
Abstract
Background:
Drug provocation tests (DPTs) are the gold standard for the diagnosis of drug hypersensitivity reaction (DHR). To the best of our knowledge, there is no previous study reporting DPT-related anxiety levels in children and their parents. This study aimed to determine the difference in pre- and post-DPT anxiety levels of parents and children who were informed of the possibility of another DHR during the DPT, and to evaluate the relationship between parental psychological distress and anxiety levels.
Methods:
The study included children who underwent DPT in our clinic between July 1, 2019, and February 29, 2020, and accompanying parents who consented to participate. Age-appropriate State-Trait Anxiety Inventory scales were used to assess levels of state and trait anxiety in the patients and parents. The Symptom Checklist-90-Revised (SCL-90-R) was used to screen for psychological symptoms in parents.
Results:
Data were collected from the parents of 69 children who underwent DPTs. The patients' median age was 7.28 (interquartile range: 4.52–10.06) and their parents' mean age was 35.28 ± 5.38 years. Anxiety-related data were collected from 21 pediatric patients. The children and parents had higher state anxiety scores before DPT compared to after DPT. There was a positive correlation between the parents' trait anxiety and pre-DPT state anxiety scores. In addition, parental pre-DPT state anxiety scores were positively correlated with SCL-90-R general severity index, somatization, anxiety, obsessive-compulsive, and depression subscale scores.
Conclusion:
The risk of allergic reaction in DPT may cause anxiety. A high level of parental anxiety before DPT, which gradually decreased after negative test results, was associated with history of drug-induced anaphylaxis in their children and high trait anxiety. Appropriate evaluation of patients and parents before DPT and providing detailed information may be important to reduce this anxiety.
Introduction
Adverse drug reactions are an important cause of morbidity and mortality, leading to increased health costs and prolonged hospitalization. 1 An estimated 6%–10% of adverse drug reactions are due to hypersensitivity mechanisms.2,3 The prevalence of drug hypersensitivity reactions (DHRs) is reported to be higher than 7% in the general population. 4
In 1 study, the rate of immediate drug hypersensitivity among school children was 7.87% according to parents' reports, while this rate decreased to 0.11% after diagnostic workup. 5 This demonstrates the importance of confirming or ruling out the diagnosis of DHR through a detailed allergological workup, which includes standardized questionnaires recommended by the European Network for Drug Allergy (ENDA), 6 in vivo/in vitro tests for suspect drugs,7,8 and drug provocation tests (DPTs). 9 DPT is the gold standard for DHR diagnosis.10–12 However, it carries the risk of causing an allergic reaction of unpredictable severity. In rare cases, reactions may be more severe than the index reaction. 13
Children and parents with previous drug reaction experiences may feel anxiety about having a similar experience during DPT. Soyyiğit et al. reported in adults that the mean visual analog scale anxiety scores were higher before DPTs than those measured afterward. 14 Losappio et al. also reported a strong and significant correlation between depression/anxiety symptoms assessed before DPT and development of a placebo reaction during DPT. 15 To the best of our knowledge, there is no previous study reporting DPT-related anxiety levels in children and their parents. The level of anxiety in both parent and child may also be influenced by the presence of psychological distress in the parents.
This study aimed to determine the difference between pre- and post-DPT anxiety levels in parents and children who were informed of the possibility of a DHR during DPT, and to evaluate the relationship between parental symptoms of psychological distress and anxiety levels.
Methods
The study included children who underwent DPTs for diagnostic purposes or to detect alternative drugs in our pediatric allergy and immunology clinic between July 1, 2019, and February 29, 2020, and accompanying parents who consented to participate. The local ethics committee approved the study design and protocols (no: 2019-193). Written informed consent was obtained from the patients' parents.
Patients who had a history of suspected drug allergy according to the standardized ENDA questionnaire 6 were included. The suspect drug, spectrum and timing of symptoms, and list of concomitant medications were recorded. Coexisting chronic and allergic diseases in the patient and family history of drug allergy and other allergic diseases were recorded. In addition, the accompanying parent's age, education level, and any chronic/allergic/psychiatric disease were recorded.
All DPTs were conducted in strict accordance with the ENDA guidelines. 16 To confirm DHRs, DPT was performed with the suspect drug. To identify alternative drug in patients with DHRs to antibiotics, DPT was performed with a drug selected from a structurally different group. 17 In patients with DHRs to nonsteroidal anti-inflammatory drugs (NSAIDs), DPT was performed using weak COX-1 inhibitors and preferential COX-2 inhibitors, such as nimesulide/meloxicam and weak COX-1 inhibitor such as paracetamol. 18 DPT results were considered positive if any objective sign or symptom was documented.
