
Abstract
Progressive multifocal leukoencephalopathy (PML) is a fatal demyelinating disease of the central nervous system that is caused by John Cunningham virus (JCV). It occurs almost exclusively in immunosuppressed individuals, for example, patients with AIDS and hematological and lymphoreticular malignancies. In this article, we present a review of the literature and 2 case reports with PML. The first report examines a 15-year-old male (who presented with dedicator of cytokinesis 8 deficiency) who was diagnosed as having PML based on characteristic magnetic resonance imaging (MRI) lesions and a positive PCR for JCV in cerebrospinal fluid. He was transferred for bone marrow transplantation after stabilization with therapy of maraviroc and cidofovir. The second report examines a 6-year-old male who presented with encephalitis and was also diagnosed with AIDS. He was diagnosed with PML and started treatment with cidofovir. His clinical status and MRI findings deteriorated rapidly. In immunosuppressive patients who developed encephalopathy, JCV ought to be considered.
Introduction
John Cunningham virus (JCV) was first identified in 1971 by isolating it from the brain tissue of a patient diagnosed with progressive multifocal leukoencephalopathy (PML). JCV is species-specific double-stranded DNA virus that infects >70% of human population. 1 It occurs almost exclusively in immunosuppressed individuals, for example, patients with AIDS, hematological and lymphoreticular malignancies, autoimmune rheumatological diseases, patients who underwent organ transplantation, and receive immunomodulatory therapy with monoclonal antibodies (eg, natalizumab, rituximab). PML is an often fatal demyelinating disease of the central nervous system that is caused by JCV. PML occurred in as many as 4% of AIDS cases, before the advent of highly active antiretroviral therapy (HAART). 2 We would like to report 2 cases we followed up with a diagnosis of PML due to JCV.
Case 1
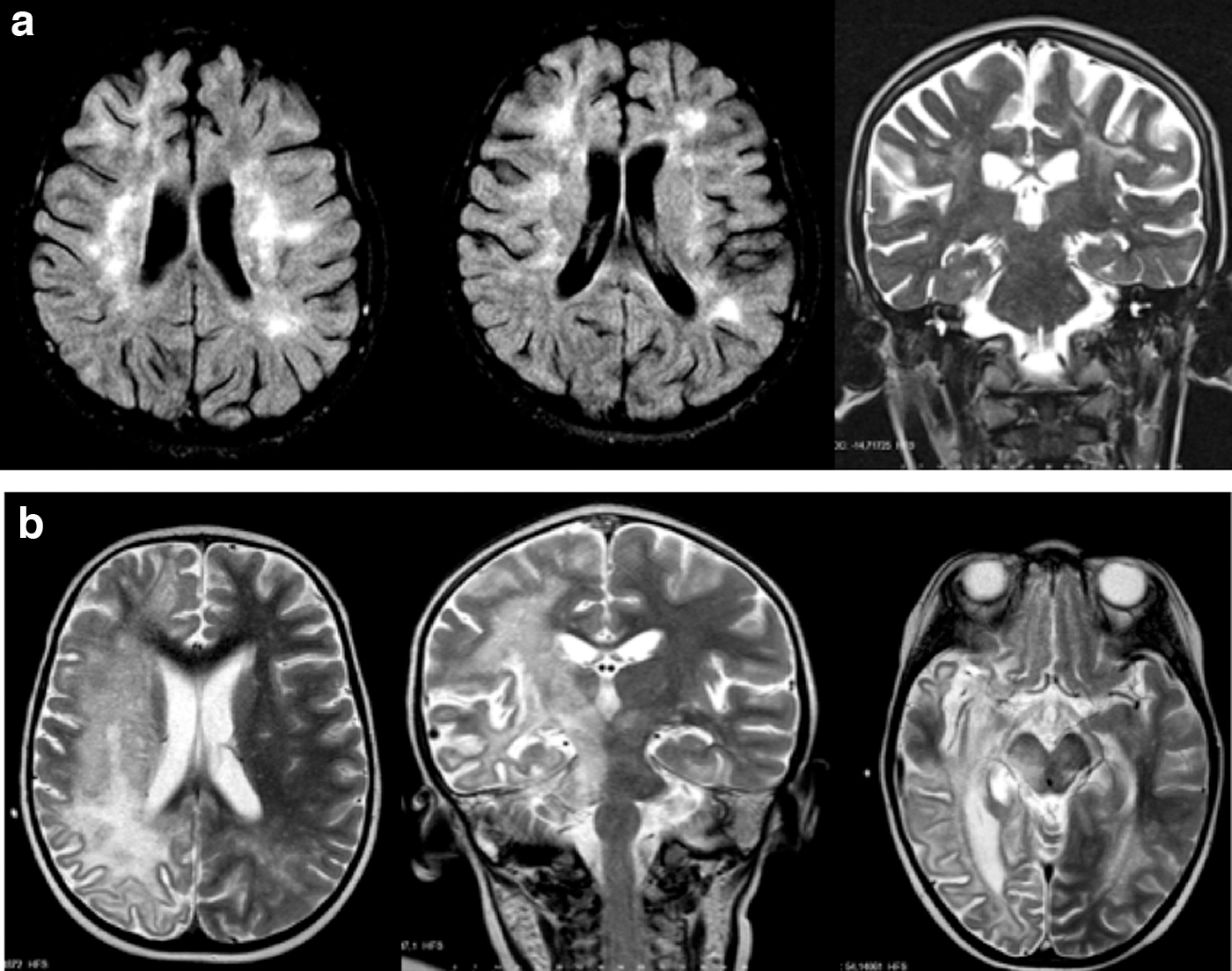
A 13-year-old male, who had been diagnosed with atopic dermatitis at the age of 4 years, presented with progressively worsening purulent lesion on the nose for the past 3 months. He had a consanguineous family. Upon examination, it was found that there was a 3- to 4-cm lesion with purulent inflammation enlarged enough to close the nasal entrance on the patient's nose. His weight and height were under the 3rd percentile and he had papilloma on his hands and arms. Laboratory test revealed the following results: neutrophil 3,300/μL (N: 1,800–8,000/μL), lymphocyte 1,100/μL (N: 1,500–6,500/μL), immunoglobulin G (IgG) 1,005 mg/dL (N: 639–1,349 mg/dL), immunoglobulin E 540 ku/L (N: <100 ku/L), nitroblue tetrazolium 75% (N: >20%), CD3 61% (N: 52%–78%), CD4 33% (N: 25%–48%), CD8 28% (N: 9%–35%), CD19 17% (N: 8%–24%), and CD16/56 8% (N: 6%–27%). Dedicator of cytokinesis 8 (DOCK-8) protein expression was detected very