
Abstract
Background:
Although serum levels of squamous cell carcinoma antigen (SCCA) are elevated in atopic dermatitis (AD), their clinical utility has not been fully elucidated.
Methods:
Thirty-three cases of AD who admitted to our hospital were analyzed.
Results:
Baseline characteristics on admission were as follows: median age 19 months [interquartile range (IQR), 12–52 months], median objective severity scoring of atopic dermatitis (O-SCORAD) 19.2 (IQR, 4.2–36.0), and median serum SCCA levels 3.2 ng/mL (IQR, 2.1–6.8 ng/mL). O-SCORAD significantly correlated with serum SCCA levels (rs = 0.865, P < 0.001). In 9 cases whose information before and after treatment was available (median interval, 3 days; IQR 2–5 days), median serum SCCA levels significantly decreased from 8.0 to 2.0 ng/mL (P = 0.008) after the treatment.
Conclusions:
Serum levels of total SCCA rapidly declined in response to the treatment and could be used as a real-time biomarker in childhood AD.
Introduction
Atopic dermatitis (AD)
In addition to the activation of immune cells, Th2 cytokines also induce squamous cell carcinoma antigen (SCCA) from squamous cells. SCCA, a member of the ovalbumin serine protease inhibitor family, is physiologically involved in cell survival and growth, epithelial–mesenchymal transition, antiparasite defense, and inhibition of defense against tumors. 2 SCCA, originally identified as a marker for squamous cell carcinoma in adults, consists of 2 isoforms: SCCA1 and SCCA2.
Although serum levels of SCCA2 are reported to reflect the severity and some distinct phenotypes such as erythroderma or lichenification in AD patients,3,4 measurement of SCCA2 is not widely available. In contrast, studies on the relationship between serum total SCCA levels and AD are limited. 5 Furthermore, comparison of changes between serum total SCCA and serum TARC in a short-term treatment for AD has not been fully investigated. We report the clinical usefulness of serum SCCA levels for evaluating the severity and effect of treatment for childhood AD.
Materials and Methods
Thirty-three cases previously diagnosed as AD according to the Japanese guidelines for AD, 6 who admitted to our hospital for oral food challenge test (n = 17) or treatment of AD (n = 16) between April 2018 and March 2020, were enrolled in this study. Cases with infectious symptoms (e.g., fever) or psoriasis were excluded because they could influence serum SCCA levels. The severity of AD was evaluated by objective severity scoring of atopic dermatitis (O-SCORAD). Laboratory tests included complete blood count, serum lactate dehydrogenase (LDH), serum immunoglobulin (Ig)E, serum TARC, and SCCA. In 9 of 16 patients who admitted for the treatment of AD, laboratory examinations were performed both before (on admission) and after treatment (at discharge).
Serum SCCA levels were commercially measured by the chemiluminescent immunoassay method using ARCHITECT SCC® kit, BML, Inc., Tokyo, Japan (reference range <1.5 ng/mL). Serum levels of total IgE and house dust mite-specific IgE were measured by an ImmunoCAP system (Thermo Fisher Scientific, Inc., Tokyo, Japan). The treatment of AD consisted of skin care education, showering, and an application of both moisture ointment and topical glucocorticoids (GC) 3 times a day according to the Japanese guidelines for AD. 6
The significance of correlations was analyzed using Spearman's rank correlation coefficient test (rs). The significance of changes in values of O-SCORAD, TARC, and SCCA in each individual was analyzed using Wilcoxon's signed-rank test. All analyses were conducted using IBM SPSS statistical software (version 24.0), and P values <0.05 were considered to be significant. Informed consent was obtained from all the participants' parents. This study was approved by the ethics committee of KKR Sapporo Medical Center (no. 2019-5).