Assessment of child anxiety
The State-Trait Anxiety Inventory for Children (STAIC) was used to assess the state and trait anxiety levels in pediatric patients 8–18 years of age. The validity and reliability study of the Turkish version was performed by Özusta. 19 The STAIC state anxiety subscale (STAIC-S) measures current anxiety using 20 items asking pediatric patients how they feel at the present time, while the trait subscale (STAIC-T) has 20 items that are used to understand how pediatric patients generally feel and to measure individual differences in anxiety tendencies. Response options include hardly ever, sometimes, and often.19,20 Higher scores indicate a higher level of anxiety. As with the parents, children who agreed to participate completed the STAIC-S both before and after the DPT and the STAIC-T once before the DPT.
Assessment of parental anxiety
The STAI was used to assess state and trait anxiety levels in the patients' parents. The test-retest reliability coefficients in the initial development study ranged between 0.31 and 0.86 at intervals ranging between 1 hour and 104 days. 21 The validity and reliability study of the Turkish version was performed by Oner and Le Compte. 22
Parents who agreed to participate in the study completed the STAI state anxiety subscale (STAI-S) before and after DPT. The STAI-S consists of 20 items regarding feelings of subjective tension, nervousness, anxiety, and activation/arousal “right now,” rated by selecting the response of not at all, somewhat, moderately so, or very much so. The trait anxiety subscale (STAI-T) was completed before DPT. It consists of 20 items regarding anxiety tendencies independent of the current situation. Items evaluate the general frequency of emotions with response options of almost never, sometimes, often, and almost always.21,22 Higher scores indicate a higher level of anxiety.
Assessment of parental psychological distress
Parents were screened for psychological symptoms using the Symptom Checklist-90-Revised (SCL-90-R). SCL-90-R is a 90-item tool that has been adapted into Turkish. The respondent rates to what degree each symptom has bothered them in the last week as not at all, a little, somewhat, quite a bit, or extremely. Scores are obtained in the subscales of anxiety, depression, interpersonal sensitivity, phobic anxiety, obsessive-compulsive, hostility, paranoid ideation, psychoticism, and somatization, and a general severity index (GSI) can be calculated as a summary score. GSI values over 1 indicate psychological distress.23,24
Statistical methods
Statistical analyses were performed using SPSS version 22 (IBM Corp, Armonk, NY). Data were reported as number and percentage for nominal variables and as mean and SD or median and interquartile range (IQR) for continuous variables. Chi-square (χ 2 ) test was used for comparisons of nonparametric data, and independent-samples t test for normally distributed continuous data. Spearman/Pearson correlation analyses were employed to evaluate the relationships between parameters. Linear regression modeling was used to evaluate parameters that may affect parental STAI-S scores before DPT. Results with P values <0.05 were considered statistically significant.
Results
The study included 69 pediatric patients who underwent DPT and whose parents agreed to participate. Anxiety-related data were collected from all 69 parents and from 21 patients who were old enough to be assessed with the STAIC (>8 years) and agreed to complete the questionnaire.
The median age of patients was 7.28 (IQR: 4.52–10.06) years. Most patients (46/69, 66.7%) underwent DPT due to history of suspected reaction to antibiotics, and urticaria and/or angioedema was the most common initial symptom (45/69, 65.2%) (Table 1). Family history of drug allergy was present in 19 cases.
Characteristics of Patients, Features of Index Reactions, and Allergic Diseases of Children
IQR, interquartile range; NSAID, nonsteroidal anti-inflammatory drug.
DPT was performed in 66 of the 69 patients to diagnose drug allergy and to identify an alternative agent for other 3 patients. Five patients developed reactions during DPT. Three of these patients had urticaria, 1 had angioedema, and 1 patient vomited during DPT.
Fifteen patients (21.7%) had previously undergone 1 or more DPTs and 3 patients had a history of previous positive DPT. One of those patients had undergone DPT for 2 suspect NSAIDs and had a positive DPT with one of them; this time, the patient had a negative result with another drug. Another patient had a previous positive DPT result with a suspect NSAID and this time had a negative DPT result with an alternative drug. The other patient had a previous positive DPT result with acetyl salicylic acid and this time a negative DPT result with amoxicillin-clavulanate.