low in flow cytometric analysis. Heterozygous missense mutations were detected in TRAF3IP2 and TYK2 in next generation sequencing panel including DOCK8, CYBA, ICAM1, CYBB, and CARD9 genes and further genetic analysis such as whole exome sequencing or whole genome sequencing could not be performed. He was treated with intravenous immunoglobulin and α-interferon 2b for 2 years. When he became 15 years old, he presented with generalized tonic–clonic convulsion. He was diagnosed as having PML based on characteristic magnetic resonance imaging (MRI) lesions such as patch lesions in the subcortical deep white matter in both frontoparietal lobes (Fig. 1a). JCV in cerebrospinal fluid was detected at 23,900 copies/mL. First, we discontinued α-interferon 2b therapy. After that, maraviroc (300 mg/day) and cidofovir (5 mg/kg per dosage) treatments were initiated. Intravenous immunoglobulin (IVIG) and cidofovir were continued for 10 months, the neurological examination and imaging remained stable during this period. He was transferred for bone marrow transplantation. However, the patient died due to septicemia during the post-transplant period.
Case 2
A 6-year-old boy had been admitted to the hospital with a first generalized tonic clonic convulsion and hemiparesis. On physical examination, the patient's Glasgow coma score was 9, he had central facial paralysis and hemiparesis. Blood tests were performed with the diagnosis of encephalitis and resulting with lymphocyte 710/μL (N: 1,500–6,500/μL), IgG 2,310 mg/dL (639–1,349 mg/dL), anti-HIV reactive, HIV RNA 54,034 copies/mL, lymphocyte subgroups resulted in CD4 18/mm3 (N: 400–2,100/mm3), CD8 62/mm3 (N: 200–1,200/mm3), and CD4/8 0.3 (N: 0.9–3.4). On cranial MRI, diffuse white matter signal anomaly is seen at the right side. It is more remarkable in parietal and temporal lobes; subcortical U fibers are involved, and signal anomaly extends to the opposite hemisphere along the posterior corpus callosum splenium segment. There is extension along the right capsule to the front basal white matter posterior leg of internal capsule, thalamus, cerebral pedicle, right side of the brain stem, and right cerebral pedicle (Fig. 1b). Ceftriaxone, acyclovir, and dexamethasone initial treatments were administered to the patient who was considered of HIV infection and secondary encephalopathy. HIV RNA copies were 1,450,000 ıu/mL in cerebrospinal fluid (CSF). Antiretroviral treatments were initiated (lopinavir/ritonavir, lamivudine/zidovudine). The patient was referred to our department because there was no clinical improvement. We detected JCV in CSF because the neurological imaging was compatible with PML, and JCV was determined as 13,700,000 copies/mL. The patient received a single dose of IVIG (0.5 g/kg) and 6 doses of cidofovir treatments. The bulbus and brainstem involvement was detected and seen in cranial MRI. Eventually the patient died due to cardiopulmonary arrest.
