma of childhood are explained by social factors and low adherence to treatment?
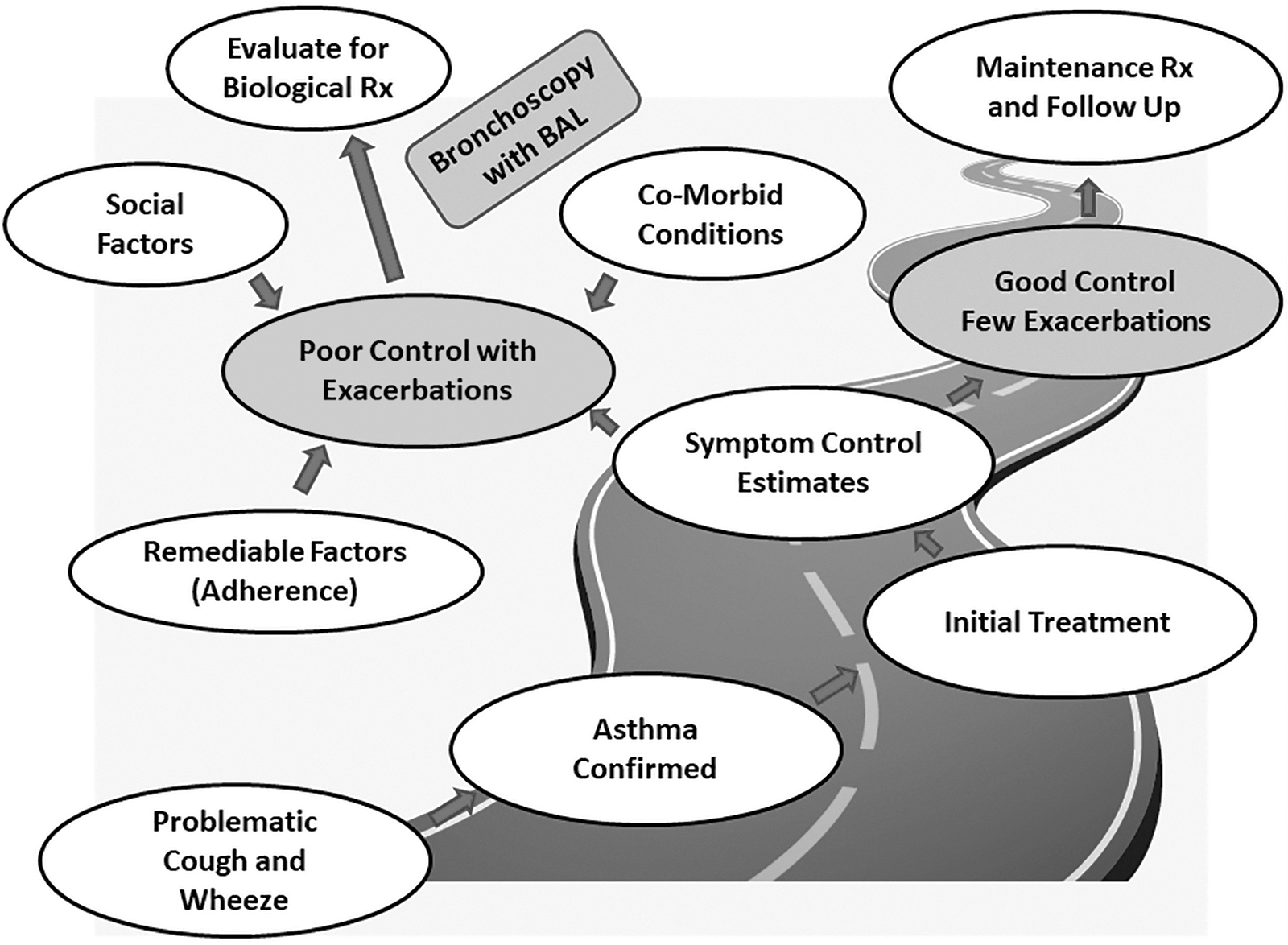
Real-world approach to the assessment of the child with problematic cough and wheeze. Important steps are to confirm the diagnosis of asthma before initiating guidelines-appropriate treatment. Symptom control should be assessed objectively with validated control scales and longitudinal lung function measures. Children with poor control and frequent exacerbations are offered a detailed evaluation, including assessment of remediable factors (inhaler technique), social factors (access to medications and home environment), and comorbid conditions. Once this evaluation is completed, children who remain poorly controlled are offered bronchoscopy and BAL to precisely select the appropriate biologic. BAL, bronchoalveolar lavage.
