
Abstract
Background:
We describe a rare case involving paracetamol, a commonly used drug worldwide. Increased paracetamol consumption increases the risk of adverse drug reactions.
Case Presentation:
This is a case of a 9-year-old girl who visited the emergency department due to sudden onset sneezing, nasal itching, urticaria, and angioedema after paracetamol ingestion. The diagnostic and etiologic studies revealed an immunoglobulin E (IgE)-mediated hypersensitivity mechanism to paracetamol.
Conclusion:
Few cases of this phenomenon have been reported in previous literature. As confirmed in this study, a negative skin prick test did not exclude hypersensitivity, and conducting intradermal tests (IDTs) increased diagnostic accuracy. The patient had a positive IDT, confirming the underlying IgE-mediated reaction. The follow-up of a confirmed paracetamol hypersensitivity implies patient education about avoidance of any paracetamol-containing formulation, including combination products and clarification of available alternative drugs. This is likely the first publication documenting IgE-mediated paracetamol allergy in pediatric patients. We intend to underline the clinical benefits of diagnostic confirmation toward suspected drug hypersensitivity reactions in children, a particularly useful topic for pediatricians and pediatric allergists.
Introduction
This is a rare case involving paracetamol, a commonly used drug among pediatric patients worldwide. It has become ubiquitous as it is a nonprescription drug, available over-the-counter, with an excellent safety profile. 1 In Portugal, it has been the most sold active substance since 2003. 2 Increased consumption results in an increased risk of adverse drug reactions (ADRs). 1 The risk of paracetamol anaphylaxis is low, as immunoglobulin E (IgE)-mediated paracetamol-induced hypersensitivity is rare, with only a few pediatric cases reported in the literature. 2 In oral challenge test (OCT)-proven paracetamol-hypersensitive patients described in literature, neither skin prick test (SPT) nor intradermal test (IDT) was positive. 3 In clinical practice, an evaluation involving skin tests and OCTs, concomitantly, is rare. 3
This case report is unique, as this concomitant evaluation was carried out, with a proven IgE mechanism to paracetamol among pediatric patients.
Case Presentation
This is a case of a 9-year-old girl with a history of atopic dermatitis and mild persistent allergic rhinoconjunctivitis, who visited the emergency department due to sudden onset sneezing, nasal itching, urticaria, and facial angioedema.
The history revealed accidental inhalation of sodium hypochlorite with a subsequent severe headache. As a result, the patient took 250 mg (7 mg/kg) of paracetamol, and the symptoms occurred a few minutes after ingestion. Aside from paracetamol, no other medication was taken, and the patient was not under medical prescription in the previous days. In the emergency department, she presented with facial angioedema, characterized by swollen lips and eyelids, and generalized urticaria, characterized by pruritic papules and plaques, which were circumscribed, slightly elevated, erythematous, and edematous. There were no hemorrhagic lesions, arthralgia, or respiratory or gastrointestinal tract symptoms. Intravenous clemastine and oral dexamethasone were administered, and the symptoms clinically resolved within ∼30 min.
She was discharged from the emergency department and was referred to a pediatric outpatient consultation. The history confirmed that she had previously ingested paracetamol without developing an abnormal reaction and tolerated ibuprofen. The patient was suspected of having an allergic reaction to paracetamol. After obtaining parental informed consent, the patient underwent an OCT. She tested positive at 20 mg (0.5 mL) of paracetamol with concomitant manifestations of sneezing, nasal itching, conjunctivitis, and generalized urticaria. The OCT was terminated, and diagnostic studies were performed to clarify and document the pathophysiological mechanisms underlying this reaction. Six months later, the patient underwent an SPT with injectable paracetamol solution (10 mg/mL) and IDTs with a 1:10 and 1:100 dilution of paracetamol in 0.9% sodium chloride.