Patient anxiety levels
The mean age of the 21 patients who completed STAIC was 12.5 ± 3.5 years. Seven patients had an allergic disease, 3 patients had a chronic comorbidity, and 2 patients had both allergic disease and a comorbid chronic and/or psychiatric disease.
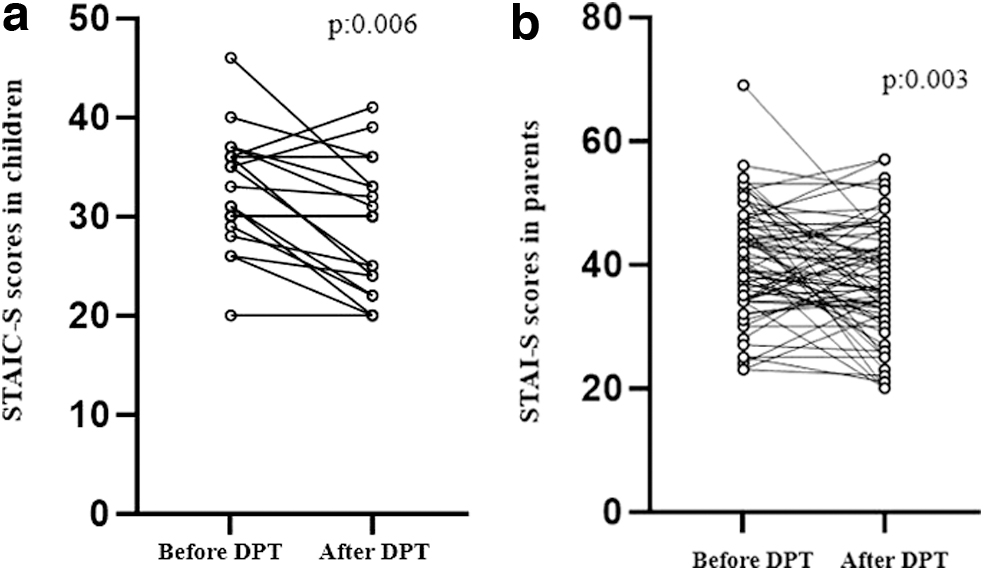
The median STAIC-T score was 35 (IQR: 27–39). The patients' STAIC-S scores were higher before DPT (median: 31; IQR: 29.5–36) than after DPT (median: 30, IQR: 23–33) (P = 0.006) (Fig. 1a). Mean STAIC-S scores were similar when patients were compared according to history of anaphylaxis as the index reaction, suspect drug group (antibiotic, NSAID, other), and the presence of allergic and/or chronic disease (P = 0.822, P = 0.748, and P = 0.915, respectively).
Parental anxiety levels
The mean age of the 69 parents who agreed to participate in the study was 35.28 ± 5.38 years. Sixty-five (94%) were mothers and the rest were fathers of the patients. Twenty-four of the parents' children had a history of allergic disease. Thirty-eight of the parents themselves or a family member had allergic illness, history of psychiatric illness, and/or a chronic illness involving other systems. A total of 3 parents had psychiatric illness (anxiety disorder in 1, panic attacks in 1, and obsessive-compulsive disorder in 1 parent).
The parents' mean pre-DPT and post-DPT STAI-S scores were 40.77 ± 9 and 37.22 ± 9.18, respectively (P = 0.003) (minimal importance difference: 2.84) (Fig. 1b). Comparisons of parental anxiety scores according to DPT reaction revealed no significant difference between STAI-S scores before (median: 41, IQR: 29.5–45.5) and after DPT (median: 32, IQR: 21–51) in the 5 parents whose children developed reactions during DPT (P = 0.588). In contrast, there was a statistically significant decrease in anxiety from before (mean: 40.97 ± 9) to after DPT (mean: 37.38 ± 8.65) in the parents of the 64 children with no reaction during DPT (P = 0.007).
Mean pre-DPT STAI-S score was lower in parents graduated from primary school (39.35 ± 9.22) than in parents with higher education levels (42.14 ± 8.67), but this difference was not statistically significant (P = 0.2).
The parents' mean STAI-T score was 42.88 ± 7.43. Mean STAI-T score was higher among parents who had a history of allergic illness, history of psychiatric illness, and/or a chronic illness involving other systems in themselves, their spouse, or other children compared to those without, but the difference did not reach statistical significance (mean: 44.26 ± 7.25 versus mean: 41.19 ± 7.40; P = 0.088). There was a positive correlation between the parents' STAI-T score and pre-DPT STAI-S score (Pearson's r = 0.395, P = 0.001; Fig. 2).