The gap between treatment promise and treatment provision has never been wider in severe asthma of childhood. We maintain a registry of children with severe poorly controlled asthma referred to the UVA for care. Children in the program who fail guidelines-directed therapy have adequate adherence, and comorbidities addressed, are offered bronchoscopy and bronchoalveolar lavage as a means to guide revised treatment (Figs. 1 and 2). Over an 11-year span, we have evaluated 243 children >5 years with a confirmed diagnosis of poorly controlled asthma who had clinically indicated bronchoscopies. Only 60% had been treated high-dose ICS, including 58% with combination ICS/LABA, yet 23% required maintenance oral prednisone! These patients had been under the care of pediatric asthma specialists for months, and many were enrolled in government-funded managed care organizations that would not approve treatment with combination of ICS and LABA. At the time of bronchoscopy, despite a high prevalence of allergen sensitization (66%), and a sample geometric mean total IgE of 131 IU/mL, only 5% were treated with omalizumab. Peripheral blood eosinophilia (>300 cells/μL) was common (44%), yet only 3.3% of the sample was treated with either mepolizumab or benralizumab. Efforts to obtain these biologicals required a significant coordinated staff effort, frustrated by payor denials and requests for reapplication, and overall was a lengthy process, which often resulted in failure. Henceforth, in an era when the prospects for more effective nonsteroidal treatment of severe asthma of childhood are highly promising, biologics are difficult to obtain.
What are some practical solutions that readers of Pediatric Allergy, Immunology, and Pulmonology can offer to their patients? Foremost is to consider the social determinants of health. Discussions in the office can center around topics such as school and exercise performance, challenges in using inhalers, and peer influences. Many communities have organizations that include volunteer attorneys to address issues of substandard housing and financial pressure exerted by landlords. 9 Community churches have an enduring legacy of trust among urban African Americans, and patients with asthma can be engaged through pastors and health ministries. 10 If handled poorly, the issue of inconsistent adherence can dilute what should be an empowering relationship between providers and patients' families. Adherence must be discussed directly with the caregiver and child so that providers can learn about the environment of care and barriers to adherence. Often the foundation of inconsistent adherence is lack of understanding, and providers should engage families as empowering teachers and counselors and avoid judgmental statements. Treatment recommendations should be aligned with the child's lifestyle. As providers of care, we treat children not guidelines! Providers must develop a level partnership with families and children, open to practical issues that impact care. The first step is to listen patiently. When revisions in care are made or escalated, providers should explain to the family the rationale and discuss safety concerns. The “system” of quality monitoring primarily rewards good outcomes and limited resource allocation, values that are often at odds with nurturing provider relationships. As advocates for children, providers must expect managed care organizations and the government to fund indicated combination ICS/LABA inhalers and biologics for severe asthma. Comparative clinical trials of different biologics or biologics versus standard treatment are urgently needed and will not likely be conducted by private industry. It is indeed a promising time for children with severe asthma; however, unless the chasm separating expensive biologics and the financial priorities of the health care consumer is bridged, many deserving children will go untreated even in a society that can routinely afford thousand dollar cell phones.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Ivy Foundation, University of Virginia; iTHRIVE CTSA UL1TR003015/KLTR003016; NIH/NIAID PA-19-0530 SF424; NIH/NHLBI 7UG1HL139126-03.