The SPT was negative (Fig. 1). The first IDT with a 1/100 paracetamol dilution was equivocal; however, a positive result was obtained with paracetamol IDT at 1/10 dilution (paracetamol ID 1 mg/mL) (Fig. 2). Serum-specific IgE measurement to paracetamol was negative with a total IgE level of 595 KU/L. Based on these results, the patient was diagnosed with a paracetamol IgE-mediated hypersensitivity reaction. Consequently, she was prescribed to abstain from paracetamol. Ibuprofen, which was previously tolerated, was recommended as an alternative.
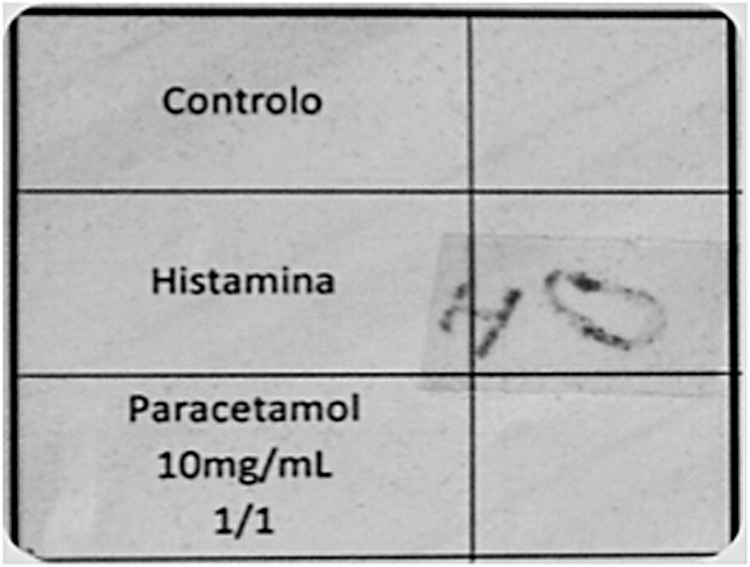
Prick test: negative result, as reaction with paracetamol is identical to that of the negative control.

IDT: Doubtful result with paracetamol at 1/100 dilution, but a positive result with paracetamol at 1/10 dilution (paracetamol ID 1 mg/mL). IDT, intradermal test.
Diagnostic Approach
Detailed history taking and anamnesis, specifically concerning the patient's drug intake history, are essential. 1 Our patient denied previous allergic reactions to oral paracetamol, which have been used in acute febrile situations. Theoretically, a drug that has been tolerated on multiple occasions is unlikely to cause an allergic reaction. Based on this, paracetamol allergy could have been excluded in our patient. However, patients tend to focus on the initial symptoms rather than the later drug-induced symptoms. Therefore, previous signs of paracetamol-induced hypersensitivity may have been missed. 4 Using the Naranjo Adverse Drug Reaction Probability Scale, the patient's score can be classified under “probable,” consistent with previous studies on allergies or ADRs. 5
The differential diagnosis includes hypersensitivity to concomitant drugs and skin/mucosal diseases. 1 These hypotheses were excluded as the reaction occurred accidentally, rather than coincidentally with the acute phase of illness. Allergy to sodium hypochlorite was initially considered, but a subsequent exposure of the patient to this cleaning product developed no reaction. Regarding the diagnostic approach, in vivo skin tests have minimal diagnostic value because they are specific but not sensitive. Their utility is limited by the lack of standardization and scarcity of available commercial reagents. In this study, a negative SPT did not exclude hypersensitivity, and conducting IDT increased diagnostic accuracy. Moreover, the negative serum-specific IgE finding in a proven IgE-mediated mechanism reinforced the low sensitivity of this approach.1,6
In our patient, a positive IDT confirmed the IgE-mediated reaction.
The gold standard for the diagnosis or exclusion of hypersensitivity is the drug provocation test (DPT). In this case, it was unnecessary since there was an immediate reaction after paracetamol intake. The development of severe clinical symptoms is a contraindication for this method. However, the family attributed the symptoms to sodium hypochlorite and decided to undergo DPT for diagnostic clarification.