Positive correlations of parents' pre-DPT STAI-S scores. DPT, drug provocation test; STAI-S, State-Trait Anxiety Inventory state anxiety subscale.
There was no significant difference in mean STAI-S scores before and after DPT among the parents of children older than 10 years (37.84 ± 9.9 and 38.11 ± 11.8, respectively), whereas the parents of children younger than 10 years had significantly higher mean STAI-S score before DPT (41.88 ± 8.5 versus 36.88 ± 8.1; P = 0.001). In addition, mean STAI-S scores were significantly higher before DPT among parents graduated from primary school (39.35 ± 9.22 versus 36.03 ± 8.92, respectively; P = 0.005), whereas there was no significant difference in mean STAI-S scores before and after DPT among parents with higher education level (42.14 ± 8.67 and 38.37 ± 9.4, respectively; P = 0.242).
The parents of children with anaphylaxis history also had a higher mean STAI-S score before DPT (mean: 47.44) compared to parents of children with other symptoms (mean: 39.77) (P = 0.016), and showed a decrease in STAI-S score after DPT (mean STAI-S score of the parents of children with anaphylaxis post-DPT: 37.89), although it was not statistically significant.
Linear regression analysis to evaluate parameters associated with pre-DPT STAI-S score showed that patient history of anaphylaxis with the drug (P = 0.009) and high parental STAI-T score (P = 0.002) were associated with parents' pre-DPT STAI-S scores (Table 2).
Evaluation of Parameters That May Affect Parental State-Trait Anxiety Inventory-State Anxiety Subscale Score Before Drug Provocation Test
The independent variables included in the model explain 22.1% of parental STAI-S score before DPT (dependent variable) (P = 0.03; adjusted R2 = 0.221; F = 3.411).
Formula: dependent variable = 19.239 + 8.247 × (patient history of anaphylaxis with the drug) +0.450 × parental STAI-T score.
CI, confidence interval; DPT, drug provocation test; STAI, State-Trait Anxiety Inventory; STAI-T, STAI trait anxiety subscale; STAI-S, STAI state anxiety subscale.
Parental psychological symptoms and relationship with anxiety levels
The parents' median SCL-90-R subscale scores are shown in Table 3. Parental pre-DPT STAI-S scores were found to be positively correlated with GSI and somatization, anxiety, obsessive-compulsive, and depression subscale scores (Fig. 2). The strongest correlation was with the depression subscale.
Symptom Checklist-90-Revised Results and Correlation with State-Trait Anxiety Inventory-Trait Anxiety Subscale Results
IQR, interquartile range; SCL-90-R, Symptom Checklist-90 Revised; STAI-T, State-Trait Anxiety Inventory-trait anxiety subscale.
GSI was higher than 1 in 19 parents and less than 1 in the other 50 parents. GSI results were consistent with STAI-T results. Mean STAI-T score was significantly higher among parents with GSI higher than 1 compared to those with lower than 1 (48.42 versus 40.78, P < 0.001). Furthermore, parents with a GSI higher than 1 on the SCL-90-R reported significantly higher anxiety than those with GSI lower than 1, both before DPT (45.79 versus 38.86; P = 0.003) and after DPT (40.79 versus 35.86; P = 0.045). In addition, correlations between SCL-90-R subscale and STAI-T scores were detected (Table 3).
Discussion
To our knowledge, this is the first study to show that DPTs can cause anxiety in pediatric patients and their parents and to evaluate factors associated with this anxiety. We evaluated 21 children and 69 parents with the STAI and found that the children had higher state anxiety scores before DPT compared to after DPT. We also observed a statistically significant decrease in parental state anxiety from pre- to post-DPT. Parents who had graduated from primary school and had children younger than 10 years reported higher levels of anxiety before DPT than after DPT. There was also a positive correlation between the parents' anxiety levels and their symptoms of psychological distress.
Children who experience an allergic reaction and parents who witness their child have an allergic reaction often describe it as a negative, frightening experience. It is not surprising that patients who have experienced DHRs are anxious, as reactions ranging from mild symptoms to life-threatening anaphylaxis may recur after drug intake. In 1 study, among patients with drug allergy, asthma, and allergic rhinitis, the group of patients who had drug allergy had the highest number of psychological disorders. 25
Like the presence of drug allergy, the possibility of having a reaction during a DPT may also cause anxiety. In a previous study evaluating DPT-related anxiety in adults, Soyyiğit et al. showed that adults experienced similar anxiety for themselves. 14 In our study, the anxiety levels of patients and parents were higher before DPT and decreased afterward. Moreover, although the level of state anxiety did not differ before and after DPT in the parents of 5 patients who had a reaction during DPT, the parents of the 64 patients whose DPT induced no reaction showed a statistically significant decrease in anxiety scores after DPT. The higher anxiety before DPT in the latter group may be related to their previous experience of witnessing their child's DHR and the risk of experiencing this again during DPT.