Discussion
PML tends to not occur in immunologically healthy individuals, and it develops after JCV infection primarily in oligodendrocytes, with subsequent demyelination of subcortical white matter in the CNS by lysis of oligodendrocytes. 3 In a patient with progressive focal neurological deficits consistent with PML, neuroimaging is indicated. The combination of a characteristic clinical picture and typical imaging findings supports a confident presumptive diagnosis of PML, 4 but it is established by demonstrating the presence of JCV DNA in the cerebrospinal fluid using PCR.
It is recommended to discontinue or decrease any potential sources of immunosuppression in PML patients without HIV infection. Possible benefit is suggested by the case reports of renal, liver, and heart transplant recipients who survived PML after immunosuppression was reduced. One report described that 2 PML patients on immunosuppressive therapy showed clinical and radiological improvement after partial taper or cessation of immunosuppression. 5 In the first case, we also discontinued immunomodulatory therapy, but it did not stop the progression of disease. Therefore, we decided to give maraviroc (300 mg/day) and cidofovir (5 mg/kg per dose) treatments for PML. In several cases of patients with PML, the addition of maraviroc was associated with clinical improvement, 6 however, no benefit was found in the other cases. 7 It is possible that maraviroc efficacy may be higher if administered on earlier stages of HIV and JCV disease. Cidofovir is a nucleotide analogue approved for the treatment of cytomegalovirus retinitis in HIV-infected patients. Several case reports have shown its efficacy, but the largest clinical studies reported no benefit. 8 Our patient received 5 mg/kg once weekly for 2 weeks, followed by a maintenance dose of 5 mg/kg biweekly. The patient has remained stable while receiving cidofovir treatment and this may suggest that it has played a considerable role in improving symptoms of PML. However, this patient died due to sepsis after being referred to the bone marrow transplantation with the diagnosis of immune deficiency.
The other one presented with encephalopathy before HAART was initiated. HIV infection accounts for ∼85% of the total cases, and its prevalence in this population is ∼4%–5%. With the adoption of HAART, the incidence of PML decreased substantially. Studies in HIV-positive patients indicate that increases of CD +4 T cell counts from 100 to 200/μL are associated with decreased morbidity and mortality, and CD4 T cell counts >200/μL are associated with improved PML outcome. 9 However, we are considering that neurological findings progressed rapidly in our patient due to the administration of steroid before HAART and the late detection of JCV. Despite the improvement in the cellular functions of the patient, his neurological status and radiological findings deteriorated, and the patient has died. Immune reconstitution remains the most effective strategy for the treatment of PML. But this strategy depends on early diagnosis, rapid and effective immune repletion. 10 There are still many unknown facts about the pathophysiology of the disease. PML will continue to be a risk with the use of various immunosuppressive therapies. Viral-like particles may be used to develop a vaccine against pathogenic JCV, eliminating the risk of developing PML altogether. 11 However, there is no effective treatment currently, and more studies are considered necessary.
Conclusion
There is currently no specific treatment for PML, which has a high mortality rate. The main approach is restoring the host adaptive immune response, a strategy that differs according to clinical setting. 12 Treatment guidelines for PML recommend starting antiretroviral therapy immediately in patients with HIV infection who are not on therapy and optimizing the antiretroviral regimen for virological suppression in patients who are receiving antiretroviral therapy. 13 In an immunosuppressive patient who developed encephalopathy, JCV should be considered and examined with MRI and molecular methods.
Ethics
Informed and written consent to publish the patients' data was obtained from the parents. Ethics approval for the study was granted by Istanbul University, Faculty of Medicine Clinical Research Ethics Committee.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
No funding was received.