Results
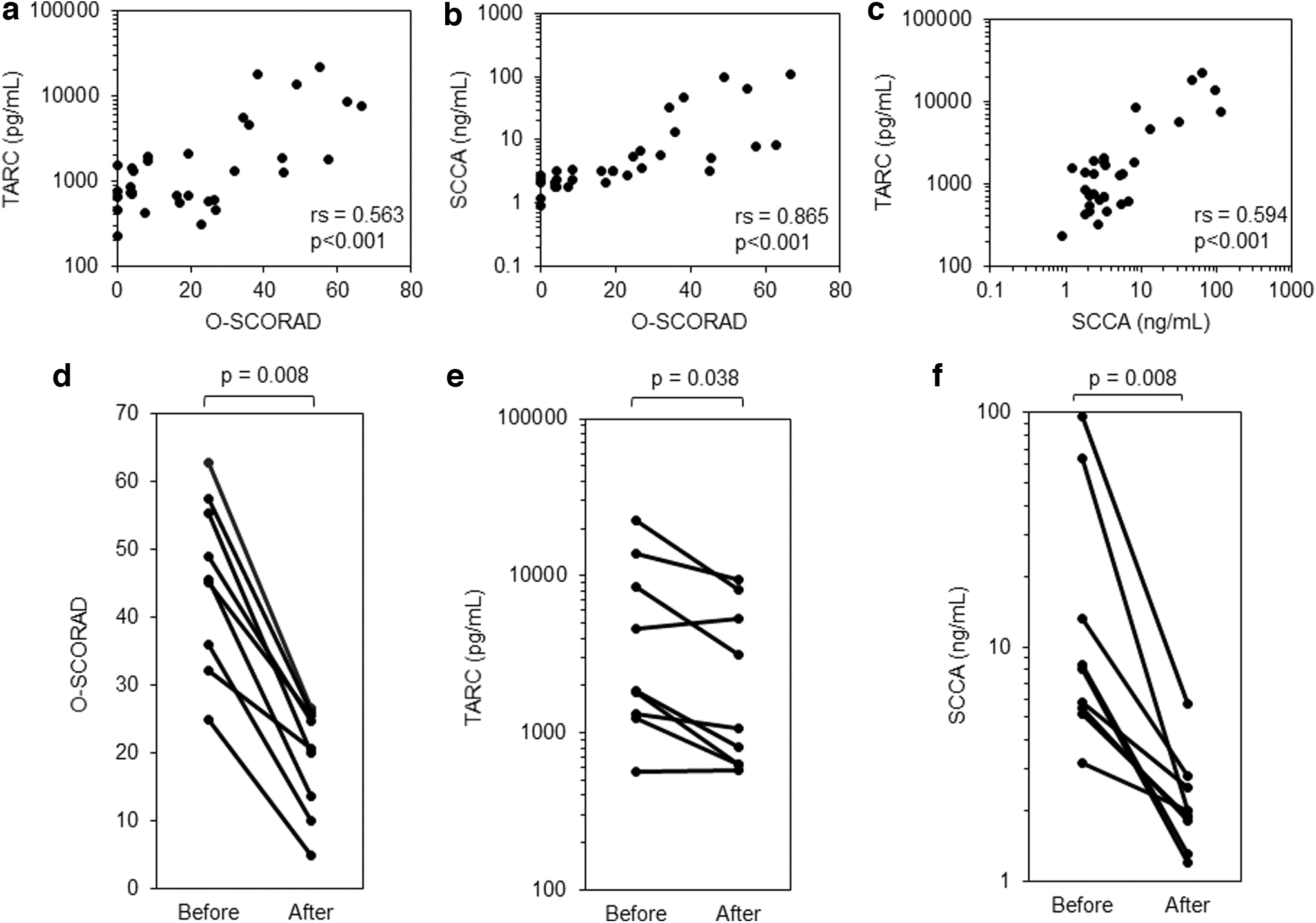
The patients' characteristics on admission were as follows: median age 19 months [interquartile range (IQR), 12–52 months], median O-SCORAD 19.2 (IQR, 4.2–36.0), median serum TARC levels 1,248 pg/mL (IQR, 643–1,914 pg/mL), and median serum SCCA levels 3.2 ng/mL (IQR, 2.1–6.8 ng/mL) (Table 1). In analysis of correlation between O-SCORAD and biomarkers, we found no significant correlation of O-SCORAD with total IgE or serum LDH levels (rs = 0.35, 0.095, respectively). In contrast, O-SCORAD significantly correlated with blood eosinophil counts (rs = 0.826, P < 0.001), serum TARC levels (rs = 0.563, P < 0.001; Fig. 1a), and serum SCCA levels (rs = 0.865, P < 0.001; Fig. 1b). Furthermore, there was a significant positive correlation between serum TARC and SCCA levels (rs = 0.594, P < 0.001; Fig. 1c).