This is consistent with our findings that patients who did not develop a reaction during DPT showed a marked reduction in anxiety score after the test, and that state anxiety levels before DPT were higher in parents of children who had anaphylactic reactions than in parents whose children had other symptoms.
In a study that aimed to determine the value of the minimal importance difference for anxiety and depression questionnaires after an intervention aimed at increasing daily physical activity in smokers, the minimal importance difference was calculated as 10. 26 In our study, it was calculated as 2.84 during the evaluation of the effect of provocation on anxiety in parents. However, the specific characteristics of the patient groups, their cultures, and the reasons for participating in the study are different in both studies, and this value may be affected by these characteristics. Calculation of the minimal importance difference value is important for psychiatric studies. Unfortunately, we do not have results produced from studies in Turkey, including frequently used scales.
Although there was no statistically significant difference in pre-DPT anxiety levels, parents with children younger than 10 years were also found to have higher anxiety before DPT than after DPT. We encountered no similar data in our review of the literature, nor does our study include any data related to factors that may be responsible for this phenomenon. The anxiety of parents with children older than 10 years may be slower to subside compared to parents with younger children.
This result was found to be similar to the comparison of mean pre-DPT and post-DPT STAI-S scores of parents who graduated from high school and university. If this result is corroborated in subsequent studies, it may be useful to provide additional information before DPT to parents with higher education levels and those with children older than 10 years to alleviate their anxiety. New studies that can evaluate causality are also needed for a better understanding of this subject.
In our study, the SCL-90-R was used to assess parents' psychological distress. GSI results were found to be consistent with STAI-T anxiety results. Parents with a GSI higher than 1 on the SCL-90-R also had higher pre-DPT and post-DPT STAI-S scores than parents with fewer psychological symptoms. Patients and parents with high anxiety levels in general have the potential to be more anxious about DPTs. While performing DPT on these patients, it may be necessary to give detailed information about DPTs to them and their families to create a more positive testing environment. In addition, more psychological support may be required from their physicians. Patients who need DPT for HR diagnosis and their parents may experience different anxiety than other patients and parents undergoing DPT. Our study was not designed to evaluate this difference, which is a limitation of this research.
Although there was no significant difference in the statistical analyses, parents who had a history of allergic illness, history of psychiatric illness, and/or a chronic illness involving other systems in themselves, their spouse, or other children tended to have higher trait anxiety scores than those without. In addition, the parents of children with history of anaphylaxis had higher mean state anxiety score before DPT compared to parents of children with other symptoms. This indicates that history and reaction patterns in the patient should be taken into consideration when informing patients and their families about the test.
STAI-S scores were evaluated immediately after DPT. However, it should be considered that these anxiety scores may change over time. A previous study conducted in our clinic showed that of 163 patients with negative DPT, 38 of them still did not use the drug because they or their doctor were afraid of a DHR. 27 In another study conducted in our clinic, 19 of 143 contacted patients who had a negative DPT with NSAIDs did not use the drug again due to fear. 28 According to these data, although post-DPT anxiety scores are low in patients with a negative result, they may still be reluctant to use the drug in question. Further studies are needed to compare parents' anxieties about post-DPT drug use in the long term.
In conclusion, DPTs carry the risk of causing an allergic reaction with a severity that cannot be reliably predicted, which can cause anxiety in pediatric patients and their parents. This is more common in parents with high trait anxiety and those whose children have a history of drug-induced anaphylaxis. We recommend clinicians ask children and parents to rate how anxious they generally feel on a simple 1 to 10 scale before DPT to gain insight into their trait anxiety level and allow the provision of more detailed information to those who may have high trait anxiety. Additional psychological support and creating a more positive testing environment may be important for these patients and parents. Reducing the anxiety levels of families after DPT, especially if there was no reaction, may help prevent drug avoidance in the future.
Footnotes
Authors' Contributions
All the authors reviewed it critically for important intellectual content and agree to be accountable for all aspects of the work related to its accuracy or integrity.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.