Discussion
ADRs can be classified as A and B types. A-type ADRs are more common (70%–80%), dose dependent, and predictable. 7 An example of this is the hepatotoxic effect of the N-acetyl-p-benzoquinone imine nonprimary cytochrome pathway metabolism product. 4 B-type ADRs are unpredictable and unrelated to the pharmacological effects of the drug at normal dosage. These include hypersensitivity reactions. Drug hypersensitivity reactions (DHRs) are adverse drug effects that clinically resemble allergic reactions. In contrast, drug allergies are DHRs with a definite immunological mechanism. Immediate DHRs occur within the first hour after the administration of a new treatment course, whereas nonimmediate DHRs occur beyond 1 h after the initial drug administration. 8
Another explanation for hypersensitivity reactions to paracetamol is its pharmacological effect of cyclooxygenase-1 inhibition, which is the most common mechanism. Majority of suspected paracetamol reactions occur in conjunction with nonsteroidal anti-inflammatory drug (NSAID) intolerance. The most common DHRs to analgesics are caused by NSAIDs. These occur in ∼0.6%–5.7% of the general population.4,6,9 The risk of anaphylaxis is low, as IgE-mediated paracetamol-induced hypersensitivity is rare, with only 6 pediatric cases reported in the literature. 2
There have been no reports of a paracetamol allergy with a proven IgE mechanism in pediatric patients because the skin tests were either not performed or negative. Six adult cases, described by Couto M, had positive skin tests. 2 Paramo BJ also published 2 female adult cases with positive SPT and OCT results. 10 A meta-analysis by Gabrielli S demonstrated that the prevalence of paracetamol hypersensitivity reaction among children undergoing OCT was 10.1%. 11 In a trial published by Sipahi Cimen, 1 pediatric patient tested positive through skin test, but the OCT was negative. 3 Among OCT-proven paracetamol-hypersensitive patients, neither SPT nor IDT was positive. 3 Skin tests and OCTs are rarely evaluated concomitantly. 3 Therefore, this is likely the first publication on a paracetamol allergy with a proven mediated IgE mechanism in a pediatric patient, as this concomitant evaluation was carried out.
The authors advertise that this study was carried out a few years ago, and Figs. 1 and 2 are the only imaging source obtained in that moment.
Conclusions
During the follow-up, patients with confirmed paracetamol hypersensitivity should be educated about paracetamol-containing formulation avoidance and alternative drugs. Cross-intolerance to NSAIDs was observed among 25% of patients with paracetamol hypersensitivity. Conversely, among patients with NSAID hypersensitivity, only 3% also reacted to paracetamol.1,2,12,13 Fortunately, our patient was a single reactor, and ibuprofen was a safe alternative for her.
Owing to the increase in hypersensitivity reactions to paracetamol, diagnostic confirmation of these DHRs is crucial. In our patient, the serum-specific IgE for paracetamol lacked utility because it yielded a false negative result. In previous studies, the paracetamol skin tests were either not performed or were negative. In this case, the IDT was positive. SPT and DPT were conducted to confirm the causative agent as the index of suspicion for IgE-mediated allergy to paracetamol was low. These tests confirmed the diagnosis and underlying pathophysiological mechanism. There is a relatively low risk of anaphylaxis to paracetamol, as IgE-mediated paracetamol-induced hypersensitivity is rare. Thus, this case report is valuable. We intend to underline the clinical benefits of diagnostic confirmation toward suspected DHRs in children, a particularly useful topic for pediatricians and pediatric allergists.
Key “take-home” Points
A DPT is the gold standard to diagnose or exclude hypersensitivity.
An IgE-mediated paracetamol-induced hypersensitivity is very rare.
This is likely the first publication of an allergy to paracetamol with a proven mediated IgE mechanism, in pediatric age.
Toward a suspected DHR, a definitive diagnosis is required, to institute proper preventive measures.
The follow-up of a confirmed paracetamol hypersensitivity implies patient education about avoidance of any paracetamol-containing formulation, including combination products (eg, cold and cough medications) and clarification of available alternative drugs, namely NSAIDs.
Ethics/Consent Statement
Patient's proxy is informed of this submission and has also signed a consent to publication form, which is held by the treating institution. Informed parental consent was assured, within the scope of patient's diagnostic approach.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.