Subject Profile (n = 33)
Reference ranges of the laboratory marker are as follows: HD-sIgE <0.35 kUA/L, LDH 0–1 years: <400 U/L, 2–5 years: <300 U/L, 6–12 years: <270 U/L, >13 years: <250 U/L, TARC 6–11 months: <1,367 pg/mL, 1 year <998 pg/mL, 2–15 years <743 pg/mL, SCCA <1.5 ng/mL.
HD, house dust mite; IQR, interquartile range; LDH, lactate dehydrogenase; O-SCORAD, objective severity scoring of atopic dermatitis; SCCA, squamous cell carcinoma antigen; sIgE, specific IgE antibody; TARC, thymus and activation-regulated chemokine.
We next examined changes in serum levels of TARC and SCCA before and after the treatment in 9 patients (median interval, 3 days; IQR 2–5 days). In all cases, O-SCORAD decreased after the treatment with topical GC, although its score did not improve completely (median score, from 45.5 to 20.5, P = 0.008; Fig. 1d). Median serum TARC levels significantly declined from 1,838 to 1,057 pg/mL after treatments, although they elevated in 2 cases (Fig. 1e). Median serum SCCA levels significantly decreased in all cases from 8.0 to 2.0 ng/mL (P = 0.008) after the treatment, reaching near the normal limit values (Fig. 1f).
Discussion
To our knowledge, only 1 report has suggested correlation between serum levels of total SCCA and the severity of childhood AD. 5 In this study, we showed that serum SCCA correlated with O-SCORAD, an internationally validated scoring system for the severity of AD, at a higher coefficient than correlation between TARC and O-SCORAD. Furthermore, serum SCCA levels rapidly declined after a short-term treatment with topical GC (median 3 days) before the complete improvement of O-SCORAD was achieved.
This discrepancy is possibly due to the short half-lives of serum SCCA that is estimated at ∼2.2 h 7 and much longer turnover cycle of the epidermal cells, 40–56 days. 8 Although precise half-lives of serum TARC levels are unknown, we have reported that they decrease from 3,308 pg/mL to lower than 100 pg/mL within a week after the onset of immune thrombocytopenic purpura, suggesting that TARC also has short half-lives. 9
However, our present data indicated that changes in serum TARC levels do not necessarily correlate with severity of AD in a short-term observation. SCCA is mainly produced by squamous cells, whereas TARC activates Th2 and has indirect effects on the development of dermatitis. In addition to the immunosuppressive and anti-inflammatory effects, GC has direct effects on the epithelial cells leading to skin atrophy. Thus, decline in serum SCCA levels after topical GC therapy may reflect both skin-targeted and Th2-mediated effects of GC. 10
A commercially available kit for SCCA (ARCHITECT SCC) detects the sum of both SCCA1 and SCCA2 with a higher sensitivity to SCCA111 and is widely used as a biomarker for various kinds of squamous cell carcinoma such as cervical cancer. Previous report has shown that patients with AD have predominant expression of SCCA2, whereas patients with cervical cancer predominantly express SCCA1. 12 Considering that SCCA1 is also increased in parallel with SCCA2 in AD patients, 12 it is reasonable that serum SCCA levels correlated with O-SCORAD in this age group because squamous cell carcinoma is quite rare in children.
Conclusions
Serum levels of total SCCA correlated with O-SCORAD at a higher coefficient than correlation between TARC and O-SCORAD, and rapidly declined in response to the treatment for AD. Serum levels of total SCCA may be superior to TARC as a real-time biomarker of AD during topical GC therapy.
Footnotes
Authors' Contributions
M.S. performed the statistical analysis and interpretation of the results, and wrote the article. I.K. designed and supervised the study. Y.O. and Y.T. critically reviewed the article. All authors contributed to data collection, and read and approved the final article.
Availability of Data and Material
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.